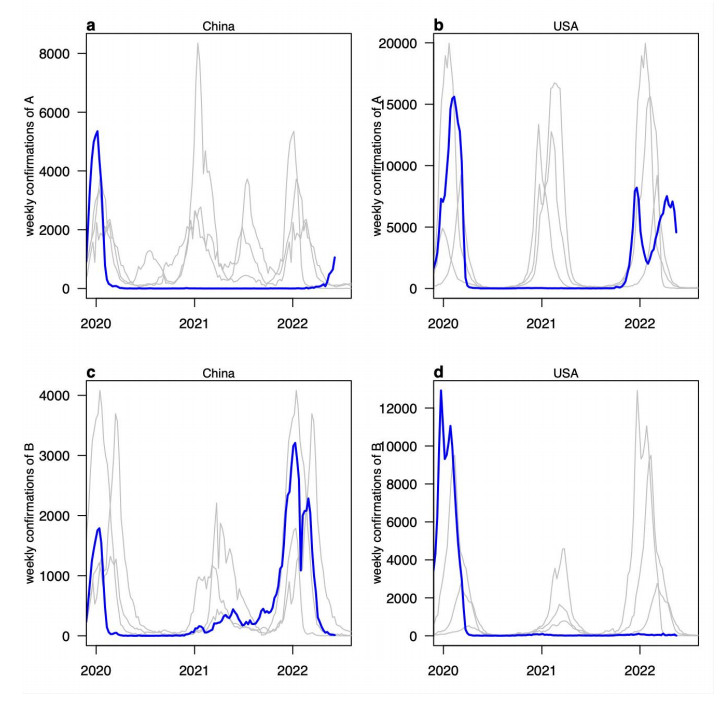
Various nonpharmaceutical interventions (NPIs) were implemented to alleviate the COVID-19 pandemic since its outbreak. The transmission dynamics of other respiratory infectious diseases, such as seasonal influenza, were also affected by these interventions. The drastic decline of seasonal influenza caused by such interventions would result in waning of population immunity and may trigger the seasonal influenza epidemic with the lift of restrictions during the post-pandemic era. We obtained weekly influenza laboratory confirmations from FluNet to analyse the resurgence patterns of seasonal influenza in China and the US. Our analysis showed that due to the impact of NPIs including travel restrictions between countries, the influenza resurgence was caused by influenza virus A in the US while by influenza virus B in China.
Citation: Boqiang Chen, Zhizhou Zhu, Qiong Li, Daihai He. Resurgence of different influenza types in China and the US in 2021[J]. Mathematical Biosciences and Engineering, 2023, 20(4): 6327-6333. doi: 10.3934/mbe.2023273
Various nonpharmaceutical interventions (NPIs) were implemented to alleviate the COVID-19 pandemic since its outbreak. The transmission dynamics of other respiratory infectious diseases, such as seasonal influenza, were also affected by these interventions. The drastic decline of seasonal influenza caused by such interventions would result in waning of population immunity and may trigger the seasonal influenza epidemic with the lift of restrictions during the post-pandemic era. We obtained weekly influenza laboratory confirmations from FluNet to analyse the resurgence patterns of seasonal influenza in China and the US. Our analysis showed that due to the impact of NPIs including travel restrictions between countries, the influenza resurgence was caused by influenza virus A in the US while by influenza virus B in China.

| [1] |
N. Jones, How COVID-19 is changing the cold and flu season, Nature, 588 (2020), 388−390. https://doi.org/10.1038/d41586-020-03519-3 doi: 10.1038/d41586-020-03519-3

|
| [2] | CDC, 2020-2021 Flu season summary [cited 2022 September 05]. Available from: https://www.cdc.gov/flu/season/faq-flu-season-2020-2021.htm. |
| [3] |
D. He, R. Lui, L. Wang, C. K. Tse, L. Yang, L. Stone, Global spatio-temporal patterns of influenza in the post-pandemic era, Sci. Rep., 5 (2015), 1−11. https://doi.org/10.1038/srep11013 doi: 10.1038/srep11013
|
| [4] |
S. T. Ali, Y. C. Lau, S. Shan, S. Ryu, Z. Du, L. Wang, et al., Prediction of upcoming global infection burden of influenza seasons after relaxation of public health and social measures for COVID-19 pandemic, Lancet, 2022 (2022). http://dx.doi.org/10.2139/ssrn.4063811 doi: 10.2139/ssrn.4063811
|
| [5] |
A. Flahault, V. Dias-Ferrao, P. Chaberty, K. Esteves, A. J. Valleron, D. Lavanchy, FluNet as a tool for global monitoring of influenza on the Web, JAMA, 280 (1998), 1330−1332. https://doi.org/10.1001/jama.280.15.1330 doi: 10.1001/jama.280.15.1330
|
| [6] |
M. Chinazzi, J. T. Davis, M. Ajelli, C. Gioannini, M. Litvinova, S. Merler, et al., The effect of travel restrictions on the spread of the 2019 novel coronavirus (COVID-19) outbreak, Science, 368 (2020), 395−400. https://doi.org/10.1126/science.aba9757 doi: 10.1126/science.aba9757
|
| [7] | A. Nowrasteh, A. C. Forrester, How US Travel Restrictions on China Affected the Spread of COVID-19 in the United States, JSTOR, 2020 (2020). Available from: https://www.jstor.org/stable/resrep24847?seq=2. |
| [8] | T. J. Christensen, A modern tragedy? COVID-19 and U.S.-China relations, Brookings Institution, 2020. Available from: https://www.brookings.edu/wp-content/uploads/2020/05/FP_20200507_covid_us_china_christensen_v2.pdf. |
| [9] |
F. Parino, L. Zino, M. Porfiri, A. Rizzo, Modelling and predicting the effect of social distancing and travel restrictions on COVID-19 spreading, J. R. Soc. Interface, 18 (2021), 20200875. https://doi.org/10.1098/rsif.2020.0875 doi: 10.1098/rsif.2020.0875
|
| [10] |
K. Linka, M. Peirlinck, F. S. Costabal, E. Kuhl, Outbreak dynamics of COVID-19 in Europe and the effect of travel restrictions, Comput. Methods Biomech. Biomed. Eng., 23 (2020), 710−717. https://doi.org/10.1080/10255842.2020.1759560 doi: 10.1080/10255842.2020.1759560
|
| [11] |
L. Zheng, J. Qi, J. Wu, M. Zheng, Changes in influenza activity and circulating subtypes during the COVID-19 outbreak in China, Front. Med., 2022 (2022), 627. https://doi.org/10.3389/fmed.2022.829799 doi: 10.3389/fmed.2022.829799
|
| [12] |
S. Han, T. Zhang, Y. Lyu, S. Cai, P. Dai, J. Zheng, et al., The incoming influenza season—China, the United Kingdom, and the United States, 2021–2022, China CDC Wkly., 3 (2021), 1039−1045. https://doi.org/10.46234/ccdcw2021.253 doi: 10.46234/ccdcw2021.253
|
| [13] |
B. J. Cowling, S. T. Ali, T. W. Y. Ng, T. K. Tsang, J. C. M. Li, M. W. Fong, et al., Impact assessment of non-pharmaceutical interventions against coronavirus disease 2019 and influenza in Hong Kong: an observational study, Lancet Public Health, 5 (2020), e279−e288. https://doi.org/10.1016/S2468-2667(20)30090-6 doi: 10.1016/S2468-2667(20)30090-6
|
| [14] |
A. Merced-Morales, P. Daly, A. I. A. Elal, N. Ajayi, E. Annan, A. Budd, et al., Influenza activity and composition of the 2022–23 influenza vaccine—United States, 2021–22 season, Morb. Mortal. Wkly. Rep., 71 (2022), 913. https://doi.org/10.15585/mmwr.mm7129a1 doi: 10.15585/mmwr.mm7129a1
|
| [15] |
M. Koutsakos, A. K. Wheatley, K. Laurie, S. J. Kent, S. Rockman, Influenza lineage extinction during the COVID-19 pandemic? Nat. Rev. Microbiol., 19 (2021), 741−742. https://doi.org/10.1038/s41579-021-00642-4 doi: 10.1038/s41579-021-00642-4
|
| [16] | CDC, Influenza vaccination coverage for persons 6 months and older [cited 2023 January 05]. Available from: https://www.cdc.gov/flu/fluvaxview/interactive-general-population.htm. |
| [17] |
J. Yang, K. E. Atkins, L. Feng, M. Pang, Y. Zheng, X. Liu, et al., Seasonal influenza vaccination in China: landscape of diverse regional reimbursement policy, and budget impact analysis, Vaccine, 34 (2016), 5724−5735. https://doi.org/10.1016/j.vaccine.2016.10.013 doi: 10.1016/j.vaccine.2016.10.013
|
| [18] |
J. Fan, S. Cong, N. Wang, H. Bao, B. Wang, Y. Feng, et al., Influenza vaccination rate and its association with chronic diseases in China: results of a national cross-sectional study, Vaccine, 38 (2020), 2503−2511. https://doi.org/10.1016/j.vaccine.2020.01.093 doi: 10.1016/j.vaccine.2020.01.093
|
 mbe-20-04-273-supplementary.pdf mbe-20-04-273-supplementary.pdf |
 |
Figures(2)

Boqiang Chen, Zhizhou Zhu, Qiong Li, Daihai He. Resurgence of different influenza types in China and the US in 2021[J]. Mathematical Biosciences and Engineering, 2023, 20(4): 6327-6333. doi: 10.3934/mbe.2023273







 DownLoad:
DownLoad: