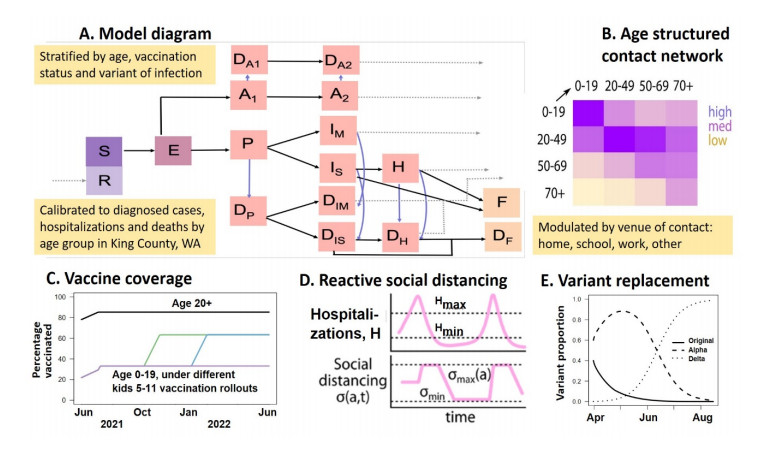
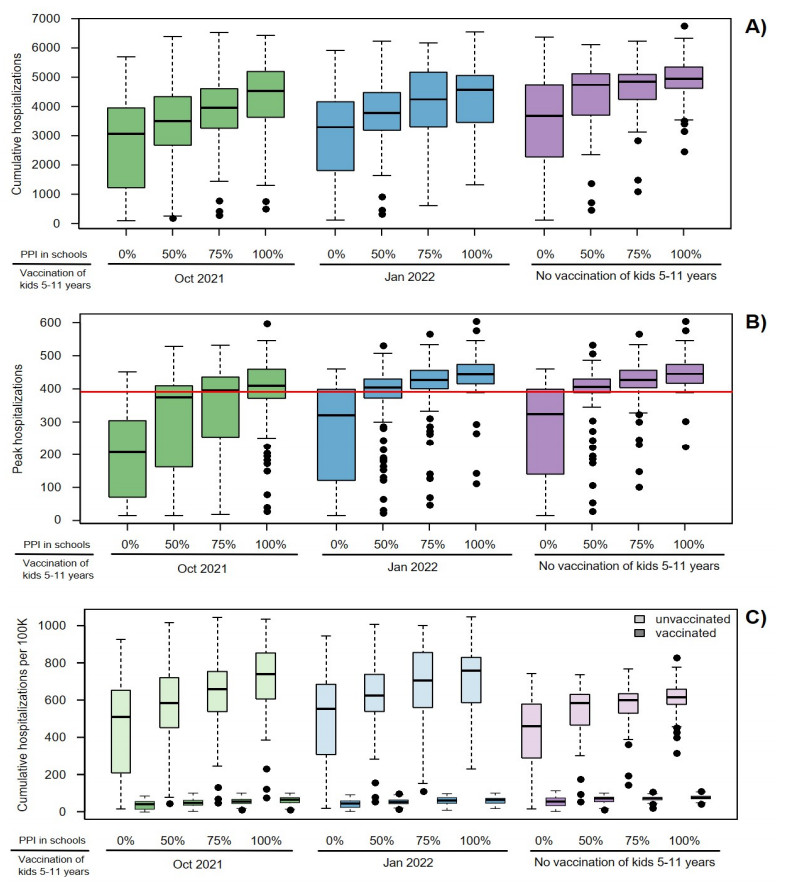
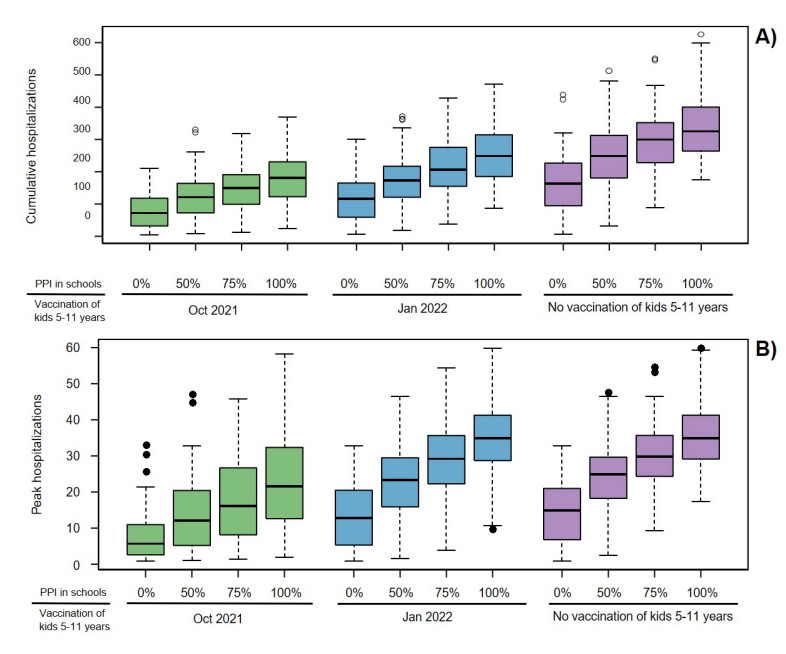
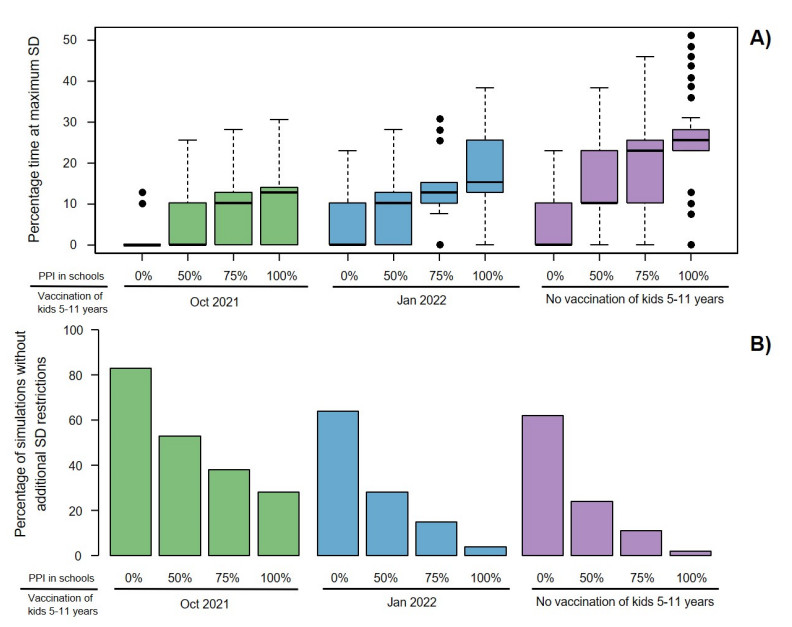
The rapid spread of highly transmissible SARS-CoV-2 variants combined with slowing pace of vaccination in Fall 2021 created uncertainty around the future trajectory of the epidemic in King County, Washington, USA. We analyzed the benefits of offering vaccination to children ages 5–11 and expanding the overall vaccination coverage using mathematical modeling. We adapted a mathematical model of SARS-CoV-2 transmission, calibrated to data from King County, Washington, to simulate scenarios of vaccinating children aged 5–11 with different starting dates and different proportions of physical interactions (PPI) in schools being restored. Dynamic social distancing was implemented in response to changes in weekly hospitalizations. Reduction of hospitalizations and estimated time under additional social distancing measures are reported over the 2021–2022 school year. In the scenario with 85% vaccination coverage of 12+ year-olds, offering early vaccination to children aged 5–11 with 75% PPI was predicted to prevent 756 (median, IQR 301–1434) hospitalizations cutting youth hospitalizations in half compared to no vaccination and largely reducing the need for additional social distancing measures over the school year. If, in addition, 90% overall vaccination coverage was reached, 60% of remaining hospitalizations would be averted and the need for increased social distancing would almost certainly be avoided. Our work suggests that uninterrupted in-person schooling in King County was partly possible because reasonable precaution measures were taken at schools to reduce infectious contacts. Rapid vaccination of all school-aged children provides meaningful reduction of the COVID-19 health burden over this school year but only if implemented early. It remains critical to vaccinate as many people as possible to limit the morbidity and mortality associated with future epidemic waves.
Citation: Chloe Bracis, Mia Moore, David A. Swan, Laura Matrajt, Larissa Anderson, Daniel B. Reeves, Eileen Burns, Joshua T. Schiffer, Dobromir Dimitrov. Improving vaccination coverage and offering vaccine to all school-age children allowed uninterrupted in-person schooling in King County, WA: Modeling analysis[J]. Mathematical Biosciences and Engineering, 2022, 19(6): 5699-5716. doi: 10.3934/mbe.2022266
The rapid spread of highly transmissible SARS-CoV-2 variants combined with slowing pace of vaccination in Fall 2021 created uncertainty around the future trajectory of the epidemic in King County, Washington, USA. We analyzed the benefits of offering vaccination to children ages 5–11 and expanding the overall vaccination coverage using mathematical modeling. We adapted a mathematical model of SARS-CoV-2 transmission, calibrated to data from King County, Washington, to simulate scenarios of vaccinating children aged 5–11 with different starting dates and different proportions of physical interactions (PPI) in schools being restored. Dynamic social distancing was implemented in response to changes in weekly hospitalizations. Reduction of hospitalizations and estimated time under additional social distancing measures are reported over the 2021–2022 school year. In the scenario with 85% vaccination coverage of 12+ year-olds, offering early vaccination to children aged 5–11 with 75% PPI was predicted to prevent 756 (median, IQR 301–1434) hospitalizations cutting youth hospitalizations in half compared to no vaccination and largely reducing the need for additional social distancing measures over the school year. If, in addition, 90% overall vaccination coverage was reached, 60% of remaining hospitalizations would be averted and the need for increased social distancing would almost certainly be avoided. Our work suggests that uninterrupted in-person schooling in King County was partly possible because reasonable precaution measures were taken at schools to reduce infectious contacts. Rapid vaccination of all school-aged children provides meaningful reduction of the COVID-19 health burden over this school year but only if implemented early. It remains critical to vaccinate as many people as possible to limit the morbidity and mortality associated with future epidemic waves.

| [1] | Centers for Disease Control and Prevention, Interim Public Health Recommendations for Fully Vaccinated People, 2019. Available from: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/fully-vaccinated-guidance.html#anchor_1619526549276. |
| [2] | Centers for Disease Control and Prevention, Covid Data Tracker: Variant Proportions, Available from: https://covid.cdc.gov/covid-data-tracker/#variant-proportions. |
| [3] | Washington State Department of Health, SARS-CoV-2 Sequencing and Variants in Washington State Washington State Department of Health, 2021. Available from: https://www.doh.wa.gov/Portals/1/Documents/1600/coronavirus/data-tables/420-316-SequencingAndVariantsReport.pdf. |
| [4] |
D. Fisman, A. Tuite, Progressive increase in virulence of novel SARS-CoV-2 variants in Ontario, Canada, medRxiv, (2021). https://doi.org/10.1101/2021.07.05.21260050 doi: 10.1101/2021.07.05.21260050

|
| [5] |
A. Sheikh, J. McMenamin, B. Taylor, C. Robertson, SARS-CoV-2 Delta VOC in Scotland: demographics, risk of hospital admission, and vaccine effectiveness, Lancet, 397 (2021), 2461–2462. https://doi.org/10.1016/S0140-6736(21)01358-1 doi: 10.1016/S0140-6736(21)01358-1
|
| [6] |
F. Campbell, B. Archer, H. Laurenson-Schafer, Y. Jinnai, F. Konings, N. Batra, et al., Increased transmissibility and global spread of SARSCoV-2 variants of concern as at June 2021, Eurosurveillance, 26 (2021), 1–6. https://doi.org/10.2807/1560-7917.ES.2021.26.24.2100509 doi: 10.2807/1560-7917.ES.2021.26.24.2100509
|
| [7] | M. G. Thompson, K. Natarajan, S. A. Irving, E. A. Rowley, E. P. Griggs, M. Gaglani, et al., Effectiveness of a third dose of mRNA vaccines against COVID-19—associated emergency department and urgent care encounters and hospitalizations among adults during periods of Delta and Omicron variant predominance—VISION Network, 10 States, August 2021–January 2022, Morb. Mortal. Wkly. Rep., 71 (2022), 1–8. |
| [8] | UK Health Security Agency, SARS-CoV-2 Variants of Concern and Variants under Investigation in England Technical Briefing 34, Available from: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1050236/technical-briefing-34-14-january-2022.pdf. |
| [9] |
S. Y. Tartof, J. M. Slezak, H. Fischer, V. Hong, B. K. Ackerson, O. N. Ranasinghe, et al., Effectiveness of mRNA BNT162b2 COVID-19 vaccine up to 6 months in a large integrated health system in the USA: a retrospective cohort study, Lancet, 398 (2021), 1407–1416, https://doi.org/10.1016/S0140-6736(21)02183-8 doi: 10.1016/S0140-6736(21)02183-8
|
| [10] |
M. Chadeau-Hyam, H. Wang, O. Eales, D. Haw, B. Bodinier, M. Whitaker, et al., SARS-CoV-2 infection and vaccine effectiveness in England (REACT-1): a series of cross-sectional random community surveys, Lancet Respir. Med., (2022). https://doi.org/10.1016/s2213-2600(21)00542-7 doi: 10.1016/s2213-2600(21)00542-7
|
| [11] |
E. Vasileiou, T. Shi, S. Kerr, C. Robertson, M. Joy, R. Tsang, et al., Investigating the uptake, effectiveness and safety of COVID-19 vaccines: protocol for an observational study using linked UK national data, BMJ Open, 12 (2022), e050062. https://doi.org/10.1016/s2213-2600(21)00542-7 doi: 10.1016/s2213-2600(21)00542-7
|
| [12] |
N. Andrews, E. Tessier, J. Stowe, C. Gower, F. Kirseborn, R. Simmons, et al., Vaccine effectiveness and duration of protection of Comirnaty, Vaxzevria and Spikevax against mild and severe COVID-19 in the UK, medRxiv, (2021). https://doi.org/10.1101/2021.09.15.21263583 doi: 10.1101/2021.09.15.21263583
|
| [13] |
J. Yu, A. R. Y. Collier, M. Rowe, F. Mardas, J. D. Ventura, H. Wan, et al., Comparable neutralization of the SARS-CoV-2 omicron BA.1 and BA.2 variants, medRxiv, (2022). https://doi.org/10.1101/2022.02.06.22270533 doi: 10.1101/2022.02.06.22270533
|
| [14] |
M. S. Rane, M. Robertson, S. Kulkarni, D. Frogel, C. Gainus, D. Nash, Effectiveness of Covid-19 vaccines against symptomatic and asymptomatic SARS-CoV-2 infections in an urgent care setting, medRxiv, (2022). https://doi.org/10.1101/2022.02.21.22271298 doi: 10.1101/2022.02.21.22271298
|
| [15] | Pfizer BioNTech, Pfizer and BioNTech Announce Positive Topline Results from Pivotal Trial of COVID-19 Vaccine in Children 5 to 11 Years, 2021. Available from: https://www.businesswire.com/news/home/20210920005452/en/. |
| [16] | U.S. Food & Drug Administration, Advisory Committee Meeting Vaccines and Related Biological Products Advisory Committee October 26, 2021 Meeting Announcement, 2021. Available from: https://www.fda.gov/advisory-committees/advisory-committee-calendar/vaccines-and-related-biological-products-advisory-committee-october-26-2021-meeting-announcement. |
| [17] | King County, Summary of COVID-19 Vaccination among King County Residents, Available from: https://kingcounty.gov/depts/health/covid-19/data/vaccination.aspx. |
| [18] | Washington Governor Jay Inslee, Inslee Signs Emergency Proclamation Requiring in-person Education Opportunities for Public K-12 Schools, Available from: https://www.governor.wa.gov/news-media/inslee-signs-emergency-proclamation-requiring-person-education-opportunities-public-k-12. |
| [19] |
L. Matrajt, H. Janes, J. T. Schiffer, D. Dimitrov, Quantifying the impact of lifting community nonpharmaceutical interventions for COVID-19 during vaccination rollout in the United States, Open Forum Infect. Dis., 8 (2021). https://doi.org/10.1093/ofid/ofab341 doi: 10.1093/ofid/ofab341
|
| [20] |
S. J. de Vlas, L. E. Coffeng, Achieving herd immunity against COVID-19 at the country level by the exit strategy of a phased lift of control, Sci. Rep., 11 (2021), 1–7. https://doi.org/10.1038/s41598-021-83492-7 doi: 10.1038/s41598-021-83492-7
|
| [21] |
M. Baniasad, M. G. Mofrad, B. Bahmanabadi, S. Jamshidi, COVID-19 in Asia: Transmission factors, re-opening policies, and vaccination simulation, Environ. Res., 202 (2021), 111657. https://doi.org/10.1016/j.envres.2021.111657 doi: 10.1016/j.envres.2021.111657
|
| [22] |
M. Coccia, Optimal levels of vaccination to reduce COVID-19 infected individuals and deaths: A global analysis, Environ. Res., 204 (2021), 112314. https://doi.org/10.1016/j.envres.2021.112314 doi: 10.1016/j.envres.2021.112314
|
| [23] |
S. M. Moghadas, T. N. Vilches, K. Zhang, C. R. Wells, A. Shoukat, B. H. Singer, et al., The Impact of vaccination on coronavirus disease 2019 (COVID-19) outbreaks in the United States, Clin. Infect. Dis., 73 (2021), 2257–2264. https://doi.org/10.1093/cid/ciab079 doi: 10.1093/cid/ciab079
|
| [24] |
Y. Zhang, K. Johnson, K. H. Lich, J. Ivy, P. Keskinocak, M. Mayorga, et al., COVID-19 projections for K12 schools in fall 2021: significant transmission without interventions, medRxiv, (2021). https://doi.org/10.1101/2021.08.10.21261726 doi: 10.1101/2021.08.10.21261726
|
| [25] |
P. Yuan, E. Aruffo, E. Gatov, Y. Tan, Q. Li, N. Ogden, et al., School and community reopening during the COVID-19 pandemic: a mathematical modelling study, R. Soc. Open Sci., 9 (2022), 1–13. https://doi.org/10.1098/rsos.211883 doi: 10.1098/rsos.211883
|
| [26] |
R. S. Mcgee, J. R. Homburger, H. E. Williams, C. T. Bergstrom, A. Y. Zhou, Model-driven mitigation measures for reopening schools during the COVID-19 pandemic, Proc. Nat. Acad. Sci., 118 (2021), 1–10. https://doi.org/10.1073/pnas.2108909118 doi: 10.1073/pnas.2108909118
|
| [27] |
J. Lessler, M. K. Grabowski, K. H. Grantz, E. Badillo-goicoechea, C. J. E. Metcalf, A. S. Azman, et al., Household COVID-19 risk and in-person schooling, Science, 2939 (2021), 1–10. https://doi.org/10.1093/cid/ciab079 doi: 10.1093/cid/ciab079
|
| [28] |
C. Bracis, E. Burns, M. Moore, D. Swan, D. B. Reeves, J. T. Schiffer, et al., Widespread testing, case isolation and contact tracing may allow safe school reopening with continued moderate physical distancing: A modeling analysis of King County, WA data, Infect. Dis. Modell., 6 (2021), 24–35. https://doi.org/10.1016/j.idm.2020.11.003 doi: 10.1016/j.idm.2020.11.003
|
| [29] | Y. Zhang, K. Johnson, Z. Yu, A. B. Fujimoto, K. H. Lich, J. Ivy, et al., medRxiv, (2021). https://doi.org/10.1101/2021.08.10.21261726 |
| [30] |
D. B. Reeves, C. Bracis, D. A. Swan, E. Burns, M. Moore, D. Dimitrov, et al., Rapid vaccination and partial lockdown minimize 4th waves from emerging highly contagious SARS-CoV-2 variants, Med, 2 (2021), 573–574. https://doi.org/10.1016/j.idm.2020.11.003 doi: 10.1016/j.idm.2020.11.003
|
| [31] |
D. A. Swan, C. Bracis, H. Janes, M. Moore, L. Matrajt, D. B. Reeves, et al., COVID-19 vaccines that reduce symptoms but do not block infection need higher coverage and faster rollout to achieve population impact, Sci. Rep., 11 (2021), 1–9. https://doi.org/10.1038/s41598-021-94719-y doi: 10.1038/s41598-021-94719-y
|
| [32] |
D. A. Swan, A. Goyal, C. Bracis, M. Moore, E. Krantz, E. Brown, et al., Mathematical modeling of vaccines that prevent SARS-CoV-2 transmission, Viruses, 13 (2021), 1921. https://doi.org/10.3390/v13101921 doi: 10.3390/v13101921
|
| [33] |
X. He, E. H. Y. Lau, P. Wu, X. Deng, J. Wang, X. Hao, et al., Temporal dynamics in viral shedding and transmissibility of COVID-19, Nat. Med., 26 (2020), 672–675. https://doi.org/10.1038/s41591-020-0869-5 doi: 10.1038/s41591-020-0869-5
|
| [34] |
L. Ferretti, C. Wymant, M. Kendall, L. Zhao, A. Nurtay, L. Abeler-Dörner, et al., Quantifying SARS-CoV-2 transmission suggests epidemic control with digital contact tracing, Science, 368 (2020), 1–8. https://doi.org/10.1126/science.abb6936 doi: 10.1126/science.abb6936
|
| [35] |
K. Prem, K. van Zandvoort, P. Klepac, R. M. Eggo, N. G. Davies, A. R. Cook, et al., Projecting contact matrices in 177 geographical regions: An update and comparison with empirical data for the COVID-19 era, PLoS Comput. Biol., 17 (2021), e1009098. https://doi.org/10.1371/journal.pcbi.1009098 doi: 10.1371/journal.pcbi.1009098
|
| [36] | King County, Key Indicators of COVID-19 Activity in King County, Available from: https://kingcounty.gov/depts/health/covid-19/data.aspx. |
| [37] |
M. A. Beaumont, J. M. Cornuet, J. M. Marin, C. P. Robert, Adaptive approximate Bayesian computation, Biometrika, 96 (2009), 983–990. https://doi.org/10.1093/biomet/asp052 doi: 10.1093/biomet/asp052
|
| [38] | Health and Human Services, Hospital Utilization, Available from: https://protect-public.hhs.gov/pages/hospital-utilization. |
| [39] | M. Jehn, J. mac Mccullough, A. P. Dale, M. Gue, B. Eller, T. Cullen, et al., Association between K-12 school mask policies and school-associated COVID-19 outbreaks—Maricopa and Pima Counties, Arizona, July–August 2021, Morb. Mortal. Wkly. Rep., 70 (2021), 2020–2022. http://dx.doi.org/10.15585/mmwr.mm7039e1 |
| [40] | S. E. Budzyn, M. J. Panaggio, S. E. Parks, M. Papazian, J. Magid, L. C. Barrios, Pediatric COVID-19 cases in counties with and without school mask requirements—United States, July 1–September 4, 2021, Morb. Mortal. Wkly. Rep., 70 (2021), 21–23. http://dx.doi.org/10.15585/mmwr.mm7039e3 |
| [41] | CNN, These 5 States Have Less than 10% of ICU Beds Left as Covid-19 Overwhelms Hospitals, Available from: https://www.cnn.com/2021/08/31/health/us-coronavirus-tuesday/index.html. |
| [42] | Mississippi's Hospital System Could Collapse Within 10 Days Under COVID's Strain, Available from: https://www.npr.org/2021/08/12/1027103023/florida-mississippi-arkansas-hospitals-overwhelmed-covid-19-delta. |
| [43] | American Academy of Pediatrics, Children and COVID-19 state data report version 6/24/21, 2021. |
| [44] | M. J. Delahoy, D. Ujamaa, M. Whitaker, A. O'Halloran, O. Anglin, et al., Hospitalizations associated with COVID-19 among children and adolescents—COVID-NET, 14 States, March 1, 2020–August 14, 2021, Morb. Mortal. Wkly. Rep., 70 (2021), 1255–1260. http://dx.doi.org/10.15585/mmwr.mm7036e2 |
| [45] | Covid-19 Vaccine Tracker: How many people have been inoculated in Ireland? Irish Times, Available from: https://www.irishtimes.com/news/health/covid-19-vaccine-tracker-how-many-people-have-been-inoculated-in-ireland-1.4481095. |
| [46] |
J. Abaluck, L. H. Kwong, A. Styczynski, A. Haque, A. Kabir, E. Bates-jeffries, et al., The impact of community masking on COVID-19: a cluster-randomized trial in Bangladesh, Science, 375 (2022), 6577. https://doi.org/10.1126/science.abi9069 doi: 10.1126/science.abi9069
|
| [47] | Washington State Department of Health, Healthy Washington: Roadmap to Recovery Report, 2021. Available from: https://coronavirus.wa.gov/sites/default/files/2021-04/421-006-RoadmapToRecovery-20210412.pdf |
| [48] |
J. L. Bernal, N. Andrews, C. Gower, E. Gallagher, R. Simmons, S. Thelwall, et al., Effectiveness of COVID-19 vaccines against the B.1.617.2 variant, medRxiv, (2021). https://doi.org/10.1101/2021.05.22.21257658 doi: 10.1101/2021.05.22.21257658
|
| [49] |
J. Stowe, N. Andrews, C. Gower, E. Gallagher, L. Utsi, R. Simmons, et al., Effectiveness of COVID-19 vaccines against hospital admission with the Delta (B.1.617.2) variant, medRxiv, (2021). https://doi.org/10.1101/2021.09.15.21263583 doi: 10.1101/2021.09.15.21263583
|
| [50] |
N. G. Davies, S. Abbott, R. C. Barnard, C. I. Jarvis, A. J. Kucharski, J. D. Munday, et al., Estimated transmissibility and impact of SARS-CoV-2 lineage B.1.1.7 in England, Science, 372 (2021), eabg3055. https://doi.org/10.1126/science.abg3055 doi: 10.1126/science.abg3055
|
| [51] |
E. Volz, S. Mishra, M. Chand, J. C. Barrett, R. Johnson, L. Geidelberg, et al., Assessing transmissibility of SARS-CoV-2 lineage B.1.1.7 in England, Nature, 593 (2021), 266–269. https://doi.org/10.1038/s41586-021-03470-x doi: 10.1038/s41586-021-03470-x
|
| [52] |
A. M. S. Dhar, R. Marwal, R. Vs, K. Ponnusamy, Genomic characterization and epidemiology of an emerging SARS-CoV-2 variant in Delhi, India Affiliations, medRxiv, (2021), 1–17. https://doi.org/10.1101/2021.06.02.21258076 doi: 10.1101/2021.06.02.21258076
|
| [53] | Public Health England, SARS-CoV-2 Variants of Concern and Variants under Investigation in England, 2021. Available from: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/993879/Variants_of_Concern_VOC_Technical_Briefing_15.pdf. |
| [54] |
J. Dagpunar, Interim estimates of increased transmissibility, growth rate, and reproduction number of the Covid-19 B.1.617.2 variant of concern in the United Kingdom, medRxiv, (2021). https://doi.org/10.1101/2021.06.03.21258293 doi: 10.1101/2021.06.03.21258293
|
| [55] |
S. W. X. Ong, C. J. Chiew, L. W. Ang, T. M. Mak, L. Cui, M. P. H. S. Toh, et al., Clinical and virological features of SARS-CoV-2 variants of concern: a retrospective cohort study comparing B.1.1.7 (Alpha), B.1.315 (Beta), and B.1.617.2 (Delta), Clin. Infect. Dis., (2021). https://doi.org/10.1093/cid/ciab721 doi: 10.1093/cid/ciab721
|
| [56] |
N. G. Davies, P. Klepac, Y. Liu, K. Prem, M. Jit, C. A. B. Pearson, et al., Age-dependent effects in the transmission and control of COVID-19 epidemics, Nat. Med., 26 (2020), 1205–1211. https://doi.org/10.1038/s41591-020-0962-9 doi: 10.1038/s41591-020-0962-9
|
 mbe-19-06-266-supplementary.pdf mbe-19-06-266-supplementary.pdf |
 |
Figures(6) / Tables(2)

Chloe Bracis, Mia Moore, David A. Swan, Laura Matrajt, Larissa Anderson, Daniel B. Reeves, Eileen Burns, Joshua T. Schiffer, Dobromir Dimitrov. Improving vaccination coverage and offering vaccine to all school-age children allowed uninterrupted in-person schooling in King County, WA: Modeling analysis[J]. Mathematical Biosciences and Engineering, 2022, 19(6): 5699-5716. doi: 10.3934/mbe.2022266







 DownLoad:
DownLoad: