Citation: Vinh Huy Chau. Powerlifting score prediction using a machine learning method[J]. Mathematical Biosciences and Engineering, 2021, 18(2): 1040-1050. doi: 10.3934/mbe.2021056

| [1] | D. J. V. D. Windt, V. Sud, H. Zhang, A. Tsung, H. Huang, The effects of physical exercise on fatty liver disease, J. Liver Res., 18 (2018), 89–101. |
| [2] |
D. Song, D. S. F. Yu, P. W. C. Li, Y. Lei, The effectiveness of physical exercise on cognitive and psychological outcomes in individuals with mild cognitive impairment: A systematic review and meta-analysis, Int. J. Nurs. Stud., 79 (2018), 155–164. doi: 10.1016/j.ijnurstu.2018.01.002

|
| [3] | M. G. Benedetti, G. Furlini, A. Zati, G. L. Mauro, The effectiveness of physical exercise on bone density in osteoporotic patients, Bio. Med. Res. Int., (2018), 4840531. |
| [4] |
M. M. Ziaaldini, E. Marzetti, A. Picca, Z. Murlasits, Biochemical pathways of sarcopenia and their modulation by physical exercise: A narrative review, Front. Med., 4 (2017), 167. doi: 10.3389/fmed.2017.00167
|
| [5] |
C. M. Hearing, W. C. Chang, K. L. Szuhany, T. Deckersbach, A. A. Nierenberg, L. G. Sylvia, Physical exercise for treatment of mood disorders: A critical review, Curr. Behav. Neurosci. Rep., 3 (2016), 350–359. doi: 10.1007/s40473-016-0089-y
|
| [6] | L. W. Judge, L. J. Urbina, D. L. Hoover, B. W. Craig, L. M. Judge, B. M. Leitzelar, et al., The impact of competitive trait anxiety on collegiate powerlifting performance, J. Strength Cond. Res., 30 (2016), 2399–2405. |
| [7] | M. Mottaghi, A. Atarodi, Z. Rohani, The relationship between coaches' and athletes' competitive anxiety and their performance, Iran. J. Psychiatry Behav. Sci., 7 (2013), 68–76. |
| [8] |
H. J. Pritchard, D. A. Tod, M. J. Barnes, J. W. Keogh, M. R. McGuigan, Tapering practices of New Zealand's elite raw powerlifters, J. Strength Cond. Res., 30 (2016), 1796–1804. doi: 10.1519/JSC.0000000000001292
|
| [9] |
M. Zawadka, M. S. Paszkowska, P. Gawda, E. Lukasik, J. Smolka, M. Jablonski, What factors can affect lumbopelvic flexion-extension motion in the sagittal plane?: A literature review, Hum. Mov. Sci., 58 (2018), 205–218. doi: 10.1016/j.humov.2018.02.008
|
| [10] | A. C. Fry, W. J. Kraemer, M. H. Stone, L. P. Koziris, J. T. Thrush, S. J. Fleck, Relationships between serum testosterone, cortisol and weightlifting performance, J. Strength Cond. Res., 14 (2000), 338–343. |
| [11] | I. Sandau, M. Witt, The influence of stress factors on joint loading of lower extremities in weightlifting, Ger. J. Sports Med./Deutsch. Z. Sportmed., 69 (2018), 1–10. |
| [12] | P. A. Solberg, W. G. Hopkins, G. Paulsen, T. A. Haugen, Peak age and performance progression in world-class weightlifting and powerlifting athletes, Int. J. Sports Physiol. Perform., (2019), 1–24. |
| [13] |
C. Latella, W. P. Teo, J. Spathis, D. V. D. Hoek, Long-term strength adaptation: A 15-year analysis of powerlifting athletes, J. Strength Cond. Res., 34 (2020), 2412. doi: 10.1519/JSC.0000000000003657
|
| [14] |
C. Latella, D. V. D. Hoek, W. P. Teo, Factors affecting powerlifting performance: an analysis of age-and weight-based determinants of relative strength, Int. J. Perform. Anal. Sport, 18 (2018), 532–544. doi: 10.1080/24748668.2018.1496393
|
| [15] | M. M. Anton, W. W. Spirduso, H. Tanaka, Age-related declines in anaerobic muscular performance: Weightlifting and powerlifting, Med. Sci. Sports Exercise, 36 (2014), 143–147. |
| [16] |
L. P. James, P. Comfort, T. J. Suchomel, V. G. Kelly, E. M. Beckman, G. G. Haff, The impact of power clean ability and training age on adaptations to weightlifting-style training, J. Strength Cond. Res., 33 (2019), 2936–2944. doi: 10.1519/JSC.0000000000002534
|
| [17] |
J. Pearson, J. G. Spathis, D. J. V. D. Hoek, P. J. Owen, J. Weakley, C. Latella, Effect of competition frequency on strength performance of powerlifting athletes, J. Strength Cond. Res., 34 (2020), 1213–1219. doi: 10.1519/JSC.0000000000003563
|
| [18] |
N. A. Coker, A. N. Varanoske, K. M. Baker, D. L. H. Vaughn, A. J. Wells, Predictors of competitive success of national-level powerlifters: A multilevel analysis, Int. J. Perform. Anal. Sport, 18 (2018), 796–805. doi: 10.1080/24748668.2018.1519751
|
| [19] | S. K. Travis, M. C. Zourdos, C. D. Bazyler, Weight selection attempts of elite classic powerlifters, Percept. Mot. Skills, 2020. |
| [20] | M. Z. Naser, A. Alavi, Insights into performance fitness and error metrics for machine learning, preprint, arXiv: 2006.00887. |
| [21] | A. Botchkarev, Performance metrics (error measures) in machine learning regression, forecasting and prognostics: Properties and typology, preprint, arXiv: 1809.03006. |
| [22] |
G. B. Huang, Q. Y. Zhu, C. K. Siew, Extreme learning machine: Theory and applications, Neurocomputing, 70 (2006), 489–501. doi: 10.1016/j.neucom.2005.12.126
|
| [23] | M. Rocca, C. Perna, Nonlinear autoregressive sieve bootstrap based on extreme learning machines, Math. Biosci. Eng., 17 (2019), 636–653. |
| [24] | G. B. Huang, H. Zhou, X. Ding, R. Zhang, Extreme learning machine for regression and multiclass classification, IEEE Trans. Syst., Man, Cybern., Part B (Cybern.), 42 (2011), 513–529. |
| [25] | J. Tang, C. Deng, G. B. Huang, Extreme learning machine for multilayer perceptron, IEEE Trans. Neural Networks Learn. Syst., 27 (2015), 809–821. |
| [26] | W. Deng, Q. Zheng, L. Chen, Regularized extreme learning machine, 2009 IEEE Symp. Comput. Intel. Data Min., (2009), 389–395. |
| [27] | Y. Zheng, B. Chen, S. Wang, W. Wang, W. Qin, Mixture correntropy-based kernel extreme learning machines, IEEE Trans. Neural Networks Learn. Syst., 2020. |
| [28] | J. Cao, H. Dai, B. Lei, C. Yin, H. Zeng, A. Kummert, Maximum correntropy criterion-based hierarchical one-class classification, IEEE Trans. Neural Networks Learn. Syst., 2020. |
| [29] |
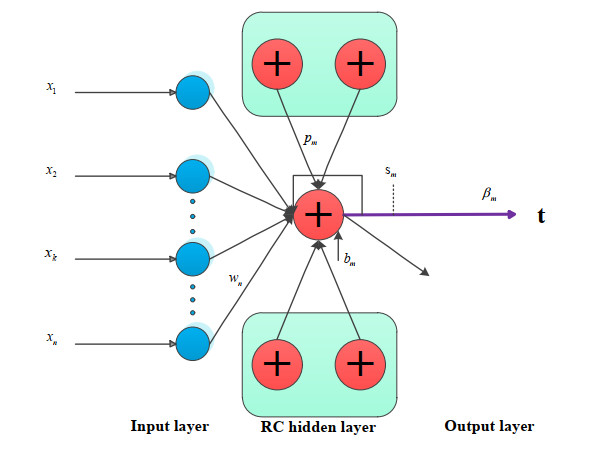
O. F. Ertugrul, A novel randomized machine learning approach: Reservoir computing extreme learning machine. Appl. Soft Comput., 94 (2020), 106433. doi: 10.1016/j.asoc.2020.106433
|
| [30] |
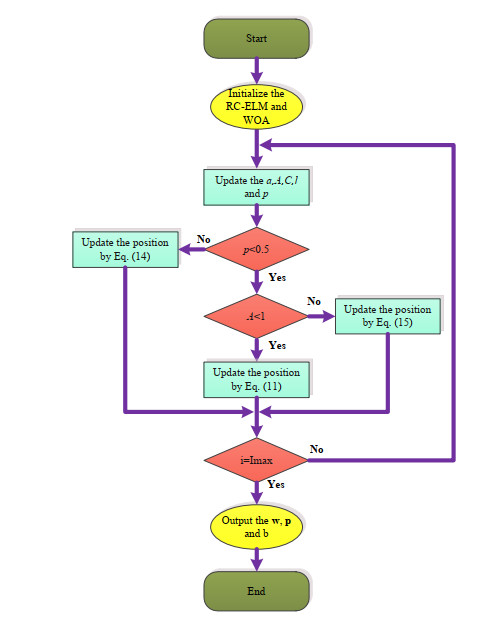
S. Mirjalili, A. Lewis, The whale optimization algorithm. Adv. Eng. Software, 95 (2016), 51–67. doi: 10.1016/j.advengsoft.2016.01.008
|
| [31] |
L. L. Li, J. Sun, M. L. Tseng, Z. G. Li, Extreme learning machine optimized by whale optimization algorithm using insulated gate bipolar transistor module aging degree evaluation, Expert Syst. Appl., 127 (2019), 58–67. doi: 10.1016/j.eswa.2019.03.002
|
| [32] | https://www.powerlifting.sport/championships/results.html |
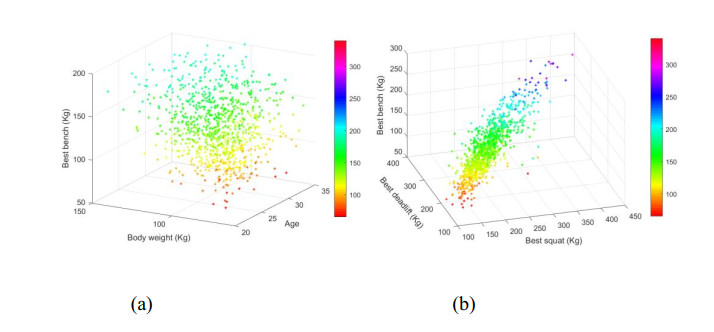
| [33] | https://www.kaggle.com/open-powerlifting/powerlifting-database |
| [34] | T. Yang, Study on the growth rule of the olympic men's weightlifting champion and winning factors. Sichuan Sports Sci., 38 (2019), 54–58. |
| [35] |
B. T. Le, D. Xiao, Y. Mao, D. He, Coal analysis based on visible-infrared spectroscopy and a deep neural network, Infrared Phys. Technol., 93 (2018), 34–40. doi: 10.1016/j.infrared.2018.07.013
|
| [36] | D. Xiao, B. T. Le, Rapid analysis of coal characteristics based on deep learning and visible-infrared spectroscopy, Microchem. J., (2020), 104880. |
Figures(5)

Vinh Huy Chau. Powerlifting score prediction using a machine learning method[J]. Mathematical Biosciences and Engineering, 2021, 18(2): 1040-1050. doi: 10.3934/mbe.2021056







 DownLoad:
DownLoad: