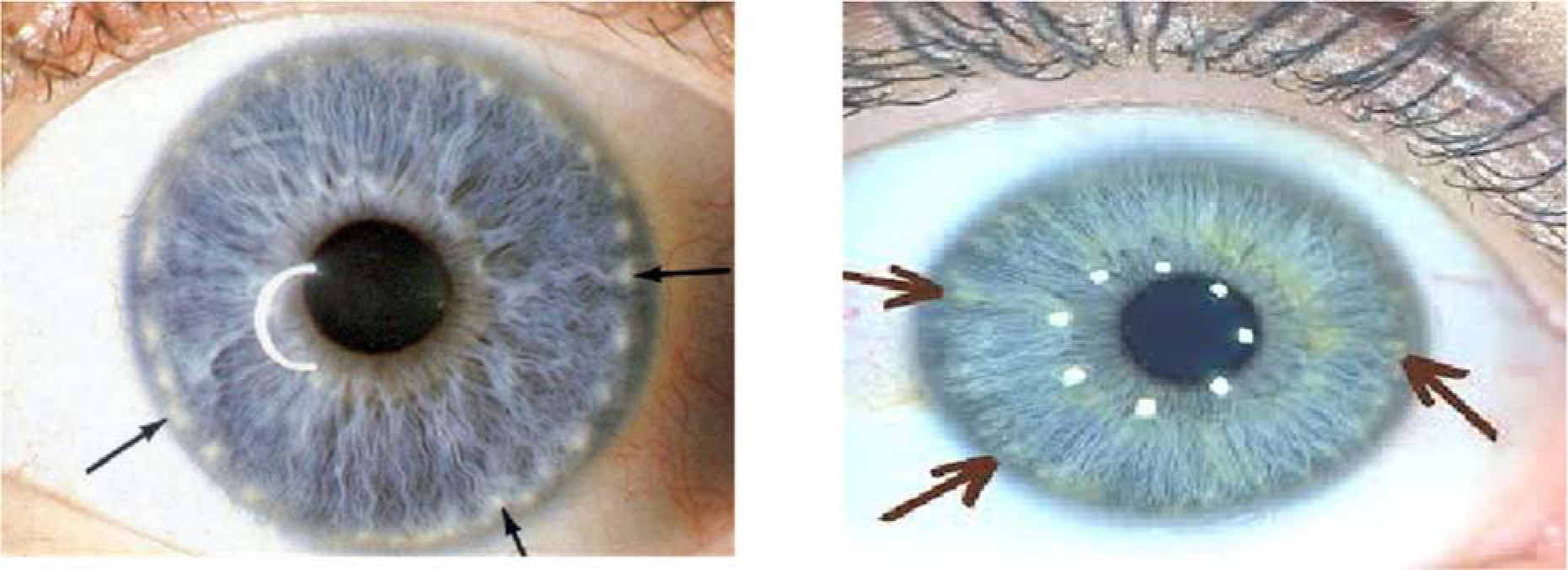
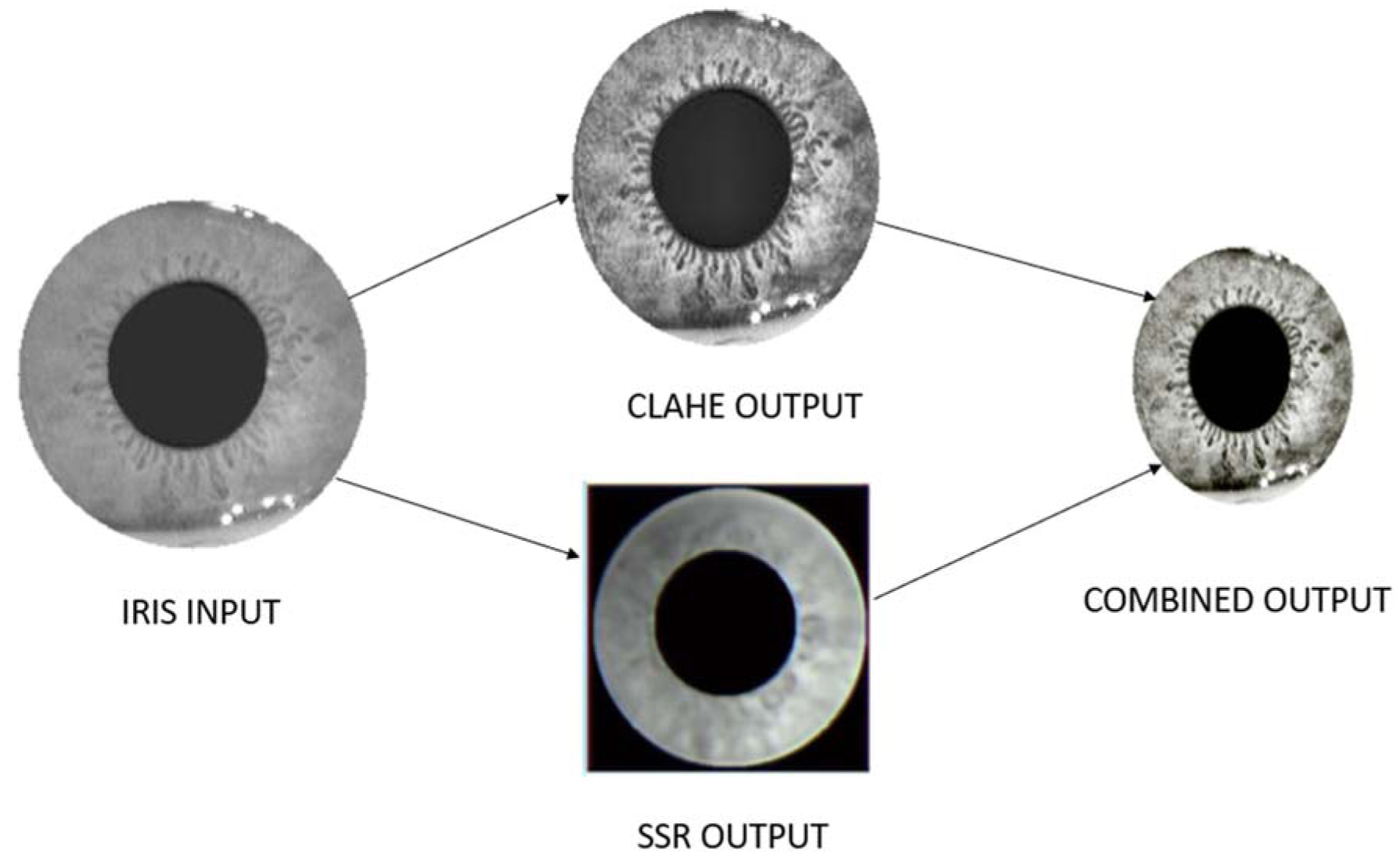
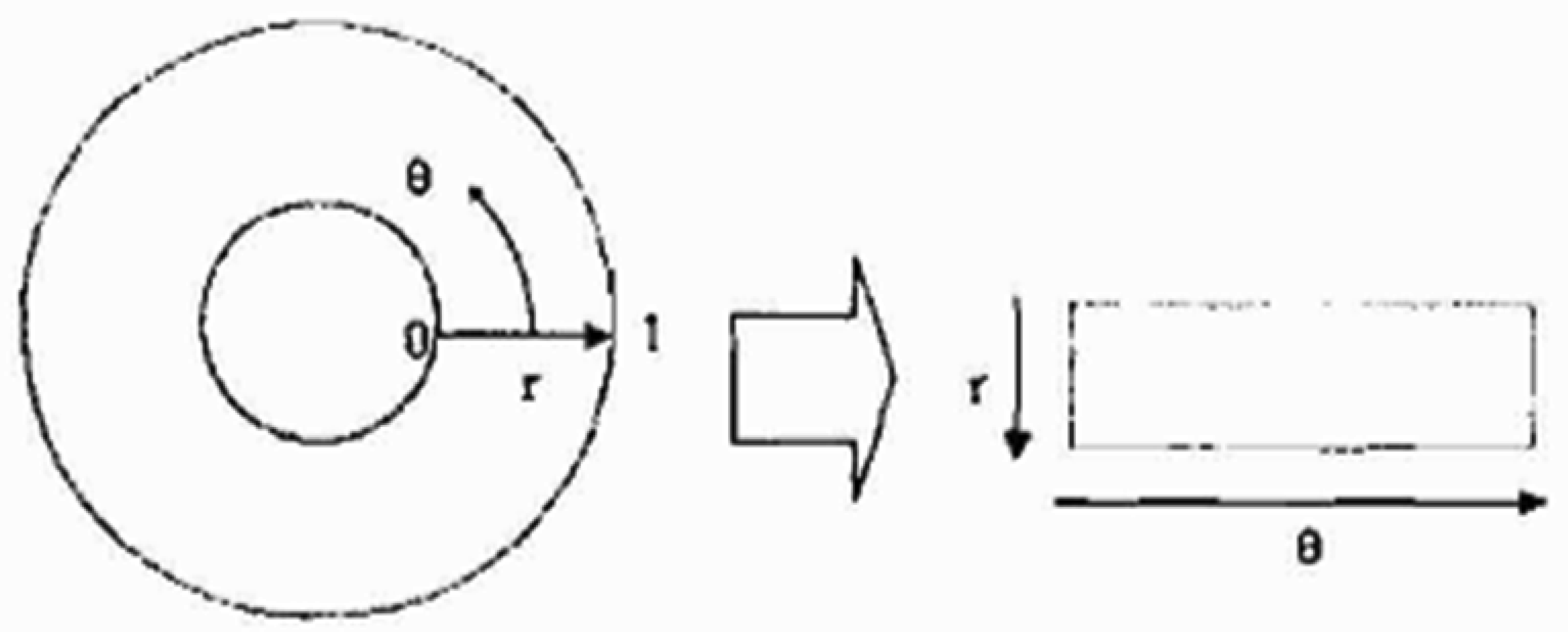
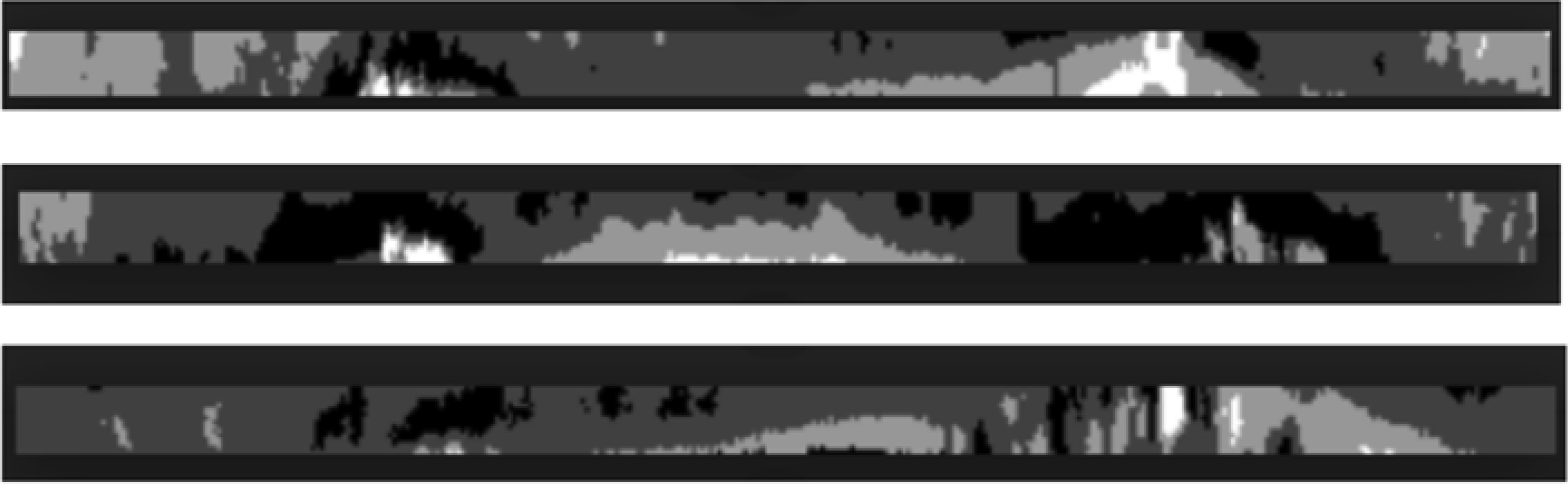
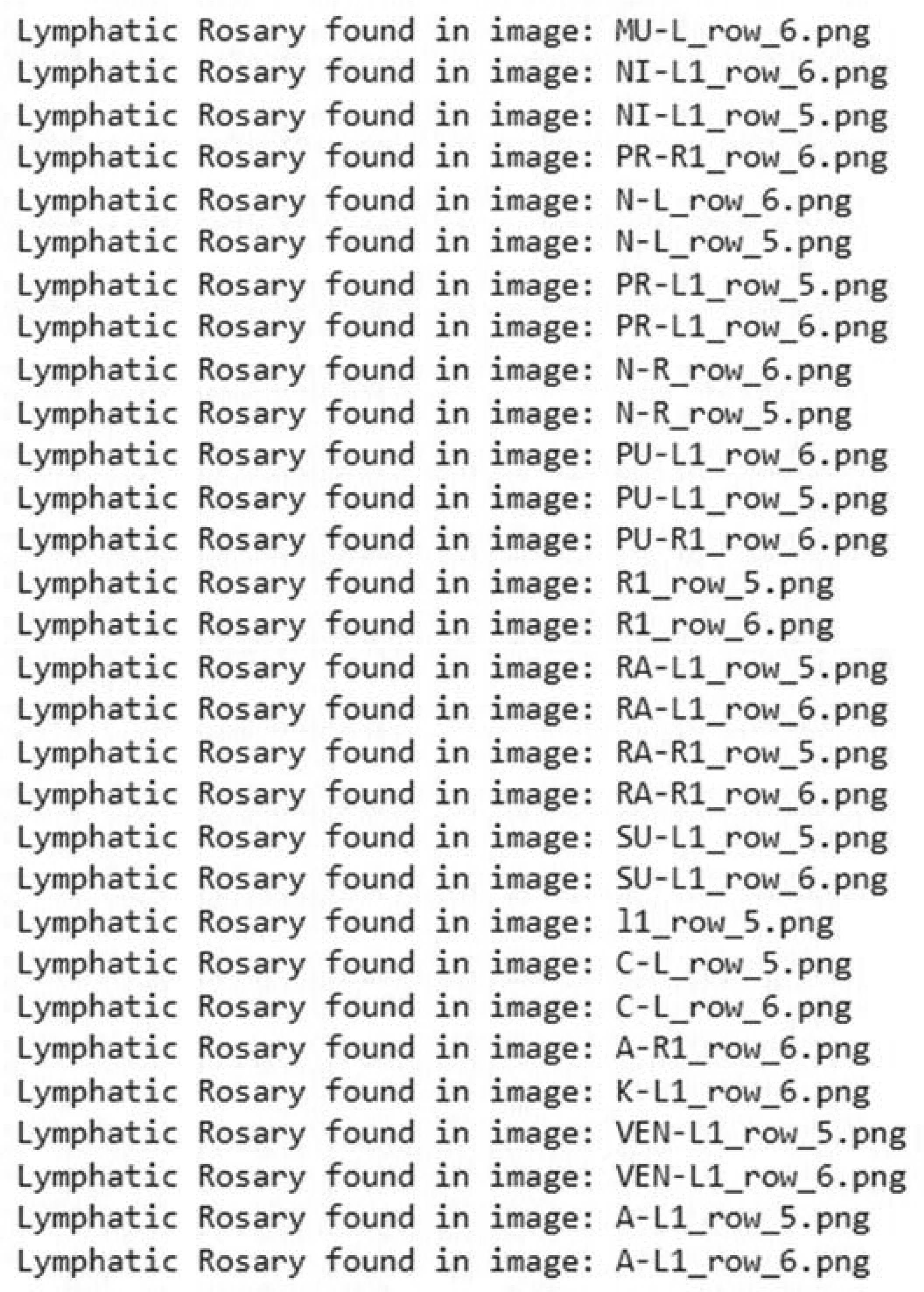
Lymphatic dysfunction is characterized by the sluggish movement of lymph fluids. It manifests as a “Lymphatic Rosary” in the iris which is often due to dehydration and inactivity. Detecting these signs early is crucial for diagnosis and treatment. Therefore, there is a need for an automated, accurate, and efficient method to detect lymphatic rosaries in the iris. This paper presents a novel approach for detecting a lymphatic rosary using advanced image processing techniques. The proposed method involves iris segmentation to isolate the iris from the eye, followed by normalization to standardize its structure, and concludes with the application of the modified Daugman method to identify the lymphatic rosary. This automated process aims to enhance the accuracy and reliability of detection by minimizing the subjectivity associated with manual analysis. The proposed approach was tested on various iris images and the results demonstrated impressive accuracy in detecting lymphatic rosaries. The use of different iris code bit representations allowed for a robust detection process, showcasing the method's effectiveness by achieving an accuracy of 94.5% in identifying the presence of a lymphatic rosary across different stages. The novel image processing technique outlined in this paper offers a promising solution for the automated detection of lymphatic rosaries in the iris. The approach not only improves diagnostic accuracy but also provides a standardized method that could be widely implemented in clinical settings. This advancement in iris diagnosis has the potential to play a significant role in the early detection and management of lymphatic dysfunction.
Citation: Poovayar Priya Mohan, Ezhilarasan Murugesan. A novel approach for detecting the presence of a lymphatic rosary in the iris using a 3-stage algorithm[J]. AIMS Bioengineering, 2024, 11(4): 506-526. doi: 10.3934/bioeng.2024023
Lymphatic dysfunction is characterized by the sluggish movement of lymph fluids. It manifests as a “Lymphatic Rosary” in the iris which is often due to dehydration and inactivity. Detecting these signs early is crucial for diagnosis and treatment. Therefore, there is a need for an automated, accurate, and efficient method to detect lymphatic rosaries in the iris. This paper presents a novel approach for detecting a lymphatic rosary using advanced image processing techniques. The proposed method involves iris segmentation to isolate the iris from the eye, followed by normalization to standardize its structure, and concludes with the application of the modified Daugman method to identify the lymphatic rosary. This automated process aims to enhance the accuracy and reliability of detection by minimizing the subjectivity associated with manual analysis. The proposed approach was tested on various iris images and the results demonstrated impressive accuracy in detecting lymphatic rosaries. The use of different iris code bit representations allowed for a robust detection process, showcasing the method's effectiveness by achieving an accuracy of 94.5% in identifying the presence of a lymphatic rosary across different stages. The novel image processing technique outlined in this paper offers a promising solution for the automated detection of lymphatic rosaries in the iris. The approach not only improves diagnostic accuracy but also provides a standardized method that could be widely implemented in clinical settings. This advancement in iris diagnosis has the potential to play a significant role in the early detection and management of lymphatic dysfunction.

| [1] |
Sharan F (1989) Iridology: A Complete Guide to Diagnosing through the Iris and to Related Forms of Treatment. New York: HarperThorsons. |
| [2] | Jensen B (1980) Iridology Simplified. Canada: Book Publishing Company. |
| [3] | Kryzhanivska O (2020) Iris changes at patients with temporomandibular joint diseases and urinary system pathology. MSU 16: 28-34. https://doi.org/10.32345/2664-4738.4.2020.5 |
| [4] |
Sen M, Honavar SG (2022) Theodor karl gustav von leber: the sultan of selten. Indian J Ophthalmol 70: 2218-2220. https://doi.org/10.4103/ijo.IJO_1379_22 
|
| [5] | de Oliveira ER, de Souza Cardoso J, da Silva Rodrigues VT, et al. (2023) Nocardia niwae infection in dogs. Acta Sci Vet 51: 900. https://doi.org/10.22456/1679-9216.131057 |
| [6] |
Caruso M, Catalano O, Bard R, et al. (2022) Non-glandular findings on breast ultrasound. Part I: a pictorial review of superficial lesions. J ultrasound 25: 783-797. https://doi.org/10.1007/s40477-021-00619-2
|
| [7] | Jogi SP, Sharma BB Retracted: methodology of iris image analysis for clinical diagnosis. (2014)2014: 235-240. https://doi.org/10.1109/MedCom.2014.7006010 |
| [8] | Atkin S (2013) Bilateral pitting oedema with multiple aetiologies. Aust J Herbal Med 25: 79-82. https://doi.org/10.3316/informit.481869825723186 |
| [9] | Jensen B (1982) Iridology: Science and Practice in the Healing Arts. Canada: Book Publishing Company. |
| [10] |
Gu R, Wang G, Song T, et al. (2020) CA-Net: comprehensive attention convolutional neural networks for explainable medical image segmentation. IEEE T Med Imaging 40: 699-711. https://doi.org/10.1109/TMI.2020.3035253
|
| [11] | Touvron H, Cord M, Douze M, et al. Training data-efficient image transformers & distillation through attention. (2021)139: 10347-10357. |
| [12] | Wang Y, Seo J, Jeon T (2021) NL-LinkNet: toward lighter but more accurate road extraction with nonlocal operations. IEEE Geosci Remote S 19: 1-5. https://doi.org/10.1109/LGRS.2021.3050477 |
| [13] | Chen Z, Zeng H, Yang W, et al. Texture enhancement method of oceanic internal waves in SAR images based on non-local mean filtering and multi-scale retinex. (2022)2022: 1-5. https://doi.org/10.1109/CISS57580.2022.9971169 |
| [14] | Agrawal S, Panda R, Mishro PK, et al. (2022) A novel joint histogram equalization-based image contrast enhancement. J King Saud Univ-Com 34: 1172-1182. https://doi.org/10.1016/j.jksuci.2019.05.010 |
| [15] |
Rao BS (2020) Dynamic histogram equalization for contrast enhancement for digital images. Appl Soft Comput 89: 106114. https://doi.org/10.1016/j.asoc.2020.106114
|
| [16] |
Doshvarpassand S, Wang X, Zhao X (2022) Sub-surface metal loss defect detection using cold thermography and dynamic reference reconstruction (DRR). Struct Health Monit 21: 354-369. https://doi.org/10.1177/1475921721999599
|
| [17] | Murugachandravel J, Anand S (2021) Enhancing MRI brain images using contourlet transform and adaptive histogram equalization. J Med Imag Health In 11: 3024-3027. https://doi.org/10.1166/jmihi.2021.3906 |
| [18] |
Radzi SFM, Karim MKA, Saripan MI, et al. (2020) Impact of image contrast enhancement on the stability of radiomics feature quantification on a 2D mammogram radiograph. IEEE Access 8: 127720-127731. https://doi.org/10.1109/ACCESS.2020.3008927
|
| [19] | Kuran U, Kuran EC (2021) Parameter selection for CLAHE using multi-objective cuckoo search algorithm for image contrast enhancement. Intell Syst Appl 12: 200051. https://doi.org/10.1016/j.iswa.2021.200051 |
| [20] |
Islam MR, Nahiduzzaman M (2022) Complex features extraction with deep learning model for the detection of COVID-19 from CT scan images using ensemble-based machine learning approach. Expert Syst Appl 195: 116554. https://doi.org/10.1016/j.eswa.2022.116554
|
| [21] |
Chen Y, Xia R, Yang K, et al. (2024) MICU: image super-resolution via multi-level information compensation and U-net. Expert Syst Appl 245: 123111. https://doi.org/10.1016/j.eswa.2023.123111
|
| [22] |
Chen Y, Xia R, Yang K, et al. (2024) DNNAM: image inpainting algorithm via deep neural networks and attention mechanism. Appl Soft Comput 154: 111392. https://doi.org/10.1016/j.asoc.2024.111392
|
| [23] |
Chen Y, Xia R, Yang K, et al. (2024) MFMAM: image inpainting via multi-scale feature module with attention module. Comput Vis Image Und 238: 103883. https://doi.org/10.1016/j.cviu.2023.103883
|
| [24] |
Naeem AB, Senapati B, Bhuva D, et al. (2024) Heart disease detection using feature extraction and artificial neural networks: a sensor-based approach. IEEE Access 12: 37349-37362. https://doi.org/10.1109/ACCESS.2024.3373646
|
| [25] |
Mira ES, Sapri AMS, Aljehanı RF, et al. (2024) Early diagnosis of oral cancer using image processing and artificial intelligence. Fusion: Pract Appl 14: 293-308. https://doi.org/10.54216/FPA.140122
|
| [26] |
Kumar K, Pradeepa M, Mahdal M, et al. (2023) A deep learning approach for kidney disease recognition and prediction through image processing. Appl Sci 13: 3621. https://doi.org/10.3390/app13063621
|
| [27] | Priyal MP, Ezhilarasan M IRIS segmentation technique using IRIS-UNet method. (2023)14124: 235. https://doi.org/10.1007/978-3-031-45382-3_20 |
| [28] | Yang Y, Jiang Z, Yang C, et al. Improved retinex image enhancement algorithm based on bilateral filtering. (2015)2015: 1363-1369. https://doi.org/10.2991/icmmcce-15.2015.427 |
| [29] |
Daugman J (2007) New methods in iris recognition. IEEE T Syst Man Cy B 37: 1167-1175. https://doi.org/10.1109/TSMCB.2007.903540
|



Figures(16) / Tables(4)

Poovayar Priya Mohan, Ezhilarasan Murugesan. A novel approach for detecting the presence of a lymphatic rosary in the iris using a 3-stage algorithm[J]. AIMS Bioengineering, 2024, 11(4): 506-526. doi: 10.3934/bioeng.2024023







 DownLoad:
DownLoad: