The outbreak of the COVID-19 pandemic has affected the safety and well-being of healthcare workers. A scoping review was conducted to highlight the impact of COVID-19 on the safety, health, and well-being of healthcare workers and to shed light on the concerns about their perceived safety and support systems. A literature search was conducted in three different databases from December 1, 2019, through July 20, 2022, to find publications that meet the aim of this review. Using search engines, 3087 articles were identified, and after a rigorous assessment by two reviewers, 30 articles were chosen for further analysis. Two themes emerged during the analysis: safety and health and well-being. The primary safety concern of the staff was mostly about contracting COVID-19, infecting family members, and caring for patients with COVID-19. During the pandemic, the health care workers appeared to have anxiety, stress, uncertainty, burnout, and a lack of sleep. Additionally, the review focused on the suggestions of health care providers to improve the safety and well-being of workers through fair organizational policies and practices and timely, individualized mental health care.
Citation: Abdulqadir J. Nashwan, Rejo G. Mathew, Reni Anil, Nabeel F. Allobaney, Sindhumole Krishnan Nair, Ahmed S. Mohamed, Ahmad A. Abujaber, Abbas Balouchi, Evangelos C. Fradelos. The safety, health, and well-being of healthcare workers during COVID-19: A scoping review[J]. AIMS Public Health, 2023, 10(3): 593-609. doi: 10.3934/publichealth.2023042
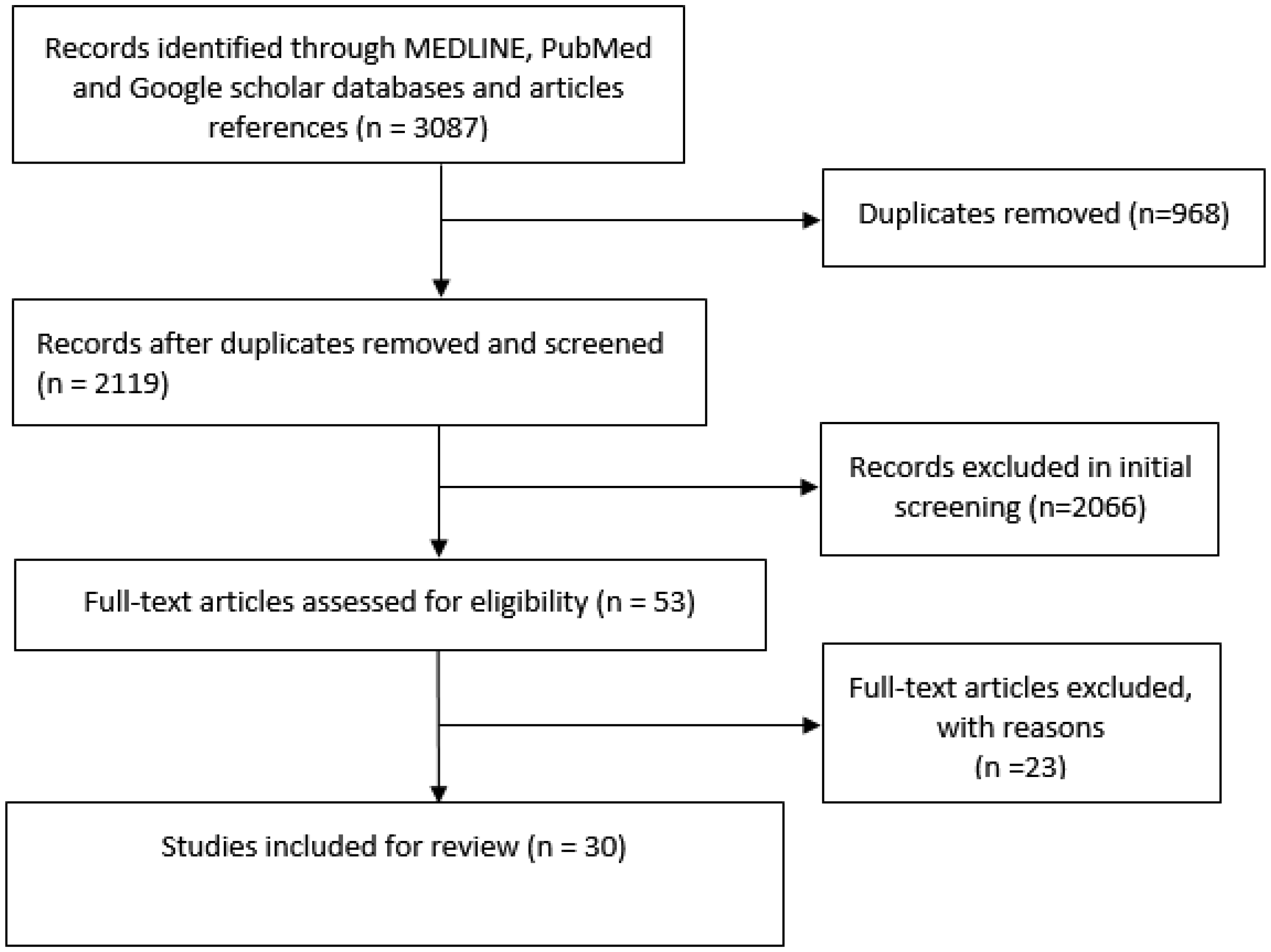
The outbreak of the COVID-19 pandemic has affected the safety and well-being of healthcare workers. A scoping review was conducted to highlight the impact of COVID-19 on the safety, health, and well-being of healthcare workers and to shed light on the concerns about their perceived safety and support systems. A literature search was conducted in three different databases from December 1, 2019, through July 20, 2022, to find publications that meet the aim of this review. Using search engines, 3087 articles were identified, and after a rigorous assessment by two reviewers, 30 articles were chosen for further analysis. Two themes emerged during the analysis: safety and health and well-being. The primary safety concern of the staff was mostly about contracting COVID-19, infecting family members, and caring for patients with COVID-19. During the pandemic, the health care workers appeared to have anxiety, stress, uncertainty, burnout, and a lack of sleep. Additionally, the review focused on the suggestions of health care providers to improve the safety and well-being of workers through fair organizational policies and practices and timely, individualized mental health care.

| [1] |
Jacob L, Smith L, Butler L, et al. (2020) COVID-19 social distancing and sexual activity in a sample of the British Public. J Sex Med 17: 1229-1236. https://doi.org/10.1016/j.jsxm.2020.05.001 
|
| [2] | Gostin L O (2022) Life after the COVID-19 Pandemic. in JAMA Health Forum. J Am Med Inform Assn 3: e220323-e220323. https://doi.org/10.1001/jamahealthforum.2022.0323 |
| [3] | McDiarmid M, Condon M, Gaitens J (2021) The healthcare sector employer's duty of care: Implications for worker well-being. Int J Environ Res 18: 6015. https://doi.org/10.3390/ijerph18116015 |
| [4] | Centers for Disease Control and Prevention (U.S.) COVID data tracker. Available from: https://stacks.cdc.gov/view/cdc/115269 |
| [5] | World Health OrganizationThe impact of COVID-19 on health and care workers: a closer look at deaths (2021). Available from: https://apps.who.int/iris/bitstream/handle/10665/345300/WHO-HWF-WorkingPaper-2021.1-eng.pdf?sequence=1&isAllowed=y. |
| [6] | World Health OrganizationWHO calls for healthy, safe and decent working conditions for all health workers, amidst COVID-19 pandemic (2020). Available from: https://www.who.int/news/item/28-04-2020-who-calls-for-healthy-safe-and-decent-working-conditions-for-all-health-workers-amidst-covid-19-pandemic. |
| [7] |
Nissan D, Weiss G, Siman-Tov M, et al. (2021) Differences in levels of psychological distress, perceived safety, trust, and efficacy amongst hospital personnel during the COVID-19 pandemic. Res Nurs Health 44: 776-786. https://doi.org/10.1002/nur.22165
|
| [8] |
Pereira M A, Camanho A S, Marques R C, et al. (2021) The convergence of the world health organization member states regarding the United Nations' sustainable development goal ‘good health and well-being’. Omega 104: 102495. https://doi.org/10.1016/j.omega.2021.102495
|
| [9] |
Munn Z, Peters MDJ, Stern C, et al. (2018) Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med Res Methodol 18: 1-7. https://doi.org/10.1186/s12874-018-0611-x
|
| [10] |
Galanis P, Vraka I, Fragkou D, et al. (2021) Nurses' burnout and associated risk factors during the COVID-19 pandemic: A systematic review and meta-analysis. J Adv Nurs 77: 3286-3302. https://doi.org/10.1111/jan.14839
|
| [11] |
Kader N, Elhusein B, Chandrappa NSK, et al. (2021) Perceived stress and post-traumatic stress disorder symptoms among intensive care unit staff caring for severely ill coronavirus disease 2019 patients during the pandemic: a national study. Ann Gen Psychiatry 20: 1-8. https://doi.org/10.1186/s12991-021-00363-1
|
| [12] |
Peters MD, Godfrey CM, Khalil H, et al. (2015) Guidance for conducting systematic scoping reviews. Int J Evid Based Healthc 13: 141-146. https://doi.org/10.1097/XEB.0000000000000050
|
| [13] |
Khalil H, Peters M, Godfrey CM, et al. (2016) An evidence-based approach to scoping reviews. Worldviews Evid Based Nurs 13: 118-123. https://doi.org/10.1111/wvn.12144
|
| [14] |
Peters MDJ, Marnie C, Tricco AC, et al. (2020) Updated methodological guidance for the conduct of scoping reviews. JBI Evid Synth 18: 2119-2126. https://doi.org/10.11124/JBIES-20-00167
|
| [15] | Aromataris E, Munn Z (2020) JBI manual for evidence synthesis. Australia Joanna Briggs Institute . Available from: https://synthesismanual.jbi.global. |
| [16] |
Munn Z, Pollock D, Khalil H, et al. (2022) What are scoping reviews? Providing a formal definition of scoping reviews as a type of evidence synthesis. JBI evidence synthesis 20: 950-952. https://doi.org/10.11124/JBIES-21-00483
|
| [17] |
Moher D, Liberati A, Tetzlaff J, et al. (2009) Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann Intern Med 151: 264-269. https://doi.org/10.7326/0003-4819-151-4-200908180-00135
|
| [18] |
Tricco AC, Lillie E, Zarin W, et al. (2018) PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and explanation. Ann Intern Med 169: 467-473. https://doi.org/10.7326/M18-0850
|
| [19] |
McGowan J, Straus S, Moher D, et al. (2020) Reporting scoping reviews—PRISMA ScR extension. J Clin Epidemiol 123: 177-179. https://doi.org/10.1016/j.jclinepi.2020.03.016
|
| [20] |
Holton S, Wynter K, Trueman M, et al. (2021) Immediate impact of the COVID-19 pandemic on the work and personal lives of Australian hospital clinical staff. Aust Health Rev 45: 656-666. https://doi.org/10.1071/AH21014
|
| [21] |
Koontalay A, Suksatan W, Prabsangob K, et al. (2021) Healthcare workers' burdens during the COVID-19 pandemic: A qualitative systematic review. J Multidiscip Healthc 14: 3015-3025. https://doi.org/10.2147/JMDH.S330041
|
| [22] |
Biber J, Ranes B, Lawrence S, et al. (2022) Mental health impact on healthcare workers due to the COVID-19 pandemic: A US cross-sectional survey study. J Patient Rep Outcomes 6: 1-14. https://doi.org/10.1186/s41687-022-00467-6
|
| [23] |
Muller AE, Hafstad EV, Himmels JPW, et al. (2020) The mental health impact of the covid-19 pandemic on healthcare workers, and interventions to help them: A rapid systematic review. Psychiatry Res 293: 113441. https://doi.org/10.1016/j.psychres.2020.113441
|
| [24] |
Kader N, Elhusein B, Al Abdulla S, et al. (2021) Risk perception and psychological impact of COVID-19 pandemic among healthcare workers in primary and secondary healthcare settings in Qatar: A national study. J Prim Care Community Health 12: 21501327211039714. https://doi.org/10.1177/21501327211039714
|
| [25] |
Nashwan AJ, Valdez GFD, Al-Fayyadh S, et al. (2022) Stigma towards health care providers taking care of COVID-19 patients: A multi-country study. Heliyon 8: e09300. https://doi.org/10.1016/j.heliyon.2022.e09300
|
| [26] |
Villar RC, Nashwan AJ, Mathew RG, et al. (2021) The lived experiences of frontline nurses during the coronavirus disease 2019 (COVID-19) pandemic in Qatar: A qualitative study. Nurs Open 8: 3516-3526. https://doi.org/10.1002/nop2.901
|
| [27] |
Nashwan AJ, Al-Fayyadh S, Al-Hadrawi H, et al. (2021) Development and initial validation of stigma towards healthcare providers working with COVID-19 patients scale (S19-HCPs). J Multidiscip Healthc 14: 3125-3134. https://doi.org/10.2147/JMDH.S321498
|
| [28] |
Nashwan A J, Korkmaz M, Avci I A (2022) Stigma against health care providers caring for COVID-19 patients in Turkey. Cogent Public Health 9: 2110191. https://doi.org/10.1080/27707571.2022.2110191
|
| [29] |
Nashwan AJ, Abujaber AA, Mohamed AS, et al. (2021) Nurses' willingness to work with COVID-19 patients: the role of knowledge and attitude. Nurs Open 8: 695-701. https://doi.org/10.1002/nop2.674
|
| [30] |
Chandler-Jeanville S, Nohra RG, Loizeau V, et al. (2021) Perceptions and experiences of the COVID-19 pandemic amongst frontline nurses and their relatives in France in six paradoxes: a qualitative study. Int J Environ Res Public Health 18: 6977. https://doi.org/10.3390/ijerph18136977
|
| [31] |
Mercado M, Wachter K, Schuster RC, et al. (2022) A cross-sectional analysis of factors associated with stress, burnout and turnover intention among healthcare workers during the COVID-19 pandemic in the United States. Health Soc Care Community 30: e2690-e2701. https://doi.org/10.1111/hsc.13712
|
| [32] |
Nashwan AJ, Abujaber AA, Villar RC, et al. (2021) Comparing the impact of COVID-19 on nurses' turnover intentions before and during the pandemic in Qatar. J Pers Med 11: 456. https://doi.org/10.3390/jpm11060456
|
| [33] |
Allobaney N F, Nashwan A J, Mohamed A S (2020) Nursing Research during COVID-19 Pandemic: A Scoping Review. Open J Nurs 10: 952-959. https://doi.org/10.4236/ojn.2020.1010066
|
| [34] |
Alnaeem MM, Hamdan-Mansour AM, Nashwan AJ, et al. (2022) Healthcare providers' intention to leave their jobs during COVID-19 pandemic: A cross-sectional study. Health Sci Rep 5: e859. https://doi.org/10.1002/hsr2.859
|
| [35] |
Vizheh M, Qorbani M, Arzaghi SM, et al. (2020) The mental health of healthcare workers in the COVID-19 pandemic: A systematic review. J Diabetes Metab Disord 19: 1967-1978. https://doi.org/10.1007/s40200-020-00643-9
|
| [36] |
Wozniak H, Benzakour L, Moullec G, et al. (2021) Mental health outcomes of ICU and non-ICU healthcare workers during the COVID-19 outbreak: a cross-sectional study. Ann Intensive Care 11: 1-10. https://doi.org/10.1186/s13613-021-00900-x
|
| [37] |
Pappa S, Ntella V, Giannakas T, et al. (2020) Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav Immun 88: 901-907. https://doi.org/10.1016/j.bbi.2020.05.026
|
| [38] |
Nashwan AJ, Villar RC, Al-Qudimat AR, et al. (2021) Quality of life, sleep quality, depression, anxiety, stress, eating habits, and social bounds in nurses during the coronavirus disease 2019 pandemic in Qatar (The PROTECTOR Study): A cross-sectional, comparative study. J Pers Med 11: 918. https://doi.org/10.3390/jpm11090918
|
| [39] | Azam F, Latif MF, Bashir S, et al. (2022) Impact of COVID-19 pandemic on psychological wellbeing of Oncology clinicians in the Middle East and North Africa (MENA) region. Eur Rev Med Pharmacol Sci 26: 1049-1055. |
| [40] |
Bhattacharya P K, Prakash J (2021) Impact of COVID-19 on psychological and emotional well-being of healthcare workers. Indian J Crit Care Med 25: 479. https://doi.org/10.5005/jp-journals-10071-23833
|
| [41] |
Jagiasi BG, Chanchalani G, Nasa P, et al. (2021) Impact of COVID-19 pandemic on the emotional well-being of healthcare workers: a multinational cross-sectional survey. Indian J Crit Care Med 25: 499-506. https://doi.org/10.5005/jp-journals-10071-23806
|
| [42] |
El Gindi H, Shalaby R, Gusnowski A, et al. (2022) The mental health impact of the COVID-19 pandemic among physicians, nurses, and other health care providers in Alberta: Cross-sectional survey. JMIR Form Res 6: e27469. https://doi.org/10.2196/27469
|
| [43] |
Haidari E, Main EK, Cui X, et al. (2021) Maternal and neonatal health care worker well-being and patient safety climate amid the COVID-19 pandemic. J Perinatol 41: 961-969. https://doi.org/10.1038/s41372-021-01014-9
|
| [44] |
Tran J, Willis K, Kay M, et al. (2022) The workplace and psychosocial experiences of Australian senior doctors during the COVID-19 pandemic: A qualitative study. Int J Environ Res Public Health 19: 3079. https://doi.org/10.3390/ijerph19053079
|
| [45] |
Daradkeh LF, Villar RC, Nashwan AJ (2021) The perception of nursing leaders towards communication and relationship management competencies while using digital platforms during COVID-19 pandemic in Qatar : A cross-sectional study. J Nurs Manag 30: 2707-2714. https://doi.org/10.1111/jonm.13722
|
| [46] |
Salgado de Snyder VN, Villatoro AP, McDaniel MD, et al. (2021) Occupational stress and mental health among healthcare workers serving socially vulnerable populations during the COVID-19 pandemic. Front Public Health 9: 782846. https://doi.org/10.3389/fpubh.2021.782846
|
| [47] |
Thatrimontrichai A, Weber DJ, Apisarnthanarak A (2021) Mental health among healthcare personnel during COVID-19 in Asia: A systematic review. J Formos Med Assoc 120: 1296-1304. https://doi.org/10.1016/j.jfma.2021.01.023
|
| [48] |
Ripp J, Peccoralo L, Charney D (2020) Attending to the emotional well-being of the health care workforce in a New York City health system during the COVID-19 pandemic. Acad Med 95: 1136-1139. https://doi.org/10.1097/ACM.0000000000003414
|
| [49] |
Pilar A, Gravel SB, Croke J, et al. (2021) Coronavirus Disease 2019's (COVID-19's) silver lining—Through the eyes of radiation oncology fellows. Adv Radiat Oncol 6: 100527. https://doi.org/10.1016/j.adro.2020.07.004
|
| [50] |
Squellati R, Zangaro GA (2022) Eight ways nurses can manage a burnt-out leader. Nurs Clin North Am 57: 67-78. https://doi.org/10.1016/j.cnur.2021.11.005
|
| [51] |
Carvalho S, Coelho CG, Kluwe-Schiavon B, et al. (2022) The acute impact of the early stages of COVID-19 pandemic in people with pre-existing psychiatric disorders: A systematic review. Int J Environ Res Public Health 19: 5140. https://doi.org/10.3390/ijerph19095140
|
| [52] |
Odachi R, Takahashi S, Sugawara D, et al. (2022) The Big Five personality traits and the fear of COVID-19 in predicting depression and anxiety among Japanese nurses caring for COVID-19 patients: A cross-sectional study in Wakayama prefecture. Plos One 17: e0276803. https://doi.org/10.1371/journal.pone.0276803
|
Figures(1) / Tables(2)

Abdulqadir J. Nashwan, Rejo G. Mathew, Reni Anil, Nabeel F. Allobaney, Sindhumole Krishnan Nair, Ahmed S. Mohamed, Ahmad A. Abujaber, Abbas Balouchi, Evangelos C. Fradelos. The safety, health, and well-being of healthcare workers during COVID-19: A scoping review[J]. AIMS Public Health, 2023, 10(3): 593-609. doi: 10.3934/publichealth.2023042







 DownLoad:
DownLoad: