The purpose of the present study was to investigate the effects of neuromodulation techniques, including transcranial direct current stimulation, transcranial magnetic stimulation, and deep brain stimulation, on the treatments of nicotine dependence. Specifically, our objective was to assess the existing evidence by conducting an umbrella review of systematic reviews. The quality of the included studies was evaluated using the standardized tools designed to evaluate systematic reviews. The PubMed/MEDLINE database was queried for systematic reviews, and yielded 7 systematic reviews with a substantial sample size (N = 4,252), some of which included meta-analyses. A significant finding across these studies was the effectiveness of neuromodulation techniques to reduce nicotine cravings and consumption, through the evidence remains not yet conclusive. A significant efficacy of transcranial direct current stimulation and repetitive transcranial magnetic stimulation that targeted the dorsolateral prefrontal cortex was found, as well as the lateral prefrontal cortex and insula bilaterally, on smoking frequency and craving. Moreover, smoking behaviors may also be positively affected by the use of deep brain stimulation (DBS) targeting the nucleus accumbens. In conclusion, neuromodulation approaches hold promise as effective treatments for tobacco use disorder. Nonetheless, further research is required to comprehensively understand their effectiveness and to determine if combining them with other treatments can aid individuals to successfully quit smoking.
Citation: Graziella Orrù, Marina Baroni, Ciro Conversano, Angelo Gemignani. Exploring the therapeutic potential of tDCS, TMS and DBS in overcoming tobacco use disorder: an umbrella review[J]. AIMS Neuroscience, 2024, 11(4): 449-467. doi: 10.3934/Neuroscience.2024027
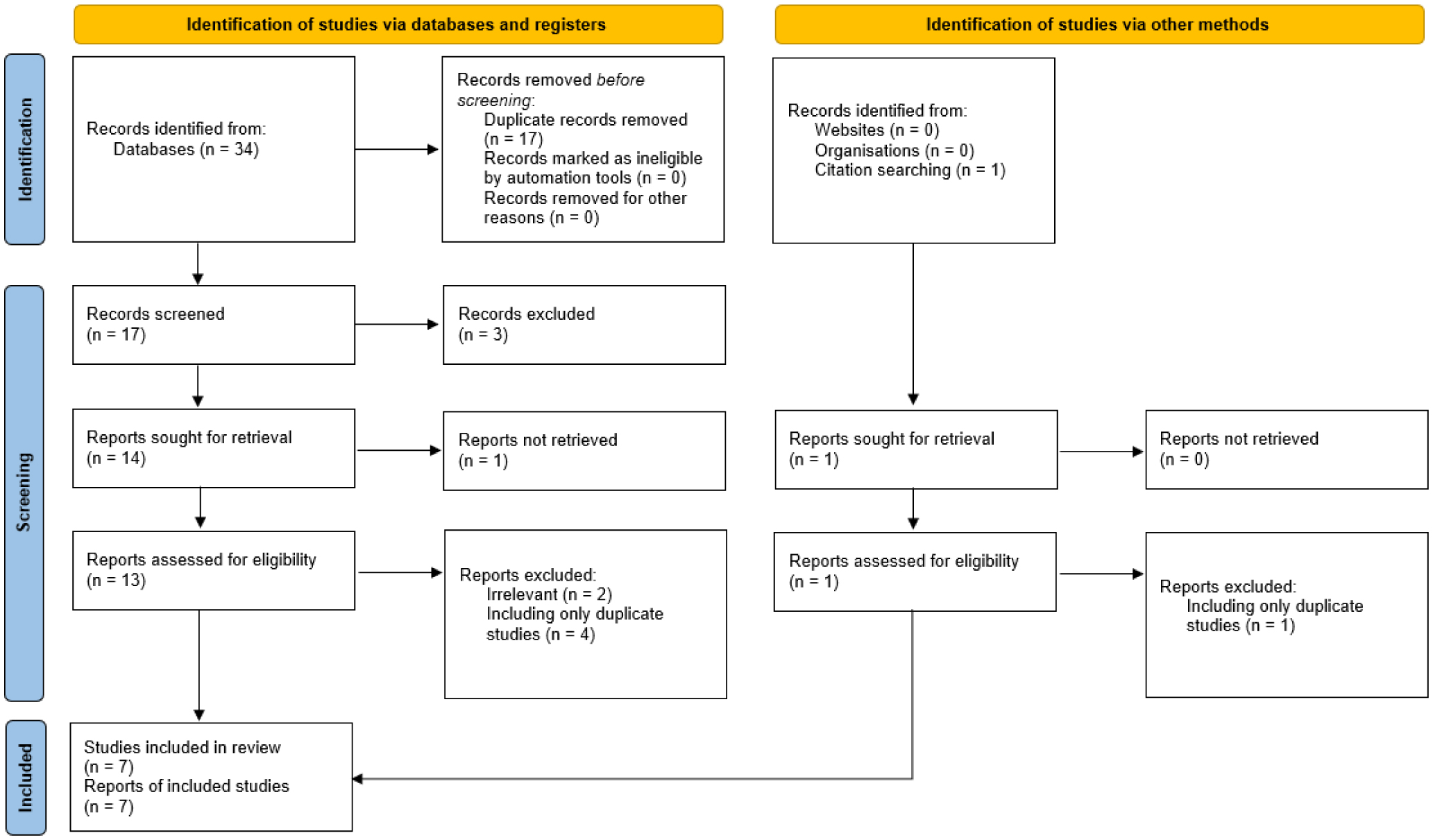
The purpose of the present study was to investigate the effects of neuromodulation techniques, including transcranial direct current stimulation, transcranial magnetic stimulation, and deep brain stimulation, on the treatments of nicotine dependence. Specifically, our objective was to assess the existing evidence by conducting an umbrella review of systematic reviews. The quality of the included studies was evaluated using the standardized tools designed to evaluate systematic reviews. The PubMed/MEDLINE database was queried for systematic reviews, and yielded 7 systematic reviews with a substantial sample size (N = 4,252), some of which included meta-analyses. A significant finding across these studies was the effectiveness of neuromodulation techniques to reduce nicotine cravings and consumption, through the evidence remains not yet conclusive. A significant efficacy of transcranial direct current stimulation and repetitive transcranial magnetic stimulation that targeted the dorsolateral prefrontal cortex was found, as well as the lateral prefrontal cortex and insula bilaterally, on smoking frequency and craving. Moreover, smoking behaviors may also be positively affected by the use of deep brain stimulation (DBS) targeting the nucleus accumbens. In conclusion, neuromodulation approaches hold promise as effective treatments for tobacco use disorder. Nonetheless, further research is required to comprehensively understand their effectiveness and to determine if combining them with other treatments can aid individuals to successfully quit smoking.

| [1] | Cornelius ME (2022) Tobacco product use among adults—United States, 2020. MMWR-Morbid Mortal W 71. http://dx.doi.org/10.15585/mmwr.mm6946a4 |
| [2] |
Hatsukami DK, Stead LF, Gupta PC (2008) Tobacco addiction. Lancet 371: 2027-2038. https://doi.org/10.1016/S0140-6736(08)60871-5 
|
| [3] |
West R (2017) Tobacco smoking: Health impact, prevalence, correlates and interventions. Psychol Health 32: 1018-1036. https://doi.org/10.1080/08870446.2017.1325890
|
| [4] |
Hughes JR, Keely J, Naud S (2004) Shape of the relapse curve and long-term abstinence among untreated smokers. Addiction 99: 29-38. https://doi.org/10.1111/j.1360-0443.2004.00540.x
|
| [5] |
Stapleton JA, West R (2012) A direct method and ICER tables for the estimation of the cost-effectiveness of smoking cessation interventions in general populations: application to a new cytisine trial and other examples. Nicotine Tob Res 14: 463-471. https://doi.org/10.1093/ntr/ntr236
|
| [6] |
Van Schayck OCP, Williams S, Barchilon V, et al. (2017) Treating tobacco dependence: guidance for primary care on life-saving interventions. Position statement of the IPCRG. NPJ Prim Care Resp M 27: 38. https://doi.org/10.1038/s41533-017-0039-5
|
| [7] |
Piasecki TM (2006) Relapse to smoking. Clin Psychol Rev 26: 196-215. https://doi.org/10.1016/j.cpr.2005.11.007
|
| [8] |
Horvath JC, Carter O, Forte JD (2014) Transcranial direct current stimulation: five important issues we aren't discussing (but probably should be). Front Syst Neurosci 8: 2. https://doi.org/10.3389/fnsys.2014.00002
|
| [9] |
Rabipour S, Wu AD, Davidson PS, et al. (2018) Expectations may influence the effects of transcranial direct current stimulation. Neuropsychologia 119: 524-534. https://doi.org/10.1016/j.neuropsychologia.2018.09.005
|
| [10] |
Vitor de Souza Brangioni MC, Pereira DA, Thibaut A, et al. (2018) Effects of prefrontal transcranial direct current stimulation and motivation to quit in tobacco smokers: a randomized, sham controlled, double-blind trial. Front Pharmacol 9: 14. https://doi.org/10.3389/fphar.2018.00014
|
| [11] |
Guerra A, López-Alonso V, Cheeran B, et al. (2020) Solutions for managing variability in non-invasive brain stimulation studies. Neurosci Lett 719: 133332. https://doi.org/10.1016/j.neulet.2017.12.060
|
| [12] |
Stein ER, Gibson BC, Votaw VR, et al. (2019) Non-invasive brain stimulation in substance use disorders: implications for dissemination to clinical settings. Curr Opin Psychol 30: 6-10. https://doi.org/10.1016/j.copsyc.2018.12.009
|
| [13] |
Young JR, Smani SA, Mischel NA, et al. (2020) Non-invasive brain stimulation modalities for the treatment and prevention of opioid use disorder: a systematic review of the literature. J Addict Dis 38: 186-199. https://doi.org/10.1080/10550887.2020.1736756
|
| [14] |
Zhang X, Huang M, Yu Y, et al. (2024) Is Transcranial Direct Current Stimulation Effective for Cognitive Dysfunction in Substance Use Disorders? A Systematic Review. Brain Sci 14: 754. https://doi.org/10.3390/brainsci14080754
|
| [15] |
Brunoni AR, Moffa AH, Fregni F, et al. (2016) Transcranial direct current stimulation for acute major depressive episodes: meta-analysis of individual patient data. Brit J Psychiat 208: 522-531. https://doi.org/10.1192/bjp.bp.115.164715
|
| [16] |
Fitzgerald PB, Hoy KE, Anderson RJ, et al. (2016) A study of the pattern of response to rTMS treatment in depression. Depress Anxiety 33: 746-753. https://doi.org/10.1002/da.22503
|
| [17] |
Mayberg HS, Lozano AM, Voon V, et al. (2005) Deep brain stimulation for treatment-resistant depression. Neuron 45: 651-660. https://doi.org/10.1016/j.neuron.2005.02.014
|
| [18] |
Orrù G, Conversano C, Hitchcott PK, et al. (2020a) Motor stroke recovery after tDCS: a systematic review. Rev Neuroscience 31: 201-218. https://doi.org/10.1515/revneuro-2019-0047
|
| [19] |
Dionisio A, Duarte IC, Patricio M, et al. (2018) The use of repetitive transcranial magnetic stimulation for stroke rehabilitation: a systematic review. J Stroke Cerebrovasc 27: 1-31. https://doi.org/10.1016/j.jstrokecerebrovasdis.2017.09.008
|
| [20] |
Fisicaro F, Lanza G, Grasso AA, et al. (2019) Repetitive transcranial magnetic stimulation in stroke rehabilitation: review of the current evidence and pitfalls. Ther Adv Neurol Diso 12: 1756286419878317. https://doi.org/10.1177/1756286419878317
|
| [21] | Paro MR, Dyrda M, Ramanan S, et al. (2022) Deep brain stimulation for movement disorders after stroke: a systematic review of the literature. J Neurosurg 138: 1688-1701. https://doi.org/10.3171/2022.8.JNS221334 |
| [22] |
Baker KB, Plow EB, Nagel S, et al. (2023) Cerebellar deep brain stimulation for chronic post-stroke motor rehabilitation: a phase I trial. Nat Med 29: 2366-2374. https://doi.org/10.1038/s41591-023-02507-0
|
| [23] | Orru G, Baroni M, Cesari V, et al. (2019) The effect of single and repeated tDCS sessions on motor symptoms in Parkinson's disease: a systematic review. Arch Ital Biol 157. https://doi.org/10.12871/aib.v157i2-3.4707 |
| [24] |
Pateraki G, Anargyros K, Aloizou AM, et al. (2022) Therapeutic application of rTMS in neurodegenerative and movement disorders: A review. J Electromyogr Kines 62: 102622. https://doi.org/10.1016/j.jelekin.2021.102622
|
| [25] |
Baumgartner AJ, Thompson JA, Kern DS, et al. (2022) Novel targets in deep brain stimulation for movement disorders. Neurosurg Rev 45: 2593-2613. https://doi.org/10.1007/s10143-022-01770-y
|
| [26] |
Tai CH, Tseng SH (2022) Cerebellar deep brain stimulation for movement disorders. Neurobiol Dis 175: 105899. https://doi.org/10.1016/j.nbd.2022.105899
|
| [27] |
Orru G, Cesari V, Conversano C, et al. (2021a) The clinical application of transcranial direct current stimulation in patients with cerebellar ataxia: a systematic review. Int J Neurosci 131: 681-688. https://doi.org/10.1080/00207454.2020.1750399
|
| [28] |
Qiu YT, Chen Y, Tan HX, et al. (2024) Efficacy and safety of repetitive transcranial magnetic stimulation in cerebellar ataxia: a systematic review and meta-analysis. Cerebellum 23: 243-254. https://doi.org/10.1007/s12311-022-01508-y
|
| [29] | Cury RG, França C, Duarte KP, et al. (2021) Safety and outcomes of dentate nucleus deep brain stimulation for cerebellar ataxia. Cerebellum : 1-5. https://doi.org/10.1007/s12311-021-01326-8 |
| [30] | Orrù G, Cesari V, Baroni M, et al. (2020) Letter to the Editor: the application of transcranial direct current stimulation on phantom phenomena. Mediterr J Clin Psyc 8. https://doi.org/10.6092/2282-1619/mjcp-2382 |
| [31] | Knorst GRS, Souza PRD, Araújo AGPD, et al. (2024) Transcranial magnetic stimulation in the treatment of phantom limb pain: a systematic review. Arq Neuro-psiquiat 82: s00441779051. https://doi.org/10.1055/s-0044-1779051 |
| [32] |
Pang D, Ashkan K (2022) Deep brain stimulation for phantom limb pain. Eur J Paediatr Neuro 39: 96-102. https://doi.org/10.1016/j.ejpn.2022.05.009
|
| [33] |
Orrù G, Cesari V, Malloggi E, et al. (2022) The effects of Transcranial Direct Current Stimulation on food craving and food intake in individuals affected by obesity and overweight: a mini review of the magnitude of the effects. AIMS Neurosci 9: 358. https://doi.org/10.3934/Neuroscience.2022020
|
| [34] |
Gay A, Cabe J, De Chazeron I, et al. (2022) Repetitive transcranial magnetic stimulation (rTMS) as a promising treatment for craving in stimulant drugs and behavioral addiction: a meta-analysis. J Clin Med 11: 624. https://doi.org/10.3390/jcm11030624
|
| [35] |
Shivacharan RS, Rolle CE, Barbosa DA, et al. (2022) Pilot study of responsive nucleus accumbens deep brain stimulation for loss-of-control eating. Nat Med 28: 1791-1796. https://doi.org/10.1038/s41591-022-01941-w
|
| [36] |
Salling MC, Martinez D (2016) Brain stimulation in addiction. Neuropsychopharmacology 41: 2798-2809. https://doi.org/10.1038/npp.2016.80
|
| [37] |
Roth Y, Zangen A, Hallett M (2002) A coil design for transcranial magnetic stimulation of deep brain regions. J Clin Neurophysiol 19: 361-370.
|
| [38] |
Biernacki K, Lin MH, Baker TE (2020) Recovery of reward function in problematic substance users using a combination of robotics, electrophysiology, and TMS. Int J Psychophysiol 158: 288-298. https://doi.org/10.1016/j.ijpsycho.2020.08.008
|
| [39] |
Mikkonen M, Laakso I, Tanaka S, et al. (2020) Cost of focality in TDCS: Interindividual variability in electric fields. Brain Stimul 13: 117-124. https://doi.org/10.1016/j.brs.2019.09.017
|
| [40] |
Sandrini M, Xu B, Volochayev R, et al. (2020) Transcranial direct current stimulation facilitates response inhibition through dynamic modulation of the fronto-basal ganglia network. Brain Stimul 13: 96-104. https://doi.org/10.1016/j.brs.2019.08.004
|
| [41] |
Dani JA, Bertrand D (2007) Nicotinic acetylcholine receptors and nicotinic cholinergic mechanisms of the central nervous system. Annu Rev Pharmacol Toxicol 47: 699-729. https://doi.org/10.1146/annurev.pharmtox.47.120505.105214
|
| [42] |
Tsukada H, Miyasato K, Harada N, et al. (2005) Nicotine modulates dopamine synthesis rate as determined by L-(b-11C) DOPA: PET studies compared with (11C) raclopride binding in the conscious monkey brain. Synapse-New York 57: 120. https://doi.org/10.1002/syn.20157
|
| [43] |
Benowitz NL (2009) Pharmacology of nicotine: addiction, smoking-induced disease, and therapeutics. Annu Rev Pharmacol Toxicol 49: 57-71. https://doi.org/10.1146/annurev.pharmtox.48.113006.094742
|
| [44] |
Gallezot JD, Kloczynski T, Weinzimmer D, et al. (2014) Imaging nicotine-and amphetamine-induced dopamine release in rhesus monkeys with [11C] PHNO vs [11C] raclopride PET. Neuropsychopharmacology 39: 866-874. https://doi.org/10.1038/npp.2013.286
|
| [45] |
Herman AI, DeVito EE, Jensen KP, et al. (2014) Pharmacogenetics of nicotine addiction: role of dopamine. Pharmacogenomics 15: 221-234. https://doi.org/10.2217/pgs.13.246
|
| [46] |
Wright KN, Wesson DW (2021) The tubular striatum and nucleus accumbens distinctly represent reward-taking and reward-seeking. J Neurophysiol 125: 166-183. https://doi.org/10.1152/jn.00495.2020
|
| [47] |
Stein EA, Pankiewicz J, Harsch HH, et al. (1998) Nicotine-induced limbic cortical activation in the human brain: a functional MRI study. Am J Psychiat 155: 1009-1015. https://doi.org/10.1176/ajp.155.8.1009
|
| [48] |
Brody AL (2006) Functional brain imaging of tobacco use and dependence. J Psychiatr Res 40: 404-418. https://doi.org/10.1016/j.jpsychires.2005.04.012
|
| [49] |
Brody AL, Mandelkern MA, Jarvik ME, et al. (2004) Differences between smokers and nonsmokers in regional gray matter volumes and densities. Biol Psychiat 55: 77-84. https://doi.org/10.1016/S0006-3223(03)00610-3
|
| [50] |
Gallinat J, Meisenzahl E, Jacobsen LK, et al. (2006) Smoking and structural brain deficits: a volumetric MR investigation. Eur J Neurosci 24: 1744-1750. https://doi.org/10.1111/j.1460-9568.2006.05050.x
|
| [51] |
Yang Z, Zhang Y, Cheng J, et al. (2020) Meta-analysis of brain gray matter changes in chronic smokers. Eur J Radiol 132: 109300. https://doi.org/10.1016/j.ejrad.2020.109300
|
| [52] |
Zhang X, Salmeron BJ, Ross TJ, et al. (2011) Factors underlying prefrontal and insula structural alterations in smokers. Neuroimage 54: 42-48. https://doi.org/10.1016/j.neuroimage.2010.08.008
|
| [53] |
Naqvi NH, Bechara A (2009) The hidden island of addiction: the insula. Trends Neurosci 32: 56-67. https://doi.org/10.1016/j.tins.2008.09.009
|
| [54] |
Zhong J, Shi H, Shen Y, et al. (2016) Voxelwise meta-analysis of gray matter anomalies in chronic cigarette smokers. Behav Brain Res 311: 39-45. https://doi.org/10.1016/j.bbr.2016.05.016
|
| [55] | Kung J, Chiappelli F, Cajulis OO, et al. (2010) From systematic reviews to clinical recommendations for evidence-based health care: validation of revised assessment of multiple systematic reviews (R-AMSTAR) for grading of clinical relevance. Open Dent J 4: 84. https://doi.org/10.2174/1874210601004020084 |
| [56] | Shea BJ, Reeves BC, Wells G, et al. (2017) AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. Bmj : 358. https://doi.org/10.1136/bmj.j4008 |
| [57] |
De Santis KK, Lorenz RC, Lakeberg M, et al. (2022) The application of AMSTAR2 in 32 overviews of systematic reviews of interventions for mental and behavioural disorders: A cross-sectional study. Res Synth Methods 13: 424-433. https://doi.org/10.1002/jrsm.1532
|
| [58] |
Shea BJ, Hamel C, Wells GA, et al. (2009) AMSTAR is a reliable and valid measurement tool to assess the methodological quality of systematic reviews. J Clin Epidemiol 62: 1013-1020. https://doi.org/10.1016/j.jclinepi.2008.10.009
|
| [59] |
Bojcic R, Todoric M, Puljak L (2022) Adopting AMSTAR 2 critical appraisal tool for systematic reviews: speed of the tool uptake and barriers for its adoption. Bmc Med Res Methodol 22: 104. https://doi.org/10.1186/s12874-022-01592-y
|
| [60] | Page MJ, McKenzie JE, Bossuyt PM, et al. (2021) The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Bmj : 372. https://doi.org/10.1136/bmj.n71 |
| [61] |
Kang N, Kim RK, Kim HJ (2019) Effects of transcranial direct current stimulation on symptoms of nicotine dependence: a systematic review and meta-analysis. Addict Behav 96: 133-139. https://doi.org/10.1016/j.addbeh.2019.05.006
|
| [62] |
Mehta DD, Praecht A, Ward HB, et al. (2024) A systematic review and meta-analysis of neuromodulation therapies for substance use disorders. Neuropsychopharmacology 49: 649-680. https://doi.org/10.1038/s41386-023-01776-0
|
| [63] | Chan YH, Chang HM, Lu ML, et al. (2023) Targeting cravings in substance addiction with transcranial direct current stimulation: insights from a meta-analysis of sham-controlled trials. Psychiat Res 115621. https://doi.org/10.1016/j.psychres.2023.115621 |
| [64] |
Petit B, Dornier A, Meille V, et al. (2022) Non-invasive brain stimulation for smoking cessation: a systematic review and meta-analysis. Addiction 117: 2768-2779. https://doi.org/10.1111/add.15889
|
| [65] |
Hauer L, Scarano GI, Brigo F, et al. (2019) Effects of repetitive transcranial magnetic stimulation on nicotine consumption and craving: a systematic review. Psychiat Res 281: 112562. https://doi.org/10.1016/j.psychres.2019.112562
|
| [66] |
Zhang JJ, Fong KN, Ouyang RG, et al. (2019) Effects of repetitive transcranial magnetic stimulation (rTMS) on craving and substance consumption in patients with substance dependence: a systematic review and meta-analysis. Addiction 114: 2137-2149. https://doi.org/10.1111/add.14753
|
| [67] |
Shaheen N, Shaheen A, Sarica C, et al. (2023) Deep brain stimulation for substance use disorder: a systematic review and meta-analysis. Front Psychiatry 14: 1231760. https://doi.org/10.3389/fpsyt.2023.1231760
|
| [68] |
Tseng PT, Jeng JS, Zeng BS, et al. (2022) Efficacy of non-invasive brain stimulation interventions in reducing smoking frequency in patients with nicotine dependence: a systematic review and network meta-analysis of randomized controlled trials. Addiction 117: 1830-1842. https://doi.org/10.1111/add.15624
|
| [69] |
Evans DE, To CN, Ashare RL (2019) The role of cognitive control in the self-regulation and reinforcement of smoking behavior. Nicotine Tob Res 21: 747-754. https://doi.org/10.1093/ntr/nty029
|
| [70] |
Flaudias V, Picot MC, Lopez-Castroman J, et al. (2016) Executive functions in tobacco dependence: Importance of inhibitory capacities. PLoS One 11: e0150940. https://doi.org/10.1371/journal.pone.0150940
|
| [71] |
Horvath JC, Forte JD, Carter O (2015) Quantitative review finds no evidence of cognitive effects in healthy populations from single-session transcranial direct current stimulation (tDCS). Brain Stimul 8: 535-550. https://doi.org/10.1016/j.brs.2015.01.400
|
| [72] |
Jentsch JD, Taylor JR (1999) Impulsivity resulting from frontostriatal dysfunction in drug abuse: Implications for the control of behavior by reward-related stimuli. Psychopharmacology (Berl) 146: 373-390. https://doi.org/10.1007/PL00005483
|
| [73] | Janes AC, Krantz NL, Nickerson LD, et al. (2020) Craving and cue reactivity in nicotine-dependent tobacco smokers is associated with different insula networks. Biol Psychiat-Cogn N 5: 76-83. https://doi.org/10.1016/j.bpsc.2019.09.005 |
| [74] |
Bari A, DiCesare J, Babayan D, et al. (2018) Neuromodulation for substance addiction in human subjects: a review. Neurosci Biobehav Rev 95: 33-43. https://doi.org/10.1016/j.neubiorev.2018.09.013
|
| [75] |
Martz ME, Hart T, Heitzeg MM, et al. (2020) Neuromodulation of brain activation associated with addiction: A review of real-time fMRI neurofeedback studies. NeuroImage-Clin 27: 102350. https://doi.org/10.1016/j.nicl.2020.102350
|
| [76] |
Adinoff B (2004) Neurobiologic Processes in Drug Reward and Addiction. Harvard Rev Psychiat 12: 305-320. https://doi.org/10.1080/10673220490910844
|
| [77] |
Tiwari RK, Sharma V, Pandey RK, et al. (2020) Nicotine addiction: Neurobiology and mechanism. J Pharmacopunct 23: 1. https://doi.org/10.3831/KPI.2020.23.001
|
| [78] |
Heinze HJ, Heldmann M, Voges J, et al. (2009) Counteracting incentive sensitization in severe alcohol dependence using deep brain stimulation of the nucleus accumbens: clinical and basic science aspects. Front Hum Neurosci 3: 710. https://doi.org/10.3389/neuro.09.022.2009
|
| [79] |
Zammit Dimech D, Zammit Dimech AA, Hughes M, et al. (2024) A systematic review of deep brain stimulation for substance use disorders. Transl Psychiat 14: 361. https://doi.org/10.1038/s41398-024-03060-1
|
| [80] |
Rabipour S, Davidson PS, Kristjansson E (2018) Measuring expectations of cognitive enhancement: item response analysis of the expectation assessment scale. J Cogn Enhance 2: 311-317. https://doi.org/10.1007/s41465-018-0073-4
|
| [81] |
Cline ME, Herman J, Shaw ER, et al. (1992) Standardization of the visual analogue scale. Nurs Res 41: 378-379. https://doi.org/10.1097/00006199-199211000-00013
|
 neurosci-11-04-027-s001.pdf neurosci-11-04-027-s001.pdf |
 |
Figures(1) / Tables(1)

Graziella Orrù, Marina Baroni, Ciro Conversano, Angelo Gemignani. Exploring the therapeutic potential of tDCS, TMS and DBS in overcoming tobacco use disorder: an umbrella review[J]. AIMS Neuroscience, 2024, 11(4): 449-467. doi: 10.3934/Neuroscience.2024027







 DownLoad:
DownLoad: