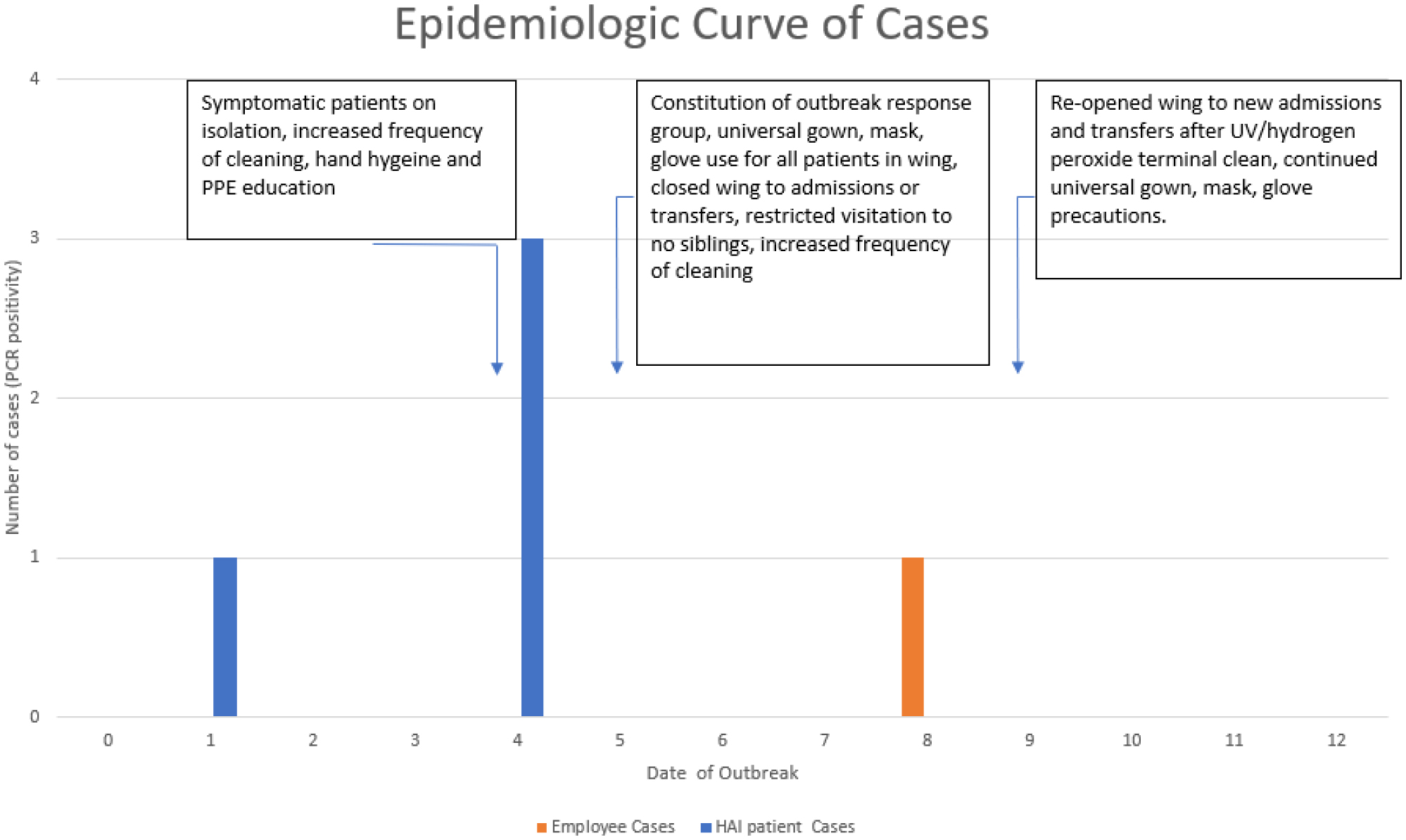
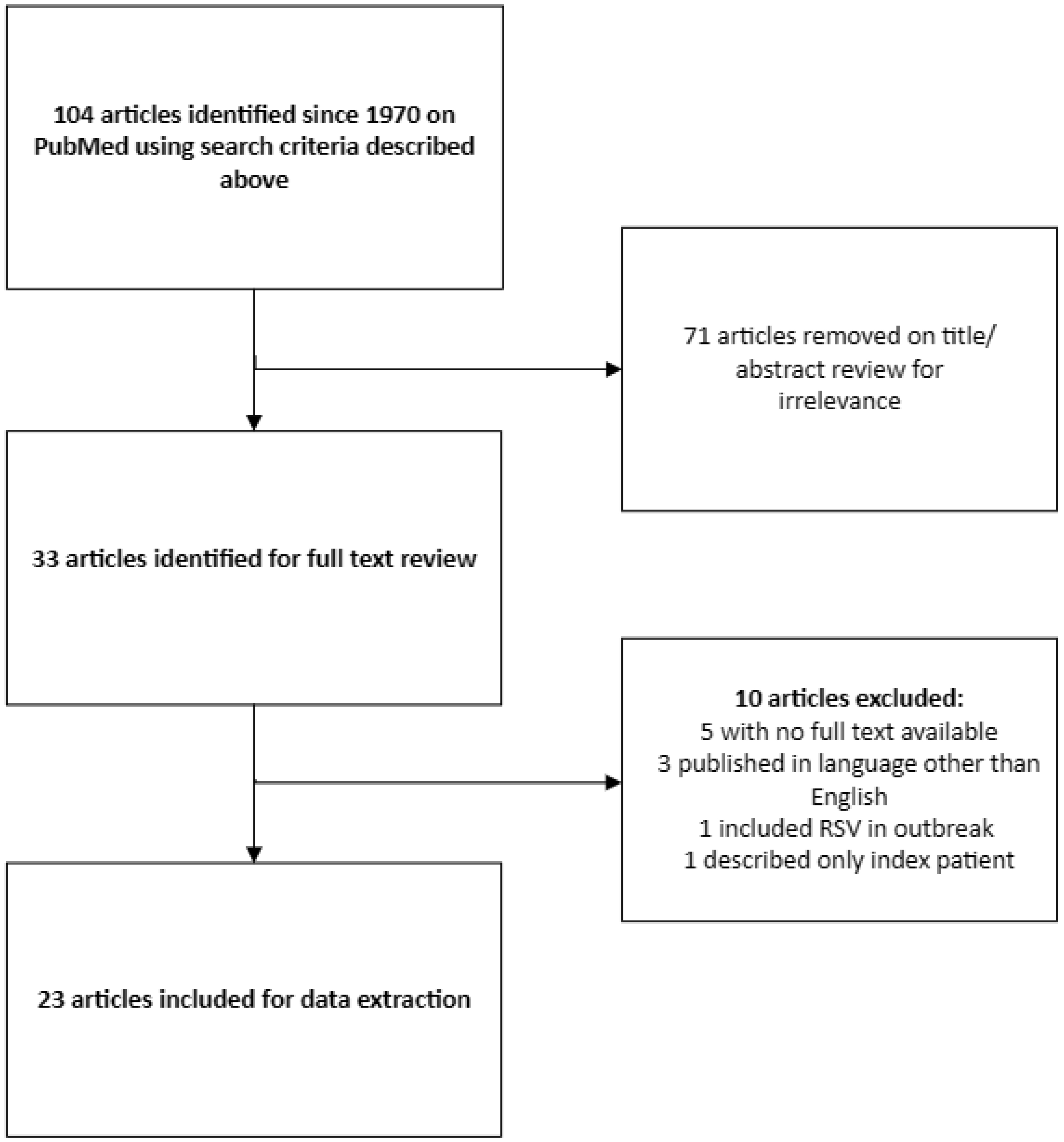
Neonatal enterovirus infections have the potential to cause devastating illness and death in this vulnerable age group. Existing evidence suggests that the incidence of enteroviral infections in the post-natal period may be higher than previously thought. Because neonates infected with enterovirus are at risk of severe sequelae, and healthcare-associated outbreaks in neonatal settings can occur, enteroviral infection in hospitalized neonates is a serious concern. Thus, it is essential to conduct surveillance for these infections and to deploy robust infection control measures once the virus has been detected in a neonatal care setting. Here, we report an outbreak of enterovirus in a neonatal intensive care unit (NICU) that was rapidly identified and contained, resulting in relatively few cases but requiring temporary closure of the unit. Additionally, we present our review of the literature describing the characteristics of enteroviral outbreaks in NICU and nursery settings to compare published outcomes of outbreaks to those of our outcome.
Citation: Nathan L'Etoile, Lindsay Brim, Susan Coffin, Ericka Hayes. Report of an outbreak of enterovirus disease in a neonatal intensive care unit and a systematic review of the literature[J]. AIMS Microbiology, 2025, 11(1): 167-181. doi: 10.3934/microbiol.2025009
Neonatal enterovirus infections have the potential to cause devastating illness and death in this vulnerable age group. Existing evidence suggests that the incidence of enteroviral infections in the post-natal period may be higher than previously thought. Because neonates infected with enterovirus are at risk of severe sequelae, and healthcare-associated outbreaks in neonatal settings can occur, enteroviral infection in hospitalized neonates is a serious concern. Thus, it is essential to conduct surveillance for these infections and to deploy robust infection control measures once the virus has been detected in a neonatal care setting. Here, we report an outbreak of enterovirus in a neonatal intensive care unit (NICU) that was rapidly identified and contained, resulting in relatively few cases but requiring temporary closure of the unit. Additionally, we present our review of the literature describing the characteristics of enteroviral outbreaks in NICU and nursery settings to compare published outcomes of outbreaks to those of our outcome.
Hand-foot-and-mouth disease
Infection prevention and control
Intravenous immune globulin
Neonatal intensive care unit
Outbreak Reports and Intervention Studies of Nosocomial Infection
Polymerase chain reaction
Personal protective equipment
Preferred Reporting Items for Systematic Reviews and Meta-Analyses

| [1] | Hawkes MT, Vaudry W (2005) Nonpolio enterovirus infection in the neonate and young infant. Paediatr Child Health 10: 383-388. |
| [2] |
Zhang M, Wang H, Tang J, et al. (2021) Clinical characteristics of severe neonatal enterovirus infection: a systematic review. BMC Pediatr 21: 127. https://doi.org/10.1186/s12887-021-02599-y 
|
| [3] |
Jenista JA, Powell KR, Menegus MA (1984) Epidemiology of neonatal enterovirus infection. J Pediatr 104: 685-690. https://doi.org/10.1016/S0022-3476(84)80944-0
|
| [4] |
Stone SP, Cooper BS, Kibbler CC, et al. (2007) The ORION statement: guidelines for transparent reporting of outbreak reports and intervention studies of nosocomial infection. Lancet Infect Dis 7: 282-288. https://doi.org/10.1016/S1473-3099(07)70082-8
|
| [5] |
Kares S, Lönnrot M, Vuorinen P, et al. (2004) Real-time PCR for rapid diagnosis of entero- and rhinovirus infections using LightCycler. J Clin Virol 29: 99-104. https://doi.org/10.1016/S1386-6532(03)00093-3
|
| [6] |
Page MJ, McKenzie JE, Bossuyt PM, et al. (2021) The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372: n71. https://doi.org/10.1136/bmj.n71
|
| [7] |
Bhambhani V, Abraham J, Sahni M, et al. (2007) Outbreak of Coxsackie B4 arthritis among newborns and staff of a neonatal unit. Trop Doct 37: 188-189. https://doi.org/10.1258/004947507781524728
|
| [8] | Chen JH, Chiu NC, Chang JH, et al. (2005) A neonatal echovirus 11 outbreak in an obstetric clinic. J Microbiol Immunol Infect 38: 332-337. |
| [9] | Rabkin CS, Telzak EE, Ho MS, et al. (1988) Outbreak of echovirus 11 infection in hospitalized neonates. Pediatr Infect Dis J 7: 186-190. |
| [10] |
Rantakallio P, Lapinleimu K, Mäntyjärvi R (1970) Coxsackie B 5 outbreak in a newborn nursery with 17 cases of serous meningitis. Scand J Infect Dis 2: 17-23. https://doi.org/10.3109/inf.1970.2.issue-1.03
|
| [11] | Lapinleimu K, Hakulinen A (1972) A hospital outbreak caused by ECHO virus type 11 among newborn infants. Ann Clin Res 4: 183-187. |
| [12] | Steinmann J, Albrecht K (1985) Echovirus 11-Epidemie bei Frühgeborenen auf einer Neonatal-Intensiv-Station [Echovirus 11 outbreak among premature newborn infants in a neonatal intensive care unit]. Zentralbl Bakteriol Mikrobiol Hyg A 259: 284-293. https://doi.org/10.1016/S0176-6724(85)80059-6 |
| [13] | Kusuhara K, Hikino S, Saito M, et al. (2007) Echovirus18 (Echo18) outbreak in an intensive care unit for newborn infants. Fukuoka Igaku Zasshi 98: 405. |
| [14] |
Haas R, Neumann D, Oeding U, et al. (1972) Ein Ausbruch von Coxsackie-B5-Meningitiden bei Neugeborenen einer Entbindungsabteilung [An epidemic of Coxsackie B5 meningitis in a newborn nursery]. Dtsch Med Wochenschr 97: 1203-1207. https://doi.org/10.1055/s-0028-1107529
|
| [15] |
Wilson CW, Stevenson DK, Arvin AM (1989) A concurrent epidemic of respiratory syncytial virus and echovirus 7 infections in an intensive care nursery. Pediatr Infect Dis J 8: 24-29. https://doi.org/10.1097/00006454-198901000-00008
|
| [16] |
Carolane DJ, Long AM, McKeever PA, et al. (1985) Prevention of spread of echovirus 6 in a special care baby unit. Arch Dis Child 60: 674-676. https://doi.org/10.1136/adc.60.7.674
|
| [17] | Drew JH (1973) Echo 11 virus outbreak in a nursery associated with myocarditis. Aust Paediatr J 9: 90-95. https://doi.org/10.1111/j.1440-1754.1973.tb01856.x |
| [18] | Faulkner RS, Van Rooyen CE (1973) Echovirus type 17 in the neonate. Can Med Assoc J 108: 878. https://doi.org/10.1097/00006254-197311000-00012 |
| [19] |
Eilard T, Kyllerman M, Wennerblom I, et al. (1974) An outbreak of Coxsackie virus type B2 among neonates in an obstetrical ward. Acta Paediatr Scand 63: 103-107. https://doi.org/10.1111/j.1651-2227.1974.tb04356.x
|
| [20] |
Mertens T, Hager H, Eggers HJ (1982) Epidemiology of an outbreak in a maternity unit of infections with an antigenic variant of Echovirus 11. J Med Virol 9: 81-91. https://doi.org/10.1002/jmv.1890090202
|
| [21] |
Nagington J, Gandy G, Walker J, et al. (1983) Use of normal immunoglobulin in an echovirus 11 outbreak in a special-care baby unit. Lancet 2: 443-446. https://doi.org/10.1016/S0140-6736(83)90402-6
|
| [22] |
Reiss-Levy E, Baker A, Don N, et al. (1986) Two concurrent epidemics of enteroviral meningitis in an obstetric neonatal unit. Aust N Z J Med 16: 365-372. https://doi.org/10.1111/j.1445-5994.1986.tb01188.x
|
| [23] |
Isaacs D, Dobson SR, Wilkinson AR, et al. (1989) Conservative management of an echovirus 11 outbreak in a neonatal unit. Lancet 1: 543-545. https://doi.org/10.1016/S0140-6736(89)90078-0
|
| [24] |
Wreghitt TG, Sutehall GM, King A, et al. (1989) Fatal echovirus 7 infection during an outbreak in a special care baby unit. J Infect 19: 229-236. https://doi.org/10.1016/S0163-4453(89)90709-3
|
| [25] |
Birenbaum E, Handsher R, Kuint J, et al. (1997) Echovirus type 22 outbreak associated with gastro-intestinal disease in a neonatal intensive care unit. Am J Perinatol 14: 469-473. https://doi.org/10.1055/s-2007-994182
|
| [26] |
Pasic S, Jankovic B, Abinun M, et al. (1997) Intravenous immunoglobulin prophylaxis in an echovirus 6 and echovirus 4 nursery outbreak. Pediatr Infect Dis J 16: 718-720. https://doi.org/10.1097/00006454-199707000-00019
|
| [27] |
Takami T, Kawashima H, Takei Y, et al. (1998) Usefulness of nested PCR and sequence analysis in a nosocomial outbreak of neonatal enterovirus infection. J Clin Virol 11: 67-75. https://doi.org/10.1016/S0928-0197(98)00022-1
|
| [28] |
Austin BJ, Croxson MC, Powell KF, et al. (1999) The successful containment of coxsackie B4 infection in a neonatal unit. J Paediatr Child Health 35: 102-104. https://doi.org/10.1046/j.1440-1754.1999.00346.x
|
| [29] |
Jankovic B, Pasic S, Kanjuh B, et al. (1999) Severe neonatal echovirus 17 infection during a nursery outbreak. Pediatr Infect Dis J 18: 393-394. https://doi.org/10.1097/00006454-199904000-00023
|
| [30] |
Eisenhut M, Algawi B, Wreghitt T, et al. (2000) Fatal Coxsackie A9 virus infection during an outbreak in a neonatal unit. J Infect 40: 297-298. https://doi.org/10.1053/jinf.2000.0650
|
| [31] |
Takami T, Sonodat S, Houjyo H, et al. (2000) Diagnosis of horizontal enterovirus infections in neonates by nested PCR and direct sequence analysis. J Hosp Infect 45: 283-287. https://doi.org/10.1053/jhin.2000.0788
|
| [32] |
Syriopoulou VP, Hadjichristodoulou CH, Daikos GL, et al. (2002) Clinical and epidemiological aspects of an enterovirus outbreak in a neonatal unit. J Hosp Infect 51: 275-280. https://doi.org/10.1053/jhin.2002.1253
|
| [33] |
Apisarnthanarak A, Kitphati R, Pongsuwann Y, et al. (2005) Echovirus type 11: outbreak of hand-foot-and-mouth disease in a Thai hospital nursery. Clin Infect Dis 41: 1361-1362. https://doi.org/10.1086/497076
|
| [34] |
Kusuhara K, Saito M, Sasaki Y, et al. (2008) An echovirus type 18 outbreak in a neonatal intensive care unit. Eur J Pediatr 167: 587-589. https://doi.org/10.1007/s00431-007-0516-x
|
| [35] |
Huang FL, Chen CH, Huang SK, et al. (2010) An outbreak of enterovirus 71 in a nursery. Scand J Infect Dis 42: 609-612. https://doi.org/10.3109/00365541003754444
|
| [36] |
Siafakas N, Goudesidou M, Gaitana K, et al. (2013) Successful control of an echovirus 6 meningitis outbreak in a neonatal intensive care unit in central Greece. Am J Infect Control 41: 1125-1128. https://doi.org/10.1016/j.ajic.2013.02.014
|
| [37] |
Alidjinou EK, Lazrek M, Schuffenecker I, et al. (2018) Necrotizing Enterocolitis Cases Associated with Nosocomial Enterovirus Transmission in a Neonatal Unit. Pediatr Infect Dis J 37: 954-957. https://doi.org/10.1097/INF.0000000000001928
|
| [38] |
Ho SY, Chiu CH, Huang YC, et al. (2020) Investigation and successful control of an echovirus 11 outbreak in neonatal intensive care units. Pediatr Neonatol 61: 180-187. https://doi.org/10.1016/j.pedneo.2019.09.012
|
| [39] |
Xi H, Tian Y, Shao H, et al. (2023) An outbreak of nosocomial infection of neonatal aseptic meningitis caused by echovirus 18. Epidemiol Infect 151: e107. https://doi.org/10.1017/S0950268823000973
|
Figures(2) / Tables(2)

Nathan L'Etoile, Lindsay Brim, Susan Coffin, Ericka Hayes. Report of an outbreak of enterovirus disease in a neonatal intensive care unit and a systematic review of the literature[J]. AIMS Microbiology, 2025, 11(1): 167-181. doi: 10.3934/microbiol.2025009







 DownLoad:
DownLoad: