Citation: Xiuli Wu, Xianli Shen, Linjuan Zhang. Solving the planning and scheduling problem simultaneously in a hospital with a bi-layer discrete particle swarm optimization[J]. Mathematical Biosciences and Engineering, 2019, 16(2): 831-861. doi: 10.3934/mbe.2019039

| [1] | X. Chen, Z. P. Fan, Z. W. Li, X. L. Han, X. Zhang and H. C. Jia, A two-stage method for member selection of emergency medical service, J. Comb. Optim., 30 (2015), 871–891. |
| [2] | B. Wang, X. B. Han, X. X. Zhang, and S. H. Zhang, Predictive-reactive scheduling for single surgical suite subject to random emergency surgery, J. Comb. Optim., 30 (2015), 949–966. |
| [3] | M. E. Bruni, P. Beraldi, and D. Conforti, A stochastic programming approach for operating theatre scheduling under uncertainty, Ima. J. Manage. Math., 26 (2015), 99–119. |
| [4] | Z. X. Zhao and X. P. Li, Scheduling elective surgeries with sequence-dependent setup times to multiple operating rooms using constraint programming, Oper. Res. Health. Car., 3 (2014), 160–167. |
| [5] | S. Neyshabouri and B. P. Berg, Two-stage robust optimization approach to elective surgery and downstream capacity planning, Eur. J. Oper. Res., 260 (2016), 21–40. |
| [6] | D. Min and Y. Yih, An elective surgery scheduling problem considering patient priority, Comput. Oper. Res., 37 (2010), 1091–1099. |
| [7] | A. Jebali and A. Diabat, A Chance-constrained operating room planning with elective and emergency cases under downstream capacity constraints, Comput. Ind. Eng., 114 (2017), 329–344. |
| [8] | M. Lamiri, X. L. Xie, A. Dolgui and F. Grimaud, A stochastic model for operating room planning with elective and emergency demand for surgery, Eur. J. Oper. Res., 185 (2008), 1026–1037. |
| [9] | A. Abedini, H. H. Ye and W. Li, Operating room planning under surgery type and priority constraints, Procedia. Manuf., 5 (2016), 15–25. |
| [10] | N. Dellaert and J. Jeunet, A variable neighborhood search algorithm for the surgery tactical planning problem, Comput. Oper. Res., 84 (2017), 1–10. |
| [11] | Y. Yang, B. Shen, W. Gao, Y. Liu and L. W. Zhong, A surgical scheduling method considering surgeons' preferences, J. Comb. Optim., 30 (2015), 1016–1026. |
| [12] | T. M. Range, R. M. Lusby and J. Larsen, A column generation approach for solving the patient admission scheduling problem, Eur. J. Oper. Res., 235 (2014), 252–264. |
| [13] | W. Xiang, J. Yin and G. Lim, An ant colony optimization approach for solving an operating room surgery scheduling problem, Comput. Ind. Eng., 85 (2015), 335–345. |
| [14] | A. Riise, C. Mannino and E. K. Burke, Modelling and solving generalised operational surgery scheduling problems, Comput. Oper. Res., 66 (2016), 1–11. |
| [15] | D. Duma and R. Aringhieri, An online optimization approach for the real time management of operating rooms, Oper. Res. Health. Car., 7 (2015), 40–51. |
| [16] | F. Guerriero and R. Guido, Operational research in the management of the operating theatre: A survey, Health. Car. Manage. Sci., 14 (2011), 89–114. |
| [17] | E. Demeulemeester, J. Beliën, B. Cardoen and M. Samudra, Operating room planning and scheduling, Eur. J. Oper. Res., 201 (2010), 921–932. |
| [18] | R. M'. Hallah and A. H. Al-Roomi, The planning and scheduling of operating rooms: A simulation approach, Comput. Ind. Eng., 78 (2014), 235–248. |
| [19] | R. Aringhieri, P. Landa, P. Soriano, E. Tànfani and A. Testi, A two level metaheuristic for the operating room scheduling and assignment problem, Comput. Oper. Res., 54 (2015), 21–34. |
| [20] | R. Guido and D. Conforti, A hybrid genetic approach for solving an integrated multi-objective operating room planning and scheduling problem, Comput. Oper. Res., 87 (2016), 270–282. |
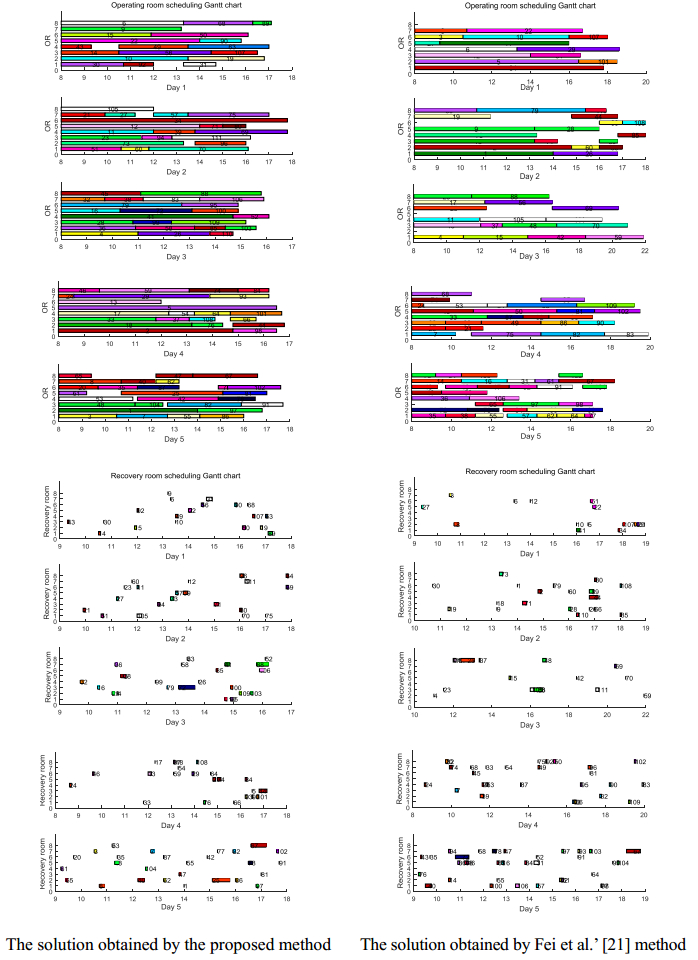
| [21] | H. Y. Fei, N. Meskens and C. B. Chu, A planning and scheduling problem for an operating theatre using an open scheduling strategy, Comput. Ind. Eng., 58 (2010), 221–230. |
| [22] | J. M. Molina-Pariente, V. Fernandez-Viagas and J. M. Framinan, Integrated operating room planning and scheduling problem with assistant surgeon dependent surgery durations, Comput. Ind. Eng., 82 (2015), 8–20. |
| [23] | P. Landa, R. Aringhieri, P. Soriano, E. Tànfani and A. Testi, A hybrid optimization algorithm for surgeries scheduling, Oper. Res. Health. Car., 8 (2016), 103–114. |
| [24] | A. J. Fong, M. Smith and A. Langerman, Efficiency improvement in the operating room, J. Surg. Res., 204 (2016), 371–383. |
| [25] | D. N. Pham and A. Klinkert, Surgical case scheduling as a generalized job shop scheduling problem, Eur. J. Oper. Res., 185 (2008), 1011–1025. |
| [26] | L. W. Zhong, S. C. Luo, L. D. Wu, L. Xu, J. H. Yang and G. C. Tang, A two-stage approach for surgery scheduling, J. Comb. Optim., 27 (2014), 545–556. |
| [27] | R. Burdett and E. Kozan,An integrated approach for scheduling health care activities in a hospital, Eur. J. Oper. Res., 264 (2017), 756–773. |
| [28] | A. Abedini, W. Li and H. H. Ye, An optimization model for operating room scheduling to reduce blocking across the perioperative process, Procedia. Manuf., 10 (2017), 60–70. |
| [29] | J. N. D. Gupta, Two-stage, hybrid flow shop scheduling problem, J. Oper. Res. Soc., 39 (1988), 359–364. |
| [30] | J. Q. Li, H. Y. Sang, Y. Y. Han, C. G. Wang and K. Z. Gao, Efficient multi-objective optimization algorithm for hybrid flow shop scheduling problems with setup energy consumptions, J. Cleaner. Prod., 181 (2018), 584–598. |
| [31] | J. Q. Li, Q. K. Pan and M. F. Tasgetiren, A discrete artificial bee colony algorithm for the multi-objective flexible job-shop scheduling problem with maintenance activities, Appl. Math. Model., 38 (2014), 1111–1132. |
| [32] | H. C. Liu, L. Gao and Q. K. Pan, A hybrid particle swarm optimization with estimation of distribution algorithm for solving permutation flowshop scheduling problem, Exp. Syst. Appl., 38 (2011), 4348–4360. |
| [33] | J. Q. Li, Q. K. Pan and F. T. Wang, A hybrid variable neighborhood search for solving the hybrid flow shop scheduling problem, Appl. Soft. Comput. J., 24 (2014), 63–77. |
| [34] | X. Y. Li and L. Gao, An effective hybrid genetic algorithm and tabu search for flexible job shop scheduling problem, Int. J. Prod. Econ., 174 (2016), 93–110. |
| [35] | S. Gao and C. G. Cao, Convergence analysis of particle swarm optimization algorithm, Sci. Technol. Eng., 4 (2008), 25–32. |
| [36] | M. A. Ghorbani, R. Kazempour, K. W. Chau and S. Shamshirband, Forecasting pan evaporation with an integrated Artificial Neural Network Quantum-behaved Particle Swarm Optimization model: A case study in Talesh, Northern Iran, Eng. Appl. Comput. Fluid. Mech., 12 (2018), 724–737. |
| [37] | J. Kennedy and R. C. Eberhart, Particle swarm optimization, Proc. IEEE. Int. Conf. Neural. Networks., 4 (1995), 1942–1948. |
| [38] | Q. K. Pan, W. H. Wang and J. Y. Zhu, Modified discrete particle swarm optimization algorithm for no-wait flow shop problem, Comput. Integr. Manuf. Syst., 13 (2007), 1127–1130. |
| [39] | X. L. Wu, S. D. Sun, J. J. Yu and H. F. Zhang, Research on multi-objective optimization for flexible job shop scheduling, Comput. Integr. Manuf. Syst., 12 (2006), 731–736. |
| [40] | M. J. Tessler, S. J. Kleiman and M. M. Huberman, A |
| [41] | M. Schuster, T. Standl, J. A. Wagner and J. Berger, Effect of different cost drivers on cost per anesthesia minute in different anesthesia subspecialties, Anesthesiology, 101 (2004), 1435–1443. |
| [42] | Y. Shi and R. C. Eberhart, Empirical study of particle swarm optimization, Proc. IEEE Congr. Evol. Comput., (1999), 1945–1950. |
| [43] | X. L. Wu and Y. J. Sun, A green scheduling algorithm for flexible job shop with energy-saving measures, J. Cleaner. Prod., 172 (2017), 3249–3264. |




Figures(15) / Tables(7)

Xiuli Wu, Xianli Shen, Linjuan Zhang. Solving the planning and scheduling problem simultaneously in a hospital with a bi-layer discrete particle swarm optimization[J]. Mathematical Biosciences and Engineering, 2019, 16(2): 831-861. doi: 10.3934/mbe.2019039







 DownLoad:
DownLoad: