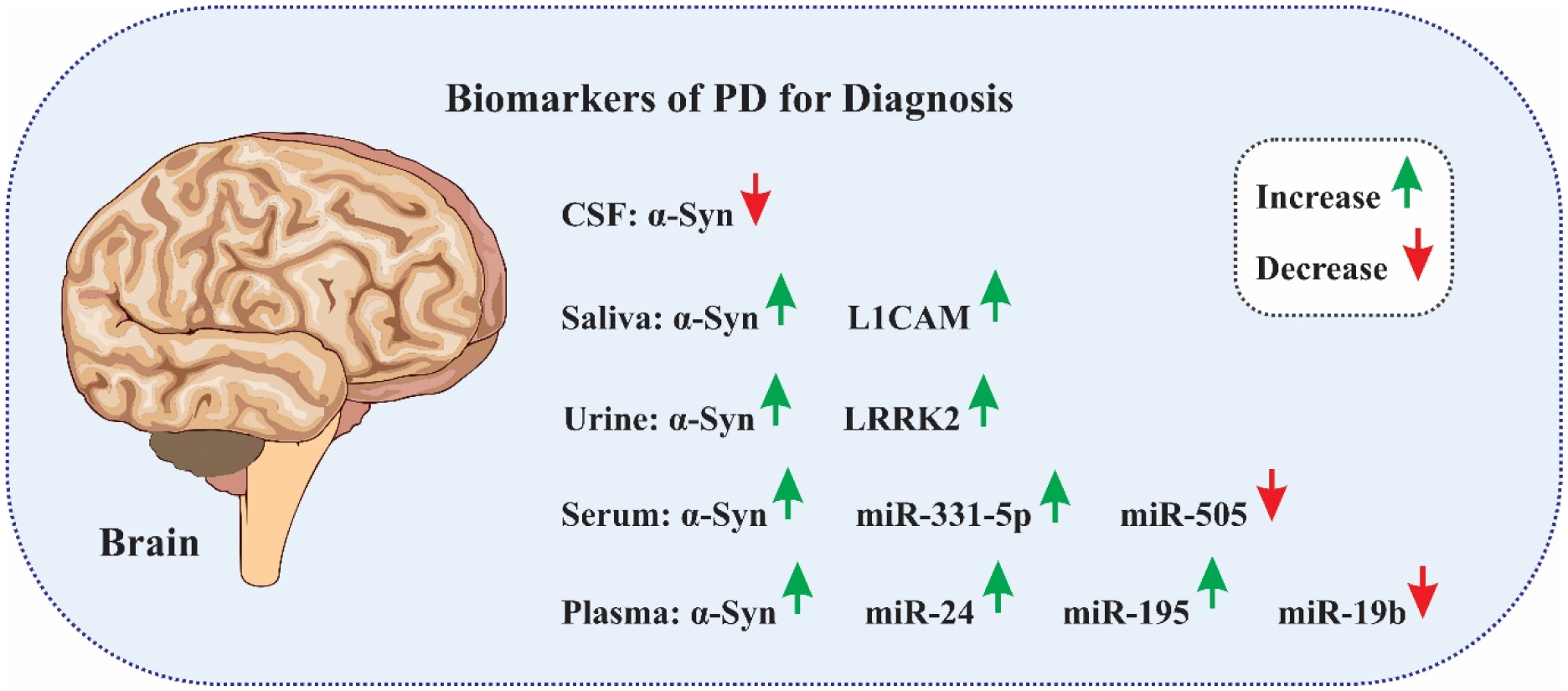
Parkinson's disease (PD) is characterized by the pathological accumulation of α-synuclein, which has driven extensive research into the role of exosomes in disease mechanisms. Exosomes are nanoscale vesicles enriched with proteins, RNA, and lipids that facilitate critical intercellular communication processes. Recent studies have elucidated the role of exosomes in transmitting misfolded proteins among neurons, which significantly impacts the progression of PD. The presence of disease-associated exosomes in cerebrospinal fluid and blood highlights their substantial diagnostic potential for PD. Specifically, exosomes derived from the central nervous system (CNS) have emerged as promising biomarkers because of their ability to accurately reflect pathological states. Furthermore, the isolation of exosomes from distinct brain cell types allows the identification of precise biomarkers, increasing diagnostic specificity and accuracy. In addition to being useful for diagnostics, exosomes hold therapeutic promise given their ability to cross the blood–brain barrier (BBB) and selectively modulate their cargo. These findings suggest that these materials could be used as delivery systems for therapeutic drugs for the treatment of neurodegenerative diseases. This review comprehensively examines the multifaceted roles of exosomes in PD pathogenesis, diagnosis, and treatment. It also addresses the associated clinical challenges and underscores the urgent need for further research and development to fully leverage exosome-based strategies in PD management.

Graphical abstract
Citation: Naeimeh Akbari-Gharalari, Maryam Ghahremani-Nasab, Roya Naderi, Leila Chodari, Farshad Nezhadshahmohammad. The potential of exosomal biomarkers: Revolutionizing Parkinson's disease: How do they influence pathogenesis, diagnosis, and therapeutic strategies?[J]. AIMS Neuroscience, 2024, 11(3): 374-397. doi: 10.3934/Neuroscience.2024023
Parkinson's disease (PD) is characterized by the pathological accumulation of α-synuclein, which has driven extensive research into the role of exosomes in disease mechanisms. Exosomes are nanoscale vesicles enriched with proteins, RNA, and lipids that facilitate critical intercellular communication processes. Recent studies have elucidated the role of exosomes in transmitting misfolded proteins among neurons, which significantly impacts the progression of PD. The presence of disease-associated exosomes in cerebrospinal fluid and blood highlights their substantial diagnostic potential for PD. Specifically, exosomes derived from the central nervous system (CNS) have emerged as promising biomarkers because of their ability to accurately reflect pathological states. Furthermore, the isolation of exosomes from distinct brain cell types allows the identification of precise biomarkers, increasing diagnostic specificity and accuracy. In addition to being useful for diagnostics, exosomes hold therapeutic promise given their ability to cross the blood–brain barrier (BBB) and selectively modulate their cargo. These findings suggest that these materials could be used as delivery systems for therapeutic drugs for the treatment of neurodegenerative diseases. This review comprehensively examines the multifaceted roles of exosomes in PD pathogenesis, diagnosis, and treatment. It also addresses the associated clinical challenges and underscores the urgent need for further research and development to fully leverage exosome-based strategies in PD management.
Graphical abstract
Alzheimer's disease
ALG2-interacting protein X
autophagy–lysosome pathway
amyotrophic lateral sclerosis
atypical parkinsonian syndrome
blood–brain barrier
corticobasal degeneration
central nervous system
cerebrospinal fluid
dementia with Lewy bodies
exosomal transfer into cells
frontotemporal dementia
glucocerebrosidase (GBA)
β-glucocerebrosidase
heat shock protein 70
heat shock protein 90
Huntington's disease
intercellular adhesion molecule 1
intraluminal vesicles
idiopathic PD
lymphocyte function-associated antigen 1
long noncoding RNAs
leucine-rich repeat kinase 2
L1 cell adhesion molecule
microtubule-associated protein
microtubule-associated protein tau gene
microRNAs
multiple sclerosis
multiple system atrophy
mesenchymal stem cell
multivesicular bodies
olivopontocerebellar atrophy
oxidized DJ-1
Parkinson's disease
PTEN-induced kinase 1
progressive supranuclear palsy
rapid eye movement sleep behavior disorder
RNA interference
Ser-1292-phosphorylated LRRK2
shRNA minicircles
small interfering RNAs
alpha-synuclein gene
striatonigral degeneration
tumor susceptibility gene 101
α-Synuclein

| [1] | Global, regional, and national burden of Parkinson's disease, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol (2018) 17: 939-953. |
| [2] | Movement Disorders: Volume 35, Number S1, September 2020. Mov Disord (2020) 35:. https://doi.org/10.1002/mds.28267 |
| [3] |
Ascherio A, Schwarzschild MA (2016) The epidemiology of Parkinson's disease: risk factors and prevention. Lancet Neurol 15: 1257-1272. https://doi.org/10.1016/S1474-4422(16)30230-7 
|
| [4] |
Kim CY, Alcalay RN (2017) Genetic Forms of Parkinson's Disease. Semin Neurol 37: 135-146. https://doi.org/10.1055/s-0037-1601567
|
| [5] |
Dauer W, Przedborski S (2003) Parkinson's disease: mechanisms and models. Neuron 39: 889-909. https://doi.org/10.1016/S0896-6273(03)00568-3
|
| [6] |
Braak H, Del Tredici K, Bratzke H, et al. (2002) Staging of the intracerebral inclusion body pathology associated with idiopathic Parkinson's disease (preclinical and clinical stages). J Neurol 249 Suppl 3: Iii/1-5. https://doi.org/10.1007/s00415-002-1301-4
|
| [7] |
Jankovic J (2008) Parkinson's disease: clinical features and diagnosis. J Neurol Neurosurg Psychiatry 79: 368-376. https://doi.org/10.1136/jnnp.2007.131045
|
| [8] |
Langston JW (2006) The parkinson's complex: Parkinsonism is just the tip of the iceberg. Ann Neurol 59: 591-596. https://doi.org/10.1002/ana.20834
|
| [9] |
Postuma RB, Berg D, Stern M, et al. (2015) MDS clinical diagnostic criteria for Parkinson's disease. Mov Disord 30: 1591-1601. https://doi.org/10.1002/mds.26424
|
| [10] |
Langston JW (1990) Predicting Parkinson's disease. Neurology 40: suppl 70-74; discussion 75–76.
|
| [11] |
Braak H, Del Tredici K, Rüb U, et al. (2003) Staging of brain pathology related to sporadic Parkinson's disease. Neurobiol Aging 24: 197-211. https://doi.org/10.1016/S0197-4580(02)00065-9
|
| [12] |
Bellingham S, Guo B, Coleman B, et al. (2012) Exosomes: Vehicles for the Transfer of Toxic Proteins Associated with Neurodegenerative Diseases?. Front Physiol 3. https://doi.org/10.3389/fphys.2012.00124
|
| [13] |
Guo M, Wang J, Zhao Y, et al. (2020) Microglial exosomes facilitate α-synuclein transmission in Parkinson's disease. Brain 143: 1476-1497. https://doi.org/10.1093/brain/awaa090
|
| [14] |
Yang T, Martin P, Fogarty B, et al. (2015) Exosome delivered anticancer drugs across the blood-brain barrier for brain cancer therapy in Danio rerio. Pharm Res 32: 2003-2014. https://doi.org/10.1007/s11095-014-1593-y
|
| [15] |
Goetzl EJ, Boxer A, Schwartz JB, et al. (2015) Altered lysosomal proteins in neural-derived plasma exosomes in preclinical Alzheimer disease. Neurology 85: 40-47. https://doi.org/10.1212/WNL.0000000000001702
|
| [16] |
Pardridge WM (2012) Drug transport across the blood–brain barrier. J Cerebr Blood F Met 32: 1959-1972. https://doi.org/10.1038/jcbfm.2012.126
|
| [17] |
Qu M, Lin Q, Huang L, et al. (2018) Dopamine-loaded blood exosomes targeted to brain for better treatment of Parkinson's disease. J Control Release 287: 156-166. https://doi.org/10.1016/j.jconrel.2018.08.035
|
| [18] |
Haney MJ, Klyachko NL, Zhao Y, et al. (2015) Exosomes as drug delivery vehicles for Parkinson's disease therapy. J Control Release 207: 18-30. https://doi.org/10.1016/j.jconrel.2015.03.033
|
| [19] |
Cooper JM, Wiklander PO, Nordin JZ, et al. (2014) Systemic exosomal siRNA delivery reduced alpha-synuclein aggregates in brains of transgenic mice. Mov Disord 29: 1476-1485. https://doi.org/10.1002/mds.25978
|
| [20] |
Guy R, Offen D (2020) Promising opportunities for treating neurodegenerative diseases with mesenchymal stem cell-derived exosomes. Biomolecules 10: 1320. https://doi.org/10.3390/biom10091320
|
| [21] |
Théry C, Zitvogel L, Amigorena S (2002) Exosomes: composition, biogenesis and function. Nat Rev Immunol 2: 569-579. https://doi.org/10.1038/nri855
|
| [22] |
Akbari-Gharalari N, Khodakarimi S, Nezhadshahmohammad F, et al. (2024) Exosomes in neuron-glia communication: A review on neurodegeneration. Bioimpacts 14: 30153-30153. https://doi.org/10.34172/bi.2023.30153
|
| [23] |
Kalluri R, LeBleu VS (2020) The biology, function, and biomedical applications of exosomes. Science 367. https://doi.org/10.1126/science.aau6977
|
| [24] | Omrani M, Beyrampour-Basmenj H, Jahanban-Esfahlan R, et al. (2023) Global trend in exosome isolation and application: an update concept in management of diseases. Mol Cell Biochem : 1-13. https://doi.org/10.1007/s11010-023-04756-6 |
| [25] |
Lachenal G, Pernet-Gallay K, Chivet M, et al. (2011) Release of exosomes from differentiated neurons and its regulation by synaptic glutamatergic activity. Mol Cell Neurosci 46: 409-418. https://doi.org/10.1016/j.mcn.2010.11.004
|
| [26] |
Wubbolts R, Leckie RS, Veenhuizen PT, et al. (2003) Proteomic and biochemical analyses of human B cell-derived exosomes. Potential implications for their function and multivesicular body formation. J Biol Chem 278: 10963-10972. https://doi.org/10.1074/jbc.M207550200
|
| [27] |
van Meer G, Voelker DR, Feigenson GW (2008) Membrane lipids: where they are and how they behave. Nat Rev Mol Cell Biol 9: 112-124. https://doi.org/10.1038/nrm2330
|
| [28] |
Zhang Y, Bi J, Huang J, et al. (2020) Exosome: A Review of Its Classification, Isolation Techniques, Storage, Diagnostic and Targeted Therapy Applications. Int J Nanomedicine 15: 6917-6934. https://doi.org/10.2147/IJN.S264498
|
| [29] |
Skokos D, Le Panse S, Villa I, et al. (2001) Mast cell-dependent B and T lymphocyte activation is mediated by the secretion of immunologically active exosomes. J Immunol 166: 868-876. https://doi.org/10.4049/jimmunol.166.2.868
|
| [30] |
Chen G, Huang AC, Zhang W, et al. (2018) Exosomal PD-L1 contributes to immunosuppression and is associated with anti-PD-1 response. Nature 560: 382-386. https://doi.org/10.1038/s41586-018-0392-8
|
| [31] |
Valadi H, Ekström K, Bossios A, et al. (2007) Exosome-mediated transfer of mRNAs and microRNAs is a novel mechanism of genetic exchange between cells. Nat Cell Biol 9: 654-659. https://doi.org/10.1038/ncb1596
|
| [32] |
Sharma A, Johnson A (2020) Exosome DNA: Critical regulator of tumor immunity and a diagnostic biomarker. J Cell Physiol 235: 1921-1932. https://doi.org/10.1002/jcp.29153
|
| [33] |
Harding CV, Heuser JE, Stahl PD (2013) Exosomes: looking back three decades and into the future. Cell Biol 200: 367-371. https://doi.org/10.1083/jcb.201212113
|
| [34] |
Pravin DP, Aashutosh US (2016) Molecular Biomarkers for Diagnosis & Therapies of Alzheimer's Disease. AIMS Neurosci 3: 433-453. https://doi.org/10.3934/Neuroscience.2016.4.433
|
| [35] |
Yakubovich E, Polischouk A, Evtushenko V (2022) Principles and problems of exosome isolation from biological fluids. Biochem Mosc Suppl S 16: 115-126. https://doi.org/10.1134/S1990747822030096
|
| [36] |
Kučuk N, Primožič M, Knez Ž, et al. (2021) Exosomes engineering and their roles as therapy delivery tools, therapeutic targets, and biomarkers. Int J Mol Sci 22: 9543. https://doi.org/10.3390/ijms22179543
|
| [37] |
Budnik V, Ruiz-Cañada C, Wendler F (2016) Extracellular vesicles round off communication in the nervous system. Nat Rev Neurosci 17: 160-172. https://doi.org/10.1038/nrn.2015.29
|
| [38] |
Desplats P, Lee HJ, Bae EJ, et al. (2009) Inclusion formation and neuronal cell death through neuron-to-neuron transmission of alpha-synuclein. Proc Natl Acad Sci U S A 106: 13010-13015. https://doi.org/10.1073/pnas.0903691106
|
| [39] |
Crews L, Spencer B, Desplats P, et al. (2010) Selective Molecular Alterations in the Autophagy Pathway in Patients with Lewy Body Disease and in Models of α-Synucleinopathy. PLOS ONE 5: e9313. https://doi.org/10.1371/journal.pone.0009313
|
| [40] |
Minakaki G, Menges S, Kittel A, et al. (2018) Autophagy inhibition promotes SNCA/alpha-synuclein release and transfer via extracellular vesicles with a hybrid autophagosome-exosome-like phenotype. Autophagy 14: 98-119. https://doi.org/10.1080/15548627.2017.1395992
|
| [41] |
Delenclos M, Trendafilova T, Mahesh D, et al. (2017) Investigation of Endocytic Pathways for the Internalization of Exosome-Associated Oligomeric Alpha-Synuclein. Front Neurosci 11. https://doi.org/10.3389/fnins.2017.00172
|
| [42] |
Huang Y, Liu Z, Li N, et al. (2022) Parkinson's Disease Derived Exosomes Aggravate Neuropathology in SNCA*A53T Mice. Ann Neurol 92: 230-245. https://doi.org/10.1002/ana.26421
|
| [43] |
Han C, Xiong N, Guo X, et al. (2019) Exosomes from patients with Parkinson's disease are pathological in mice. J Mol Med (Berl) 97: 1329-1344. https://doi.org/10.1007/s00109-019-01810-z
|
| [44] | Sano K, Atarashi R, Satoh K, et al. (2018) Prion-Like Seeding of Misfolded α-Synuclein in the Brains of Dementia with Lewy Body Patients in RT-QUIC. Mol Neurobiol 55: 3916-3930. https://doi.org/10.1007/s12035-017-0624-1 |
| [45] |
Danzer KM, Kranich LR, Ruf WP, et al. (2012) Exosomal cell-to-cell transmission of alpha synuclein oligomers. Mol Neurodegener 7: 42. https://doi.org/10.1186/1750-1326-7-42
|
| [46] |
Stuendl A, Kunadt M, Kruse N, et al. (2016) Induction of α-synuclein aggregate formation by CSF exosomes from patients with Parkinson's disease and dementia with Lewy bodies. Brain 139: 481-494. https://doi.org/10.1093/brain/awv346
|
| [47] |
Herman S, Djaldetti R, Mollenhauer B, et al. (2022) CSF-derived extracellular vesicles from patients with Parkinson's disease induce symptoms and pathology. Brain 146: 209-224. https://doi.org/10.1093/brain/awac261
|
| [48] | Yakabi K, Berson E, Montine KS, et al. (2023) Human cerebrospinal fluid single exosomes in Parkinson's and Alzheimer's diseases. bioRxiv : 2023.2012.2022.573124. https://doi.org/10.1101/2023.12.22.573124 |
| [49] |
Shi M, Liu C, Cook TJ, et al. (2014) Plasma exosomal α-synuclein is likely CNS-derived and increased in Parkinson's disease. Acta Neuropathol 128: 639-650. https://doi.org/10.1101/2023.12.22.573124
|
| [50] |
Kenwrick S, Watkins A, Angelis ED (2000) Neural cell recognition molecule L1: relating biological complexity to human disease mutations. Hum Mol Genet 9: 879-886. https://doi.org/10.1093/hmg/9.6.879
|
| [51] |
Niu M, Li Y, Li G, et al. (2020) A longitudinal study on α-synuclein in plasma neuronal exosomes as a biomarker for Parkinson's disease development and progression. Eur J Neurol 27: 967-974. https://doi.org/10.1111/ene.14208
|
| [52] |
Yan YQ, Pu JL, Zheng R, et al. (2022) Different patterns of exosomal α-synuclein between Parkinson's disease and probable rapid eye movement sleep behavior disorder. Eur J Neurol 29: 3590-3599. https://doi.org/10.1111/ene.15537
|
| [53] |
Postuma RB, Gagnon JF, Bertrand JA, et al. (2015) Parkinson risk in idiopathic REM sleep behavior disorder: preparing for neuroprotective trials. Neurology 84: 1104-1113. https://doi.org/10.1212/WNL.0000000000001364
|
| [54] | Shim KH, Go HG, Bae H, et al. (2021) Decreased Exosomal Acetylcholinesterase Activity in the Plasma of Patients With Parkinson's Disease. Front Aging Neurosci 13. https://doi.org/10.3389/fnagi.2021.665400 |
| [55] |
Si X, Tian J, Chen Y, et al. (2019) Central Nervous System-Derived Exosomal Alpha-Synuclein in Serum May Be a Biomarker in Parkinson's Disease. Neuroscience 413: 308-316. https://doi.org/10.1016/j.neuroscience.2019.05.015
|
| [56] | Kluge A, Bunk J, Schaeffer E, et al. (2022) Correction to: Detection of neuron-derived pathological α-synuclein in blood. Brain 146: e6-e6. https://doi.org/10.1093/brain/awac370 |
| [57] |
Zheng H, Xie Z, Zhang X, et al. (2021) Investigation of α-Synuclein Species in Plasma Exosomes and the Oligomeric and Phosphorylated α-Synuclein as Potential Peripheral Biomarker of Parkinson's Disease. Neuroscience 469: 79-90. https://doi.org/10.1016/j.neuroscience.2021.06.033
|
| [58] |
Zhentang C, Yufeng W, Genliang L, et al. (2019) α-Synuclein in salivary extracellular vesicles as a potential biomarker of Parkinson's disease. Neurosci Lett 696: 114-120. https://doi.org/10.1016/j.neulet.2018.12.030
|
| [59] |
Rani K, Mukherjee R, Singh E, et al. (2019) Neuronal exosomes in saliva of Parkinson's disease patients: A pilot study. Parkinsonism Relat D 67: 21-23. https://doi.org/10.1016/j.parkreldis.2019.09.008
|
| [60] |
Kang W, Chen W, Yang Q, et al. (2016) Salivary total α-synuclein, oligomeric α-synuclein and SNCA variants in Parkinson's disease patients. Sci Rep 6: 28143. https://doi.org/10.1038/srep28143
|
| [61] |
Shu H, Zhang P, Gu L (2024) Alpha-synuclein in peripheral body fluid as a biomarker for Parkinson's disease. Acta Neurol Belg 124: 831-842. https://doi.org/10.1007/s13760-023-02452-2
|
| [62] |
Clements CM, McNally RS, Conti BJ, et al. (2006) DJ-1, a cancer- and Parkinson's disease-associated protein, stabilizes the antioxidant transcriptional master regulator Nrf2. Proc Natl Acad Sci U S A 103: 15091-15096. https://doi.org/10.1073/pnas.0607260103
|
| [63] | Jang J, Jeong S, Lee SI, et al. (2018) Oxidized DJ-1 levels in urine samples as a putative biomarker for Parkinson's disease. Parkinsons Dis 2018. https://doi.org/10.1155/2018/1241757 |
| [64] |
An C, Pu X, Xiao W, et al. (2018) Expression of the DJ-1 protein in the serum of Chinese patients with Parkinson's disease. Neurosci Lett 665: 236-239. https://doi.org/10.1016/j.neulet.2017.12.023
|
| [65] |
Waragai M, Nakai M, Wei J, et al. (2007) Plasma levels of DJ-1 as a possible marker for progression of sporadic Parkinson's disease. Neurosci Lett 425: 18-22. https://doi.org/10.1016/j.neulet.2007.08.010
|
| [66] |
T. dos Santos MC, Scheller D, Schulte C, et al. (2018) Evaluation of cerebrospinal fluid proteins as potential biomarkers for early stage Parkinson's disease diagnosis. PLOS ONE 13: e0206536. https://doi.org/10.1371/journal.pone.0206536
|
| [67] |
Zhao Z-H, Chen Z-T, Zhou R-L, et al. (2019) Increased DJ-1 and α-synuclein in plasma neural-derived exosomes as potential markers for Parkinson's disease. Front Aging Neurosci 10: 438. https://doi.org/10.3389/fnagi.2018.00438
|
| [68] |
Gonzales PA, Pisitkun T, Hoffert JD, et al. (2009) Large-Scale Proteomics and Phosphoproteomics of Urinary Exosomes. J Am Soc Nephrol 20: 363-379. https://doi.org/10.1681/ASN.2008040406
|
| [69] |
Pisitkun T, Shen R-F, Knepper MA (2004) Identification and proteomic profiling of exosomes in human urine. P Natl Acad Sci 101: 13368-13373. https://doi.org/10.1073/pnas.0403453101
|
| [70] | Ho DH, Yi S, Seo H, et al. (2014) Increased DJ-1 in urine exosome of Korean males with Parkinson's disease. Biomed Res Int 2014: 704678. https://doi.org/10.1155/2014/704678 |
| [71] |
Goedert M, Spillantini MG (2006) A century of Alzheimer's disease. Science 314: 777-781. https://doi.org/10.1126/science.1132814
|
| [72] |
Spillantini MG, Goedert M (2013) Tau pathology and neurodegeneration. Lancet Neurol 12: 609-622. https://doi.org/10.1016/S1474-4422(13)70090-5
|
| [73] |
Wills J, Jones J, Haggerty T, et al. (2010) Elevated tauopathy and alpha-synuclein pathology in postmortem Parkinson's disease brains with and without dementia. Exp Neurol 225: 210-218. https://doi.org/10.1016/j.expneurol.2010.06.017
|
| [74] |
Edwards TL, Scott WK, Almonte C, et al. (2010) Genome-wide association study confirms SNPs in SNCA and the MAPT region as common risk factors for Parkinson disease. Ann Hum Genet 74: 97-109. https://doi.org/10.1111/j.1469-1809.2009.00560.x
|
| [75] |
Simón-Sánchez J, Schulte C, Bras JM, et al. (2009) Genome-wide association study reveals genetic risk underlying Parkinson's disease. Nat Genet 41: 1308-1312. https://doi.org/10.1038/ng.487
|
| [76] |
Vermilyea SC, Christensen A, Meints J, et al. (2022) Loss of tau expression attenuates neurodegeneration associated with α-synucleinopathy. Transl Neurodegener 11: 34. https://doi.org/10.1186/s40035-022-00309-x
|
| [77] |
Shi M, Kovac A, Korff A, et al. (2016) CNS tau efflux via exosomes is likely increased in Parkinson's disease but not in Alzheimer's disease. Alzheimers Dement 12: 1125-1131. https://doi.org/10.1016/j.jalz.2016.04.003
|
| [78] |
Berg D, Schweitzer KJ, Leitner P, et al. (2005) Type and frequency of mutations in the LRRK2 gene in familial and sporadic Parkinson's disease*. Brain 128: 3000-3011. https://doi.org/10.1093/brain/awh666
|
| [79] |
Paisán-Ruíz C, Jain S, Evans EW, et al. (2004) Cloning of the gene containing mutations that cause PARK8-linked Parkinson's disease. Neuron 44: 595-600. https://doi.org/10.1016/j.neuron.2004.10.023
|
| [80] | Rosenbusch KE, Kortholt A (2016) Activation Mechanism of LRRK2 and Its Cellular Functions in Parkinson's Disease. Parkinsons Dis 2016: 7351985. https://doi.org/10.1155/2016/7351985 |
| [81] |
Fraser KB, Moehle MS, Daher JP, et al. (2013) LRRK2 secretion in exosomes is regulated by 14-3-3. Hum Mol Genet 22: 4988-5000. https://doi.org/10.1093/hmg/ddt346
|
| [82] |
Fraser KB, Moehle MS, Alcalay RN, et al. (2016) Urinary LRRK2 phosphorylation predicts parkinsonian phenotypes in G2019S LRRK2 carriers. Neurology 86: 994-999. https://doi.org/10.1212/WNL.0000000000002436
|
| [83] |
Di Maio R, Hoffman EK, Rocha EM, et al. (2018) LRRK2 activation in idiopathic Parkinson's disease. Sci Transl Med 10. https://doi.org/10.1126/scitranslmed.aar5429
|
| [84] |
Fraser KB, Rawlins AB, Clark RG, et al. (2016) Ser(P)-1292 LRRK2 in urinary exosomes is elevated in idiopathic Parkinson's disease. Mov Disord 31: 1543-1550. https://doi.org/10.1002/mds.26686
|
| [85] |
Wang H (2021) MicroRNAs, Parkinson's Disease, and Diabetes Mellitus. Int J Mol Sci 22: 2953. https://doi.org/10.3390/ijms22062953
|
| [86] |
Gui Y, Liu H, Zhang L, et al. (2015) Altered microRNA profiles in cerebrospinal fluid exosome in Parkinson disease and Alzheimer disease. Oncotarget 6: 37043-37053. https://doi.org/10.18632/oncotarget.6158
|
| [87] |
Nie C, Sun Y, Zhen H, et al. (2020) Differential Expression of Plasma Exo-miRNA in Neurodegenerative Diseases by Next-Generation Sequencing. Front Neurosci 14: 438. https://doi.org/10.3389/fnins.2020.00438
|
| [88] | Yao YF, Qu MW, Li GC, et al. (2018) Circulating exosomal miRNAs as diagnostic biomarkers in Parkinson's disease. Eur Rev Med Pharmacol Sci 22: 5278-5283. |
| [89] |
Margis R, Margis R, Rieder CR (2011) Identification of blood microRNAs associated to Parkinsonĭs disease. J Biotechnol 152: 96-101. https://doi.org/10.1016/j.jbiotec.2011.01.023
|
| [90] |
Botta-Orfila T, Morató X, Compta Y, et al. (2014) Identification of blood serum micro-RNAs associated with idiopathic and LRRK2 Parkinson's disease. J Neurosci Res 92: 1071-1077. https://doi.org/10.1002/jnr.23377
|
| [91] |
Vallelunga A, Ragusa M, Di Mauro S, et al. (2014) Identification of circulating microRNAs for the differential diagnosis of Parkinson's disease and Multiple System Atrophy. Front Cell Neurosci 8. https://doi.org/10.3389/fncel.2014.00156
|
| [92] |
Cao XY, Lu JM, Zhao ZQ, et al. (2017) MicroRNA biomarkers of Parkinson's disease in serum exosome-like microvesicles. Neurosci Lett 644: 94-99. https://doi.org/10.1016/j.neulet.2017.02.045
|
| [93] |
Qian X, Zhao J, Yeung PY, et al. (2019) Revealing lncRNA Structures and Interactions by Sequencing-Based Approaches. Trends Biochem Sci 44: 33-52. https://doi.org/10.1016/j.tibs.2018.09.012
|
| [94] |
Wu P, Zuo X, Deng H, et al. (2013) Roles of long noncoding RNAs in brain development, functional diversification and neurodegenerative diseases. Brain Res Bull 97: 69-80. https://doi.org/10.1016/j.brainresbull.2013.06.001
|
| [95] |
Zou J, Guo Y, Wei L, et al. (2020) Long Noncoding RNA POU3F3 and α-Synuclein in Plasma L1CAM Exosomes Combined with β-Glucocerebrosidase Activity: Potential Predictors of Parkinson's Disease. Neurotherapeutics 17: 1104-1119. https://doi.org/10.1007/s13311-020-00842-5
|
| [96] | Boer DEC, van Smeden J, Bouwstra JA, et al. (2020) Glucocerebrosidase: Functions in and Beyond the Lysosome. J Clin Med 9. https://doi.org/10.3390/jcm9030736 |
| [97] |
Fanciulli A, Wenning GK (2015) Multiple-system atrophy. N Engl J Med 372: 249-263. https://doi.org/10.1056/NEJMra1311488
|
| [98] |
Gilman S, Wenning GK, Low PA, et al. (2008) Second consensus statement on the diagnosis of multiple system atrophy. Neurology 71: 670-676. https://doi.org/10.1212/01.wnl.0000324625.00404.15
|
| [99] |
Fanciulli A, Stankovic I, Krismer F, et al. (2019) Multiple system atrophy. Int Rev Neurobiol 149: 137-192. https://doi.org/10.1016/bs.irn.2019.10.004
|
| [100] |
Galvin JE, Lee VM, Trojanowski JQ (2001) Synucleinopathies: clinical and pathological implications. Arch Neurol 58: 186-190. https://doi.org/10.1001/archneur.58.2.186
|
| [101] |
Wenning GK, Ben-Shlomo Y, Hughes A, et al. (2000) What clinical features are most useful to distinguish definite multiple system atrophy from Parkinson's disease?. J Neurol Neurosurg Psychiatry 68: 434-440. https://doi.org/10.1136/jnnp.68.4.434
|
| [102] |
Jiang C, Hopfner F, Katsikoudi A, et al. (2020) Serum neuronal exosomes predict and differentiate Parkinson's disease from atypical parkinsonism. J Neurol Neurosurg Psychiatry 91: 720-729. https://doi.org/10.1136/jnnp-2019-322588
|
| [103] |
Dutta S, Hornung S, Kruayatidee A, et al. (2021) α-Synuclein in blood exosomes immunoprecipitated using neuronal and oligodendroglial markers distinguishes Parkinson's disease from multiple system atrophy. Acta Neuropathol 142: 495-511. https://doi.org/10.1007/s00401-021-02324-0
|
| [104] |
Höglinger GU, Respondek G, Stamelou M, et al. (2017) Clinical diagnosis of progressive supranuclear palsy: The movement disorder society criteria. Mov Disord 32: 853-864. https://doi.org/10.1002/mds.26987
|
| [105] |
Manna I, Quattrone A, De Benedittis S, et al. (2021) Exosomal miRNA as peripheral biomarkers in Parkinson's disease and progressive supranuclear palsy: A pilot study. Parkinsonism Relat Disord 93: 77-84. https://doi.org/10.1016/j.parkreldis.2021.11.020
|
| [106] |
McKeith IG, Dickson DW, Lowe J, et al. (2005) Diagnosis and management of dementia with Lewy bodies: third report of the DLB Consortium. Neurology 65: 1863-1872. https://doi.org/10.1212/01.wnl.0000187889.17253.b1
|
| [107] | Lippa CF, Duda JE, Grossman M, et al. (2007) DLB and PDD boundary issues. Diagnosis Treatment Molecular Pathology Biomarkers 68: 812-819. https://doi.org/10.1212/01.wnl.0000256715.13907.d3 |
| [108] |
Bonanni L, Thomas A, Onofrj M (2006) Diagnosis and management of dementia with Lewy bodies: third report of the DLB Consortium. Neurology 66: 1455; author reply 1455. https://doi.org/10.1212/01.wnl.0000224698.67660.45
|
| [109] |
Emre M, Aarsland D, Brown R, et al. (2007) Clinical diagnostic criteria for dementia associated with Parkinson's disease. Mov Disord 22: 1689-1707; quiz 1837. https://doi.org/10.1002/mds.21507
|
| [110] |
Walker Z, Possin KL, Boeve BF, et al. (2015) Lewy body dementias. Lancet 386: 1683-1697. https://doi.org/10.1016/S0140-6736(15)00462-6
|
| [111] |
Swallow DMA, Counsell CE (2023) The evolution of diagnosis from symptom onset to death in progressive supranuclear palsy (PSP) and corticobasal degeneration (CBD) compared to Parkinson's disease (PD). J Neurol 270: 3464-3474. https://doi.org/10.1007/s00415-023-11629-x
|
| [112] |
Meloni M, Agliardi C, Guerini FR, et al. (2023) Oligomeric α-synuclein and tau aggregates in NDEVs differentiate Parkinson's disease from atypical parkinsonisms. Neurobiol Dis 176: 105947. https://doi.org/10.1016/j.nbd.2022.105947
|
| [113] |
Jiang C, Hopfner F, Berg D, et al. (2021) Validation of α-Synuclein in L1CAM-Immunocaptured Exosomes as a Biomarker for the Stratification of Parkinsonian Syndromes. Mov Disord 36: 2663-2669. https://doi.org/10.1002/mds.28591
|
| [114] |
Müller T (2012) Drug therapy in patients with Parkinson's disease. Translational Neurodegener 1: 1-13. https://doi.org/10.1186/2047-9158-1-10
|
| [115] |
Zhuang X, Xiang X, Grizzle W, et al. (2011) Treatment of brain inflammatory diseases by delivering exosome encapsulated anti-inflammatory drugs from the nasal region to the brain. Mol Ther 19: 1769-1779. https://doi.org/10.1038/mt.2011.164
|
| [116] | Lai CP-K, Breakefield XO (2012) Role of exosomes/microvesicles in the nervous system and use in emerging therapies. Front Physiol 3: 228. https://doi.org/10.3389/fphys.2012.00228 |
| [117] |
Akbari-Gharalari N, Ghahremani-Nasab M, Naderi R, et al. (2023) Improvement of spinal cord injury symptoms by targeting the Bax/Bcl2 pathway and modulating TNF-α/IL-10 using Platelet-Rich Plasma exosomes loaded with dexamethasone. AIMS Neurosci 10: 332-353. https://doi.org/10.3934/Neuroscience.2023026
|
| [118] |
Kojima R, Bojar D, Rizzi G, et al. (2018) Designer exosomes produced by implanted cells intracerebrally deliver therapeutic cargo for Parkinson's disease treatment. Nat Commun 9: 1305. https://doi.org/10.1038/s41467-018-03733-8
|
| [119] |
Izco M, Blesa J, Schleef M, et al. (2019) Systemic exosomal delivery of shRNA minicircles prevents parkinsonian pathology. Mol Ther 27: 2111-2122. https://doi.org/10.1016/j.ymthe.2019.08.010
|
| [120] |
Mianehsaz E, Mirzaei HR, Mahjoubin-Tehran M, et al. (2019) Mesenchymal stem cell-derived exosomes: a new therapeutic approach to osteoarthritis?. Stem Cell Res Ther 10: 1-13. https://doi.org/10.1186/s13287-019-1445-0
|
| [121] |
Li Z, Liu F, He X, et al. (2019) Exosomes derived from mesenchymal stem cells attenuate inflammation and demyelination of the central nervous system in EAE rats by regulating the polarization of microglia. Int Immunopharmacol 67: 268-280. https://doi.org/10.1016/j.intimp.2018.12.001
|
| [122] |
Vilaça-Faria H, Salgado AJ, Teixeira FG (2019) Mesenchymal stem cells-derived exosomes: a new possible therapeutic strategy for Parkinson's disease?. Cells 8: 118. https://doi.org/10.3390/cells8020118
|
| [123] |
Heris RM, Shirvaliloo M, Abbaspour-Aghdam S, et al. (2022) The potential use of mesenchymal stem cells and their exosomes in Parkinson's disease treatment. Stem Cell Res Ther 13: 371. https://doi.org/10.1186/s13287-022-03050-4
|
| [124] |
Abrishamdar M, Jalali MS, Yazdanfar N (2023) The role of exosomes in pathogenesis and the therapeutic efficacy of mesenchymal stem cell-derived exosomes against Parkinson's disease. Neurol Sci 44: 2277-2289. https://doi.org/10.1007/s10072-023-06706-y
|
| [125] |
Kattaia A, Abd EL-Baset S, Abdul-Maksoud R, et al. (2022) The therapeutic potential of exosomes derived from mesenchymal stem cells in experimentally induced hypertensive encephalopathy. J Med Histol 6: 16-33. https://doi.org/10.21608/jmh.2022.145535.1100
|
| [126] |
Tomlinson PR, Zheng Y, Fischer R, et al. (2015) Identification of distinct circulating exosomes in Parkinson's disease. Ann Clin Transl Neur 2: 353-361. https://doi.org/10.1002/acn3.175
|
| [127] |
Sarko DK, McKinney CE (2017) Exosomes: origins and therapeutic potential for neurodegenerative disease. Front Neurosci 11: 82. https://doi.org/10.3389/fnins.2017.00082
|
Figures(2) / Tables(1)

Naeimeh Akbari-Gharalari, Maryam Ghahremani-Nasab, Roya Naderi, Leila Chodari, Farshad Nezhadshahmohammad. The potential of exosomal biomarkers: Revolutionizing Parkinson's disease: How do they influence pathogenesis, diagnosis, and therapeutic strategies?[J]. AIMS Neuroscience, 2024, 11(3): 374-397. doi: 10.3934/Neuroscience.2024023







 DownLoad:
DownLoad: