Glucose management for people with type 2 diabetes mellitus is essential but challenging due to the multi-factored and chronic disease nature of diabetes. To control glucose levels in a safe range and lessen abnormal glucose variability efficiently and economically, an intelligent prediction of glucose is demanding. A glucose trajectory prediction system based on subcutaneous interstitial continuous glucose monitoring data and deep learning models for ensuing glucose trajectory was constructed, followed by the application of personalised prediction models on one participant with type 2 diabetes in a community. The predictive accuracy was then assessed by RMSE (root mean square error) using blood glucose data. Changes in glycaemic parameters of the participant before and after model intervention were also compared to examine the efficacy of this intelligence-aided health care. Individual Recurrent Neural Network model was developed on glucose data, with an average daily RMSE of 1.59 mmol/L in the application segment. In terms of the glucose variation, the mean glucose decreased by 0.66 mmol/L, and HBGI dropped from 12.99 × 102 to 9.17 × 102. However, the participant also had increased stress, especially in eating and social support. Our research presented a personalised care system for people with diabetes based on deep learning. The intelligence-aided health management system is promising to enhance the outcome of diabetic patients, but further research is also necessary to decrease stress in the intelligence-aided health management and investigate the stress impacts on diabetic patients.
Citation: Lingmin Lin, Kailai Liu, Huan Feng, Jing Li, Hengle Chen, Tao Zhang, Boyun Xue, Jiarui Si. Glucose trajectory prediction by deep learning for personal home care of type 2 diabetes mellitus: modelling and applying[J]. Mathematical Biosciences and Engineering, 2022, 19(10): 10096-10107. doi: 10.3934/mbe.2022472
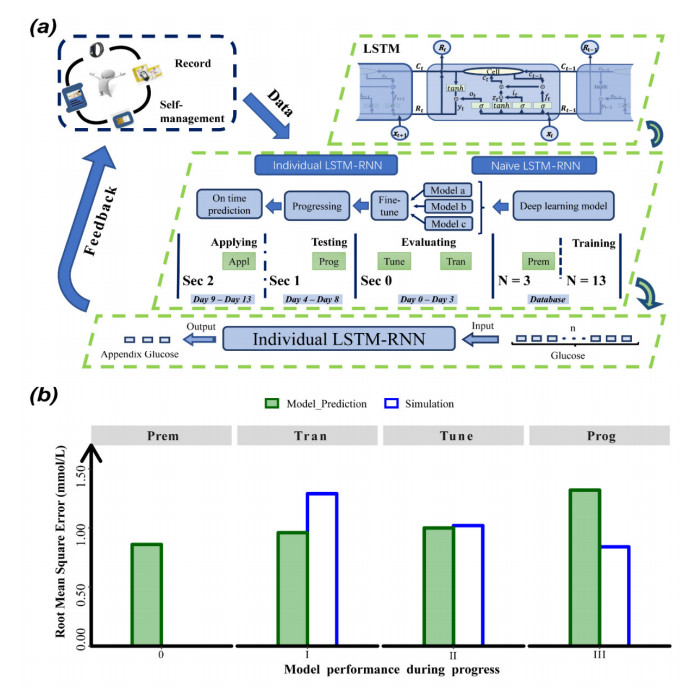
Glucose management for people with type 2 diabetes mellitus is essential but challenging due to the multi-factored and chronic disease nature of diabetes. To control glucose levels in a safe range and lessen abnormal glucose variability efficiently and economically, an intelligent prediction of glucose is demanding. A glucose trajectory prediction system based on subcutaneous interstitial continuous glucose monitoring data and deep learning models for ensuing glucose trajectory was constructed, followed by the application of personalised prediction models on one participant with type 2 diabetes in a community. The predictive accuracy was then assessed by RMSE (root mean square error) using blood glucose data. Changes in glycaemic parameters of the participant before and after model intervention were also compared to examine the efficacy of this intelligence-aided health care. Individual Recurrent Neural Network model was developed on glucose data, with an average daily RMSE of 1.59 mmol/L in the application segment. In terms of the glucose variation, the mean glucose decreased by 0.66 mmol/L, and HBGI dropped from 12.99 × 102 to 9.17 × 102. However, the participant also had increased stress, especially in eating and social support. Our research presented a personalised care system for people with diabetes based on deep learning. The intelligence-aided health management system is promising to enhance the outcome of diabetic patients, but further research is also necessary to decrease stress in the intelligence-aided health management and investigate the stress impacts on diabetic patients.

| [1] |
C. Bommer, E. Heesemann, V. Sagalova, J. Manne-Goehler, R. Atun, T. Bärnighausen, et al., The global economic burden of diabetes in adults aged 20–79 years: a cost-of-illness study, Lancet Diabetes Endocrinol., 5 (2017), 423–430. https://doi.org/10.1016/S2213-8587(17)30097-9 doi: 10.1016/S2213-8587(17)30097-9

|
| [2] |
B. Zhou, Y. Lu, K. Hajifathalian, J. Bentham, M. Cesare, G. Danaei, et al., Worldwide trends in diabetes since 1980: a pooled analysis of 751 population-based studies with 4.4 million participants, Lancet, 387 (2016), 1513–1530. https://doi.org/10.1016/S0140-6736(16)00618-8 doi: 10.1016/S0140-6736(16)00618-8
|
| [3] |
M. E. Murphy, M. Byrne, R. Galvin, F. Boland, T. Fahey, S. M. Smith, et al., Improving risk factor management for patients with poorly controlled type 2 diabetes: a systematic review of healthcare interventions in primary care and community settings, BMJ Open, 7 (2017), e015135. https://doi.org/10.1136/bmjopen-2016-015135 doi: 10.1136/bmjopen-2016-015135
|
| [4] |
V. Ponzo, L. Gentile, R. Gambino, R. Rosato, I. Cioffi, N. Pellegrini, et al., Incidence of diabetes mellitus, cardiovascular outcomes and mortality after a 12-month lifestyle interven-tion: a 9-year follow-up, Diabetes Metab., 44 (2018), 449–451. https://doi.org/10.1016/j.diabet.2018.04.008 doi: 10.1016/j.diabet.2018.04.008
|
| [5] |
J. Kropff, P. Choudhary, S. Neupane, K. Barnard, S. C. Bain, C. Kapitza, et al., Accuracy and longevity of an implantable continuous glucose sensor in the PRECISE study: a 180-Day, prospective, multicenter, pivotal trial, Diabetes Care, 40 (2017), 63–68. https://doi.org/10.2337/dc16-1525 doi: 10.2337/dc16-1525
|
| [6] |
G. Hinton, Deep learning-a technology with the potential to transform health care, JAMA, 320 (2018), 1101–1102. https://doi.org/10.1001/jama.2018.11100 doi: 10.1001/jama.2018.11100
|
| [7] | Q. Sun, M. V. Jankovic, L. Bally, S. G. Mougiakakou, Predicting blood glucose with an LSTM and Bi-LSTM based deep neural network, in 2018 14th Symposium on Neural Networks and Applications (NEUREL), (2018), 1–5. https://doi.org/10.1109/NEUREL.2018.8586990 |
| [8] |
Y. Zheng, S. H. Ley, F. B. Hu, Global aetiology and epidemiology of type 2 diabetes mellitus and its complications, Nat. Rev. Endocrinol., 14 (2018), 88–98. https://doi.org/10.1038/nrendo.2017.151 doi: 10.1038/nrendo.2017.151
|
| [9] |
K. Greff, R. K. Srivastava, J. Koutnik, B. R. Steunebrink, J. Schmidhuber, LSTM: a search space odyssey, IEEE Trans. Neural Networks Learn. Syst., 28 (2017), 2222–2232. https://doi.org/10.1109/TNNLS.2016.2582924 doi: 10.1109/TNNLS.2016.2582924
|
| [10] |
T. Danne, R. Nimri, T. Battelino, R. M. Bergenstal, K. L. Close, J. H. DeVries, et al., International consensus on use of continuous glucose monitoring, Diabetes Care, 40 (2017), 1631–1640. https://doi.org/10.2337/dc17-1600 doi: 10.2337/dc17-1600
|
| [11] | S. Mirshekarian, R. Bunescu, C. Marling, F. Schwartz, Using LSTMs to learn physiological models of blood glucose behaviour, in 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), (2017), 2887–2891. https://doi.org/10.1109/EMBC.2017.8037460 |
| [12] |
M. Munoz-Organero, Deep physiological model for blood glucose prediction in T1DM patients, Sensors, 20 (2020), 3896. https://doi.org/10.3390/s20143896 doi: 10.3390/s20143896
|
| [13] |
M. F. Rabby, Y. Tu, M. I. Hossen, I. Lee, A. S. Maida, X. Hei, Stacked LSTM based deep recurrent neural network with kalman smoothing for blood glucose prediction, BMC Med. Inf. Decis. Making, 21 (2021), 101. https://doi.org/10.1186/s12911-021-01462-5 doi: 10.1186/s12911-021-01462-5
|
| [14] |
T. Zhu, K. Li, P. Herrero, P. Georgiou, Deep learning for diabetes: a systematic review, IEEE J. Biomed. Health. Inf., 25 (2021), 2744–2757. https://doi.org/10.1109/JBHI.2020.3040225 doi: 10.1109/JBHI.2020.3040225
|
| [15] |
S. Ellahham, Artificial intelligence: the future for diabetes care, Am. J. Med., 133 (2020), 895–900. https://doi.org/10.1016/j.amjmed.2020.03.033 doi: 10.1016/j.amjmed.2020.03.033
|
| [16] |
Q. Pham, A. Gamble, J. Hearn, J. A. Cafazzo, The need for ethnoracial equity in artificial intelligence for diabetes management: review and recommendations, J. Med. Internet Res., 23 (2021), e22320. https://doi.org/10.2196/22320 doi: 10.2196/22320
|
| [17] | A. Radford, L. Metz, S. Chintala, Unsupervised representation learning with deep convolutional generative adversarial networks, preprient, arXiv: 1511.06434. |
| [18] | J. Ba, D. P. Kingma, Adam: a method for stochastic optimization, preprient, arXiv: 1412.6980. |
| [19] | Y. Baştanlar, M. Ozuysal, Introduction to machine learning, in miRNomics: MicroRNA Biology and Computational Analysis, 105–128. https://doi.org/10.1007/978-1-62703-748-8_7 |
| [20] |
M. Nguyen, J. Han, E. K. Spanakis, B. P. Kovatchev, D. C. Klonoff, A review of continuous glucose monitoring-based composite metrics for glycemic control, Diabetes Technol. Ther., 22 (2020), 613–622. https://doi.org/10.1089/dia.2019.0434 doi: 10.1089/dia.2019.0434
|
| [21] |
M. F. Huang, M. Courtney, H. Edwards, J. McDowell, Validation of the chinese version of the problem areas in diabetes (PAID-C) scale, Diabetes Care, 33 (2010), 38–40. https://doi.org/10.2337/dc09-0768 doi: 10.2337/dc09-0768
|
| [22] |
B. P. Kovatchev, Metrics for glycaemic control - from HbA1c to continuous glucose monitoring, Nat. Rev. Endocrinol., 13 (2017), 425–436. https://doi.org/10.1038/nrendo.2017.3 doi: 10.1038/nrendo.2017.3
|
| [23] |
E. K. Kim, S. H. Kwak, H. S. Jung, B. K. Koo, M. K. Moon, S. Lim, et al., The effect of a smartphone-based, patient-centered diabetes care system in patients with type 2 diabetes: a randomized, controlled trial for 24 weeks, Diabetes Care, 42 (2019), 3–9. https://doi.org/10.2337/dc17-2197 doi: 10.2337/dc17-2197
|
| [24] |
K. Li, J. Daniels, C. Liu, P. Herrero-Vinas, P. Georgiou, Convolutional recurrent neural networks for glucose prediction, IEEE J. Biomed. Health Inf., 24 (2019), 603–613. https://doi.org/10.1109/JBHI.2019.2908488 doi: 10.1109/JBHI.2019.2908488
|
| [25] |
J. M. M. Rumbold, M. O'Kane, N. Philip, B. K. Pierscionek, Big Data and diabetes: the applications of Big Data for diabetes care now and in the future, Diabetic Med., 37 (2020), 187–193. https://doi.org/10.1111/dme.14044 doi: 10.1111/dme.14044
|
| [26] |
S. Ashrafzadeh, O. Hamdy, Patient-driven diabetes care of the future in the technology era, Cell Metab., 29 (2019), 564–575. https://doi.org/10.1016/j.cmet.2018.09.005 doi: 10.1016/j.cmet.2018.09.005
|
| [27] |
L. Fisher, W. H. Polonsky, D. Hessler, Addressing diabetes distress in clinical care: a practical guide, Diabetic. Med., 36 (2019), 803–812. https://doi.org/10.1111/dme.13967 doi: 10.1111/dme.13967
|
| [28] |
D. Hessler, L. Fisher, R. E. Glasgow, L. A. Strycker, L. M. Dickinson, P. A. Arean, et al., Reductions in regimen distress are associated with improved management and glycemic control over time, Diabetes Care, 37 (2014), 617–624. https://doi.org/10.2337/dc13-0762 doi: 10.2337/dc13-0762
|
| [29] |
A. Reimer, A. Schmitt, D. Ehrmann, B. Kulzer, N. Hermanns, Reduction of diabetes-related distress predicts improved depressive symptoms: a secondary analysis of the DIAMOS study, PLoS One, 12 (2017), e0181218. https://doi.org/10.1371/journal.pone.0181218 doi: 10.1371/journal.pone.0181218
|
| [30] |
C. Ju, R. Shi, L. Yao, X. Ye, M. Jia, J. Han, et al., Effect of peer support on diabetes distress: a cluster randomized controlled trial, Diabetic Med., 35 (2018), 770–775. https://doi.org/10.1111/dme.13625 doi: 10.1111/dme.13625
|
| [31] |
A. A. Lee, J. D. Piette, M. Heisler, A. M. Rosland, Diabetes distress and glycemic control: the buffering effect of autonomy support from important family members and friends, Diabetes Care, 41 (2018), 1157–1163. https://doi.org/10.2337/dc17-2396 doi: 10.2337/dc17-2396
|

Figures(2) / Tables(2)

Lingmin Lin, Kailai Liu, Huan Feng, Jing Li, Hengle Chen, Tao Zhang, Boyun Xue, Jiarui Si. Glucose trajectory prediction by deep learning for personal home care of type 2 diabetes mellitus: modelling and applying[J]. Mathematical Biosciences and Engineering, 2022, 19(10): 10096-10107. doi: 10.3934/mbe.2022472







 DownLoad:
DownLoad: