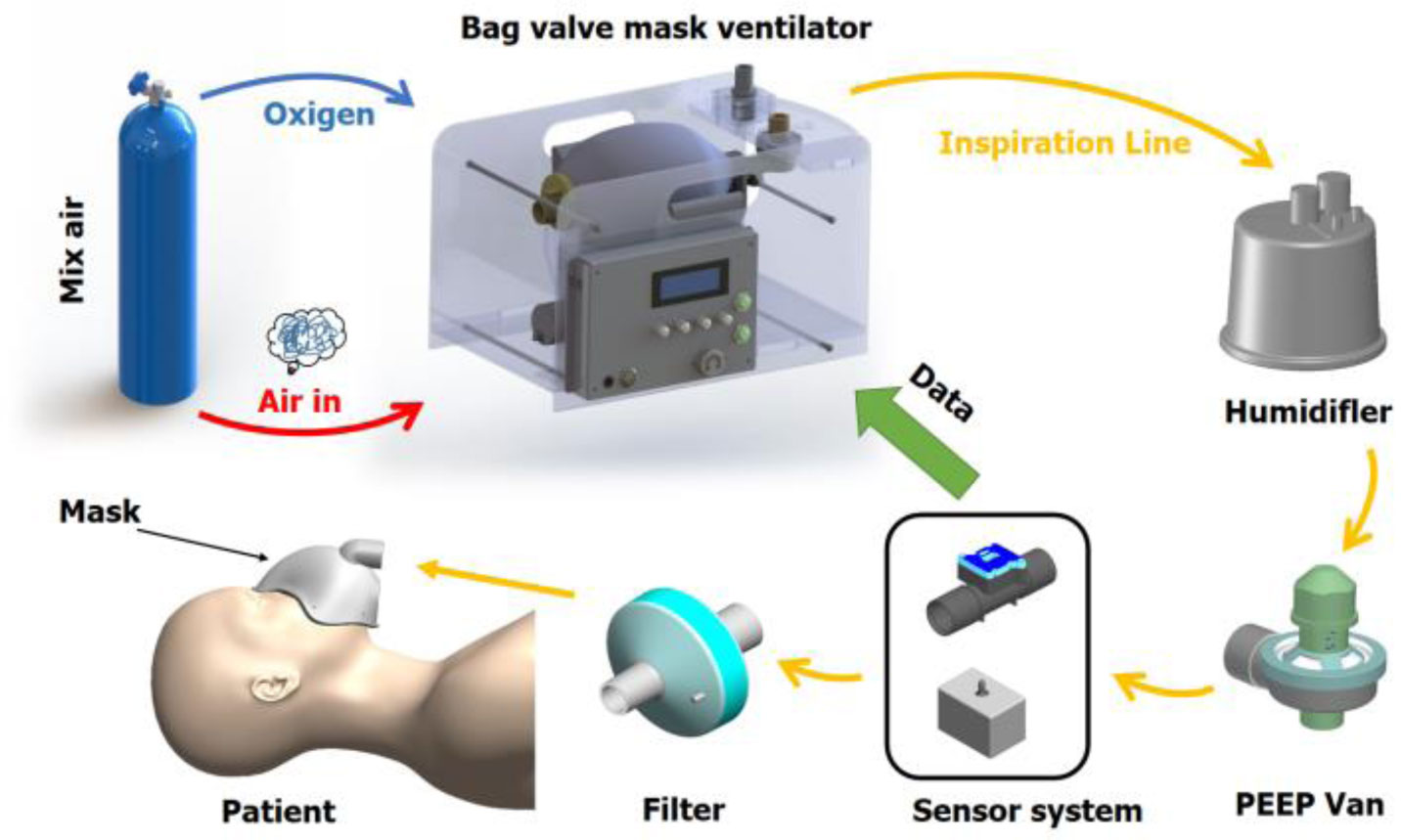
Ventilators are drawn to many researchers during the Covid-19 pandemic because it's essential equipment that's accustomed to treat severe Covid-19 patients. In low-income countries, there's a shortage of pricy respiratory devices resulting in exceeding the provision of taking care of Covid-19's patients in ICU. This paper attempts to design and implement an appropriate respiratory device referred to as a bag valve mask (BVM) ventilator for those who are Covid-19 patients in medical care, those patients have a requirement of safe transport and also palliative care. The BVM ventilator comprises a man-made manual breath unit (AMBU) bag and paddles for squeezing the AMBU bag which is popular in medical aid settings. The BVM ventilator is required to travel airflow through the system to the patient's lung with the specified volume for every breath cycle within a threshold air pressure. Since the AMBU bag is straightforward to be deformed over time, it's difficult to get mathematical modelling for constructing a reliable controller. Therefore, a model-free control (MFC) control approach is utilized successfully to style a controller for our BVM ventilator model with a PEEP valve and a HEPA filter. Some experimental scenarios are administered to gauge the effectiveness of the proposed controller for the BVM ventilator to control the airflow and control air pressure mode.
Citation: Cong Toai Truong, Kim Hieu Huynh, Van Tu Duong, Huy Hung Nguyen, Le An Pham, Tan Tien Nguyen. Model-free volume and pressure cycled control of automatic bag valve mask ventilator[J]. AIMS Bioengineering, 2021, 8(3): 192-207. doi: 10.3934/bioeng.2021017
Ventilators are drawn to many researchers during the Covid-19 pandemic because it's essential equipment that's accustomed to treat severe Covid-19 patients. In low-income countries, there's a shortage of pricy respiratory devices resulting in exceeding the provision of taking care of Covid-19's patients in ICU. This paper attempts to design and implement an appropriate respiratory device referred to as a bag valve mask (BVM) ventilator for those who are Covid-19 patients in medical care, those patients have a requirement of safe transport and also palliative care. The BVM ventilator comprises a man-made manual breath unit (AMBU) bag and paddles for squeezing the AMBU bag which is popular in medical aid settings. The BVM ventilator is required to travel airflow through the system to the patient's lung with the specified volume for every breath cycle within a threshold air pressure. Since the AMBU bag is straightforward to be deformed over time, it's difficult to get mathematical modelling for constructing a reliable controller. Therefore, a model-free control (MFC) control approach is utilized successfully to style a controller for our BVM ventilator model with a PEEP valve and a HEPA filter. Some experimental scenarios are administered to gauge the effectiveness of the proposed controller for the BVM ventilator to control the airflow and control air pressure mode.

| [1] |
Harapan H, Itoh N, Yufika A, et al. (2020) Coronavirus disease 2019 (COVID-19): A literature review. J Infect Public Health 13: 667-673. doi: 10.1016/j.jiph.2020.03.019

|
| [2] |
Jiang F, Deng L, Zhang L, et al. (2020) Review of the clinical characteristics of Coronavirus Disease 2019 (COVID-19). J Gen Intern Med 35: 1545-1549. doi: 10.1007/s11606-020-05762-w
|
| [3] |
Shi Y, Wang G, Cai X, et al. (2020) An overview of COVID-19. J Zhejiang Univ Sci B 21: 343-360. doi: 10.1631/jzus.B2000083
|
| [4] | Kumar D, Malviya R, Sharma PK (2020) Corona virus: a review of COVID-19. EJMO 4: 8-25. |
| [5] |
Khan N, Naushad M Effects of Corona Virus on the World Community (2020) . doi: 10.2139/ssrn
|
| [6] |
Hua J, Shaw R (2020) Corona virus (Covid-19) “infodemic” and emerging issues through a data lens: The case of China. Int J Environ Res Public Health 17: 2309. doi: 10.3390/ijerph17072309
|
| [7] |
Area I, Nieto JJ Forecasting the effects of the new SARS-CoV-2 variant in Europe (2021) . doi: 10.1155/2021/5553240
|
| [8] |
Bindayna KM, Crinion S (2021) Variant analysis of SARS-CoV-2 genomes in the Middle East. Microb Pathog 153: 104741. doi: 10.1016/j.micpath.2021.104741
|
| [9] | WHO Coronavirus (COVID-19) Dashboard, 2021 Available from: https://covid19.who.int/. |
| [10] | Wiwanitkit V (2021) Atypical modes of COVID-19 transmission: how likely are they? Epidemiol Health 42: e2020059. |
| [11] |
Moghadas SM, Fitzpatrick MC, Sah P, et al. (2020) The implications of silent transmission for the control of COVID-19 outbreaks. Proc Natl Acad Sci U S A 117: 17513-17515. doi: 10.1073/pnas.2008373117
|
| [12] | Hersh E Coronavirus Incubation Period: How Long Before Symptoms Appear? (2020) .Available from: https://www.healthline.com/health/coronavirus-incubation-period. |
| [13] | Galiatsatos P Johns Hopkins Bayview Medical Center, COVID-19 Lung Damage (2021) .Available from: https://www.hopkinsmedicine.org/health/conditions-and-diseases/coronavirus/what-coronavirus-does-to-the-lungs. |
| [14] |
Bhaskar S, Sinha A, Banach M, et al. (2020) Cytokine storm in COVID-19—immunopathological mechanisms, clinical considerations, and therapeutic approaches: the REPROGRAM consortium position paper. Front Immunol 11: 1648. doi: 10.3389/fimmu.2020.01648
|
| [15] |
Flato UAP, Ferreira KV, Biteli P, et al. (2021) Rabdomyolysis as a serious complication of COVID-19. AIMS Bioengineering 8: 165-172. doi: 10.3934/bioeng.2021015
|
| [16] |
Novaes Matias J, Sorrentino dos Santos Campanari G, Achete de Souza G, et al. (2020) Metabolic syndrome and COVID-19. AIMS Bioengineering 7: 242-253. doi: 10.3934/bioeng.2020021
|
| [17] |
Maclaren G, Fisher D, Brodie D (2020) Preparing for the most critically Ill patients with COVID-19: the potential role of extracorporeal membrane oxygenation. JAMA 323: 1245-1246. doi: 10.1001/jama.2020.2342
|
| [18] |
Ramanathan K, Antognini D, Combes A, et al. (2020) Planning and provision of ECMO services for severe ARDS during the COVID-19 pandemic and other outbreaks of emerging infectious diseases. Lancet Respir Med 8: 518-526. doi: 10.1016/S2213-2600(20)30121-1
|
| [19] | Engla LN (2020) Journal-2010-New engla nd journal. N Engl J Med 38: 1969-1973. |
| [20] |
Russel J, Slustsky A, Lemaire F (1999) International consensus conferences in intensive care medicine: Ventilator-associated lung injury in ARDS. Am J Respir Crit Care Med 160: 2118-2124. doi: 10.1164/ajrccm.160.6.ats16060
|
| [21] | Lagasse J COVID-19: Ventilators are in short supply, but so are medications for ventilator patients | Healthcare Finance News, 2020 Available from: https://www.healthcarefinancenews.com/news/covid-19-ventilators-are-short-supply-so-are-medications-ventilator-patients. |
| [22] |
Ranney ML, Griffeth V, Jha AK (2020) Critical supply shortages—the need for ventilators and personal protective equipment during the Covid-19 pandemic. N Engl J Med 382: e41. doi: 10.1056/NEJMp2006141
|
| [23] |
Gereffi G (2020) What does the COVID-19 pandemic teach us about global value chains? The case of medical supplies. J Int Bus Policy 3: 287-301. doi: 10.1057/s42214-020-00062-w
|
| [24] | Ouyang H The New York Times Magazine, I'm an E.R. Doctor in New York. None of Us Will Ever Be the Same, 2020 Available from: https://www.nytimes.com/2020/04/14/magazine/coronavirus-er-doctor-diary-new-york-city.html. |
| [25] |
Lapostolle F, Goix L, Vianu I, et al. (2020) COVID-19 epidemic in the Seine-Saint-Denis Department of Greater Paris: One month and three waves for a tsunami. Eur J Emerg Med 27: 274-278. doi: 10.1097/MEJ.0000000000000723
|
| [26] |
Warren J, Fromm RE, Orr RA, et al. (2004) Guidelines for the inter- and intrahospital transport of critically ill patients. Crit Care Med 32: 256-262. doi: 10.1097/01.CCM.0000104917.39204.0A
|
| [27] |
Gebremichael M, Borg U, Habashi NM, et al. (2000) Interhospital transport of the extremely ill patient: The mobile intensive care unit. Crit Care Med 28: 79-85. doi: 10.1097/00003246-200001000-00013
|
| [28] |
Blakeman TC, Branson RD (2013) Inter-and intra-hospital transport of the critically IllDiscussion. Respir Care 58: 1008-1023. doi: 10.4187/respcare.02404
|
| [29] |
Corey RM, Widloski EM, Null D, et al. (2020) Low-complexity system and algorithm for an emergency ventilator sensor and alarm. IEEE Trans Biomed Circuits Syst 14: 1088-1096. doi: 10.1109/TBCAS.2020.3020702
|
| [30] | Chauhan R, Chaudari V, Gaddamwar AS, et al. (2020) Mathematical Modelling of an automatic bag mask valve emergency ventilator. Int Res J Eng Technol 7: 1679-1685. |
| [31] | Agency M& HR, Products, Medicines & Healthcare Regulatory Agency, Rapidly Manufactured Ventilator System, 2020 Available from: https://www.gov.uk/government/publications/specification-for-ventilators-to-be-used-in-uk-hospitals-during-the-coronavirus-covid-19-outbreak. |
| [32] |
Petsiuk A, Tanikella NG, Dertinger S, et al. (2020) Partially RepRapable automated open source bag valve mask-based ventilator. HardwareX 8: e00131. doi: 10.1016/j.ohx.2020.e00131
|
| [33] |
Chauhan R, Sharma R, Chauhan N (2020) Automatic AMBU bag operating device: creating a boon for high-volume centres in low-income countries. BMJ Innov 6: 255-258. doi: 10.1136/bmjinnov-2019-000406
|
| [34] |
Dafilou B, Schwester D, Ruhl N, et al. (2020) It's in the bag: Tidal volumes in adult and pediatric bag valve masks. West J Emerg Med 21: 722-726. doi: 10.5811/westjem.2020.3.45788
|
| [35] | Hewing L, Menner M, Tachatos N, et al. (2020) Volume control of low-cost ventilator with automatic set-point adaptation arXiv: 2009.01530. |
| [36] |
Jibril M, Tadese M, Hassen N Design and performance investigation of a low cost portable ventilator for COVID-19 patients (2020) . doi: 10.20944/preprints202008.0059.v1
|
| [37] |
Husseini AM Al, Lee HJ, Negrete J, et al. (2010) Design and prototyping of a low-cost portable mechanical ventilator. J Med Device 4: 027514. doi: 10.1115/1.3442790
|
| [38] | Bocklage T, Carter JB, Balk RA Setting the Tidal Volume In Adults Receiving Mechanical Ventilation: Lessons Learned From Recent Invesitgations, 2015 Available from: https://www.nbrc.org/wp-content/uploads/2017/07/Setting-the-Tidal-Volume.pdf. |
| [39] |
Mercat A, Richard J-CM, Vielle B, et al. (2008) Positive end-expiratory pressure setting in adults with acute lung injury and acute respiratory distress syndrome: a randomized controlled trial. J Am Med Assoc 299: 646-655. doi: 10.1001/jama.299.6.646
|
| [40] |
Bime C, Fiero M, Lu Z, et al. (2017) High positive end-expiratory pressure is associated with improved survival in obese patients with acute respiratory distress syndrome. Am J Med 130: 207-213. doi: 10.1016/j.amjmed.2016.09.029
|
| [41] |
Rodriguez P, Dojat M, Brochard L (2005) Mechanical ventilation: changing concepts. Indian J Crit Care Med 9: 235-243. doi: 10.4103/0972-5229.19765
|
| [42] | Chourpiliadis C, Bhardwaj A StatPearls, Physiology, Respiratory Rate, 2019 Available from: http://www.ncbi.nlm.nih.gov/pubmed/30725991. |
| [43] |
Boros SJ (1979) Variations in inspiratory: expiratory ratio and airway pressure wave form during mechanical ventilation: The significance of mean airway pressure. J Pediatr 94: 114-117. doi: 10.1016/S0022-3476(79)80372-8
|
| [44] |
Fernandez R, Mendez M, Younes M (1999) Effect of ventilator flow rate on respiratory timing in normal humans. Am J Respir Crit Care Med 159: 710-719. doi: 10.1164/ajrccm.159.3.9709090
|
| [45] | Chatburn RL (2013) Classification of mechanical ventilators and modes of ventilation. Principles and Practice of Mechanical Ventilation Chicago: McGraw Hill Professional, 45-64. |
| [46] |
Arnal JM (2018) Monitoring Mechanical Ventilation using Ventilator Waveforms Berlin: Springer. doi: 10.1007/978-3-319-58655-7
|
| [47] |
Khoury A, Hugonnot S, Cossus J, et al. (2014) From mouth-to-mouth to bag-valve-mask ventilation: Evolution and characteristics of actual devices—a review of the literature. Biomed Res Int 2014: 762053. doi: 10.1155/2014/762053
|
| [48] |
Fliess M, Join C (2013) Model-free control. Int J Control 86: 2228-2252. doi: 10.1080/00207179.2013.810345
|
| [49] |
Fliess M, Sira-Ramírez H (2003) An algebraic framework for linear identification. ESAIM: Control Optim Calc Var 9: 151-168. doi: 10.1051/cocv:2003008
|
| [50] |
Fliess M, Sira-Ramírez H (2008) Closed-loop parametric identification for continuous-time linear systems via new algebraic techniques. Identification of Continuous-time Models from Sampled Data London: Springer, 363-391. doi: 10.1007/978-1-84800-161-9_13
|






Figures(7) / Tables(2)

Cong Toai Truong, Kim Hieu Huynh, Van Tu Duong, Huy Hung Nguyen, Le An Pham, Tan Tien Nguyen. Model-free volume and pressure cycled control of automatic bag valve mask ventilator[J]. AIMS Bioengineering, 2021, 8(3): 192-207. doi: 10.3934/bioeng.2021017







 DownLoad:
DownLoad: