To investigate the clinical epidemiological characteristics and occurrence of post-traumatic stress symptoms (PTSS) in patients with traumatic fractures, we sought to analyze the factors that influence the prognosis of a length of hospital stay (LOS) and provide valuable insights to prevent PTSS in fracture patients and improve their prognosis.
Inpatients with traumatic fractures were recruited from a third-class comprehensive general hospital in southwest China between November 2019 and October 2020. Case data of traumatic fracture patients were collected, and a questionnaire that included general information and basic fracture details was completed. The post-traumatic stress disorder Self-rating Scale was used to assess PTSS among the fracture inpatients.
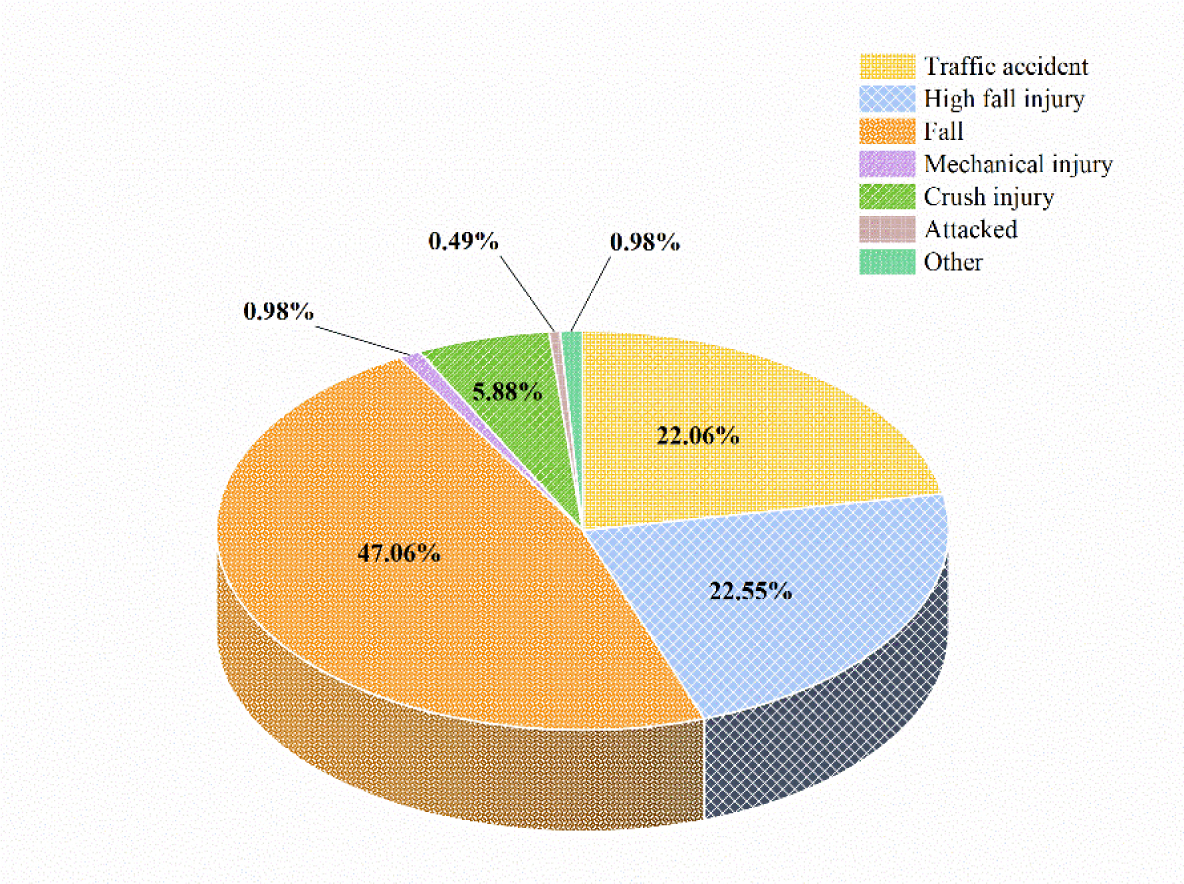
A total of 204 inpatients who experienced traumatic fractures were included in this study. Falls accounted for the largest proportion of traumatic fractures. A Cox's regression analysis revealed that serious injury [Hazard Ratio (HR) = 2.44, 95% Confidence Interval (CI): 1.33–4.46], critical illness during hospitalization (HR = 1.70, 95% CI: 1.13–2.54), and undergoing two surgeries (HR = 1.87, 95% CI: 1.20–2.93) were risk factors for longer LOS. Among the fracture patients, 30.39% exhibited positive PTSD symptoms, and physical activity during the fracture [Odds Ratio (OR) = 0.63, 95% CI: 0.45–0.88] and increased pain (OR = 3.34, 95% CI: 1.82–6.11) were identified as influencing factors.
Given the high detection rate of PTSS following traumatic fractures, it is crucial for relevant departments to implement targeted measures to protect high risk individuals. Furthermore, strengthening the care provided to the patients' physical and mental health is urgently needed to reduce the incidence of PTSS.
Citation: Guojia Qi, Xiu Dai, Xue Wang, Ping Yuan, Xiahong Li, Miao Qi, Xiuli Hu, Xiuquan Shi. Epidemiological characteristics of post-traumatic stress symptoms and its influence on length of hospital stay in inpatients with traumatic fractures in Zunyi, China[J]. AIMS Public Health, 2024, 11(3): 835-849. doi: 10.3934/publichealth.2024042
To investigate the clinical epidemiological characteristics and occurrence of post-traumatic stress symptoms (PTSS) in patients with traumatic fractures, we sought to analyze the factors that influence the prognosis of a length of hospital stay (LOS) and provide valuable insights to prevent PTSS in fracture patients and improve their prognosis.
Inpatients with traumatic fractures were recruited from a third-class comprehensive general hospital in southwest China between November 2019 and October 2020. Case data of traumatic fracture patients were collected, and a questionnaire that included general information and basic fracture details was completed. The post-traumatic stress disorder Self-rating Scale was used to assess PTSS among the fracture inpatients.
A total of 204 inpatients who experienced traumatic fractures were included in this study. Falls accounted for the largest proportion of traumatic fractures. A Cox's regression analysis revealed that serious injury [Hazard Ratio (HR) = 2.44, 95% Confidence Interval (CI): 1.33–4.46], critical illness during hospitalization (HR = 1.70, 95% CI: 1.13–2.54), and undergoing two surgeries (HR = 1.87, 95% CI: 1.20–2.93) were risk factors for longer LOS. Among the fracture patients, 30.39% exhibited positive PTSD symptoms, and physical activity during the fracture [Odds Ratio (OR) = 0.63, 95% CI: 0.45–0.88] and increased pain (OR = 3.34, 95% CI: 1.82–6.11) were identified as influencing factors.
Given the high detection rate of PTSS following traumatic fractures, it is crucial for relevant departments to implement targeted measures to protect high risk individuals. Furthermore, strengthening the care provided to the patients' physical and mental health is urgently needed to reduce the incidence of PTSS.

| [1] |
Hassanzadeh R, Farhadian M, Rafieemehr H (2023) Hospital mortality prediction in traumatic injuries patients: Comparing different SMOTE-based machine learning algorithms. BMC Med Res Methodol 23: 101. https://doi.org/10.1186/s12874-023-01920-w 
|
| [2] |
Li W, Cheng P, Liu Z, et al. (2023) Post-traumatic stress disorder and traumatic events in China: a nationally representative cross-sectional epidemiological study. Psychiatry Res 326: 115282. https://doi.org/10.1016/j.psychres.2023.115282
|
| [3] |
Chen W, Lv H, Liu S, et al. (2027) National incidence of traumatic fractures in China: A retrospective survey of 512 187 individuals. Lancet Glob Health 5: e807-e817. https://doi.org/10.1016/S2214-109X(17)30222-X
|
| [4] |
Fluck D, Lisk R, Yeong K, et al. (2023) Association of polypharmacy and anticholinergic burden with length of stay in hospital amongst older adults admitted with hip fractures: A retrospective observational study. Calcif Tissue Int 112: 584-591. https://doi.org/10.1007/s00223-023-01072-5
|
| [5] |
Huang BX, Wang YH, Wang HB, et al. (2023) Epidemiology and the economic burden of traumatic fractures in China: A population-based study. Front Endocrinol (Lausanne) 14: 1104202. https://doi.org/10.3389/fendo.2023.1104202
|
| [6] |
Manosroi W, Koetsuk L, Phinyo P, et al. (2023) Predictive model for prolonged length of hospital stay in patients with osteoporotic femoral neck fracture: A 5-year retrospective study. Front Med 9: 1106312. https://doi.org/10.3389/fmed.2022.1106312
|
| [7] |
Lv H, Chen W, Zhang T, et al. (2020) Traumatic fractures in China from 2012 to 2014: A National Survey of 512,187 individuals. Osteoporos Int 31: 2167-2178. https://doi.org/10.1007/s00198-020-05496-9
|
| [8] |
Kang KK, Ciminero ML, Parry JA, et al. (2021) The psychological effects of musculoskeletal trauma. J Am Acad Orthop Surg 29: e322-e329. https://doi.org/10.5435/JAAOS-D-20-00637
|
| [9] |
Wang X, Li X, Qi M, et al. (2022) Incidence of post-traumatic stress disorder in survivors of traumatic fracture: A systematic review and meta-analysis. Psychol Health Med 27: 902-916. https://doi.org/10.1080/13548506.2021.1957953
|
| [10] | (2013) American Psychiatric AssociationDiagnostic and statistical manual of mental disorders. Arlington, DC: American Psychiatric Association 30-80. |
| [11] |
Coloma-Carmona A, Carballo JL (2021) Predicting PTSS in general population during COVID-19 pandemic: The mediating role of health anxiety. J Affect Disord 294: 329-336. https://doi.org/10.1016/j.jad.2021.07.03
|
| [12] |
Chen K, Hynes KK, Dirschl D, et al. (2024) Depression, anxiety, and post-traumatic stress disorder following upper versus lower extremity fractures. Injury 55: 111242. https://doi.org/10.1016/j.injury.2023.11124
|
| [13] | Joseph NM, Benedick A, Flanagan CD, et al. (2020) Prevalence of posttraumatic stress disorder in acute trauma patients. OTA In 3: e056. https://doi.org/10.1097/OI9.000000000000005 |
| [14] | National Bureau of StatisticsThe sixth population census (2010). Available from: https://www.stats.gov.cn/sj/pcsj/rkpc/6rp/indexch.htm |
| [15] | Liu X, Ma D, Liu Q, et al. (1998) Development of the post-traumatic stress disorder self-rating sca leand its reliability and validity. Chin J Behav Med Sci : 14-17. |
| [16] |
Baker SP, O'Neill B, Haddon W, et al. (1974) The injury severity score: A method for describing patients with multiple injuries and evaluating emergency care. J Trauma 14: 187-196. https://doi.org/10.1097/00005373-197403000-00001
|
| [17] |
Baker S P, O'Neill B (1976) The injury severity score: An update. J Trauma 16: 882-885. https://doi.org/10.1097/00005373-197611000-00006
|
| [18] |
Hannula A, Miettinen L, Lampainen K, et al. (2023) Cost of surgical treatment for ulnar nerve entrapment in Finland, 2011–2015: A registry-based cost description study. BMJ Open 13: e068964. https://doi.org/10.1136/bmjopen-2022-068964
|
| [19] | Yuan H, Guo Q, Zhang Z, et al. (2023) Sex, age, role and geographic differences in traumatic spinal fractures caused by motor vehicle collisions: A multicentre retrospective study. Sci Re 13: 3712. https://doi.org/10.1038/s41598-023-30982-5 |
| [20] | Luo B (2022) Analysis of relevant influencing factors and intervention strategies for acute stress disorder in traumatic fractures. Inner Mongolia Med J 54: 1450-1453. |
| [21] |
Ren Y, Zhou Z, Cao D, et al. (2022) Did the integrated urban and rural resident basic medical insurance improve benefit equity in China?. Value Health 25: 1548-1558. https://doi.org/10.1016/j.jval.2022.03.007
|
| [22] | Audretsch CK, Siegemund A, Ellmerer A, et al. (2023) Sex differences in pelvic fractures-a retrospective analysis of 16 359 cases from the german trauma registry. Dtsch Arztebl Int 120: 221-222. https://doi.org/10.3238/arztebl.m2022.0402 |
| [23] |
Warren AM, Jones AL, Bennett M, et al. (2016) Prospective evaluation of posttraumatic stress disorder in injured patients with and without orthopaedic injury. J Orthop Trauma 30: e305-311. https://doi.org/10.1097/BOT.0000000000000623
|
| [24] |
Pozza DH, Azevedo LF, Castro Lopes JM (2021) Pain as the fifth vital sign-A comparison between public and private healthcare systems. PLoS On 16: e0259535. https://doi.org/10.1371/journal.pone.0259535
|
| [25] |
Kornfield SL, Lenze EJ, Rawson KS (2017) Predictors of posttraumatic stress symptoms and association with fear of falling after hip fracture. J Am Geriatr Soc 65: 1251-1257. https://doi.org/10.1111/jgs.14771
|
| [26] | Liu J, Chen L, Duan X, et al. (2019) Effect of early preoperative mobilization on rehabilitation of the elderly patients with hip fractures after operation. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi 33: 318-322. https://doi.org/10.7507/1002-1892.201809098 |
| [27] |
Sainsbury A, Seebass G, Bansal A, et al. (2005) Reliability of the Barthel Index when used with older people. Age Ageing 34: 228-232. https://doi.org/10.1093/ageing/afi063
|
| [28] |
Vlok M, Maloney T, Dilkes-Hall IE, et al. (2023) Reply to: Common orthopaedic trauma may explain 31,000-year-old remains. Nature 615: E15-E18. https://doi.org/10.1038/s41586-023-05757-7
|
| [29] |
Castillo RC, Carlini AR, Doukas WC, et al. (2021) Pain, depression, and PTSD following major extremity trauma among United States military serving in Iraq and Afghanistan: Results from the METALS Study. J Orthop Trauma 35: e96-e102. https://doi.org/10.1097/BOT.0000000000001921
|
| [30] |
Wallace M, Puryear A, Cannada LK (2013) An evaluation of posttraumatic stress disorder and parent stress in children with orthopaedic injuries. J Orthop Trauma 27: e38-41. https://doi.org/10.1097/BOT.0b013e318250c837
|
| [31] |
Lee CH, Choi CH, Yoon SY, et al. (2015) Posttraumatic stress disorder associated with orthopaedic trauma: A study in patients with extremity fractures. J Orthop Trauma 29: e198-202. https://doi.org/10.1097/BOT.0000000000000255
|
| [32] |
Kind S, Otis JD (2019) The interaction between chronic pain and PTSD. Curr Pain Headache Rep 23: 91. https://doi.org/10.1007/s11916-019-0828-3
|
| [33] |
Hildenbrand AK, Kassam-Adams N, Barakat LP, et al. (2020) Posttraumatic stress in children after injury the role of acute pain and opioid medication use. Pediatr Emerg Care 36: e549-e557. https://doi.org/10.1097/PEC.0000000000001404
|
| [34] |
Akhtar E, Ballew AT, Orr WN, et al. (2019) The prevalence of post-traumatic stress disorder symptoms in chronic pain patients in a tertiary care setting: A cross-sectional study. Psychosomatics 60: 255-262. https://doi.org/10.1016/j.psym.2018.07.012
|
Figures(1) / Tables(5)

Guojia Qi, Xiu Dai, Xue Wang, Ping Yuan, Xiahong Li, Miao Qi, Xiuli Hu, Xiuquan Shi. Epidemiological characteristics of post-traumatic stress symptoms and its influence on length of hospital stay in inpatients with traumatic fractures in Zunyi, China[J]. AIMS Public Health, 2024, 11(3): 835-849. doi: 10.3934/publichealth.2024042







 DownLoad:
DownLoad: