This study evaluates the impact of different combinations of treatment regimens, such as additional radiation, chemotherapy, and surgical treatments, on the survival of elderly rectal cancer patients ≥ 70 years of age to support physicians' clinical decision-making.
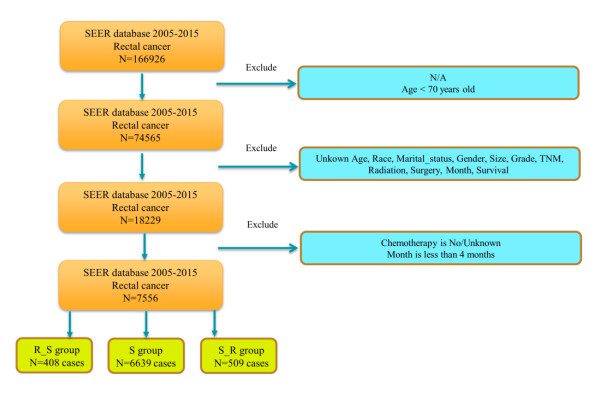
Data from a sample of elderly rectal cancer patients aged ≥ 70 years diagnosed from 2005–2015 from the US surveillance, epidemiology, and end results (SEER) database were retrospectively analyzed. The best cut-off point was selected using the x-tile software for the three continuity indices: age, tumor size, and number of regional lymph nodes. All patients were categorized into either the neoadjuvant radiotherapy and surgery group (R_S group), the surgical treatment group (S group), or the surgery and adjuvant radiotherapy group (S_R group). The propensity score allocation was used to match each included study subject in a 1:1 ratio, and the restricted mean survival time method (RMST) was used to predict the mean survival of rectal cancer patients within 5 and 10 years. The prognostic risk factors for rectal cancer patients were determined using univariate and multivariate Cox regression analyses, and nomograms were constructed. A subgroup stratification analysis of patients with different treatment combination regimens was performed using the Kaplan-Meier method, and log-rank tests were used for between-group comparisons. The model's predictive accuracy was assessed by receiver operating characteristic (ROC) curves, correction curves, and a clinical decision curve analysis (DCA).
A total of 7556 cases of sample data from 2005 to 2015 were included, which were categorized into 6639 patients (87.86%) in the S group, 408 patients (5.4%) in the R_S group, and 509 patients (6.74%) in the S_R group, according to the relevant order of radiotherapy and surgery. After propensity score matching (PSM), the primary clinical characteristics of the groups were balanced and comparable. The difference in the mean survival time before and after PSM was not statistically significant in both R_S and S groups (P value > 0.05), and the difference in the mean survival time after PSM was statistically substantial in S_R and S groups (P value < 0.05). In the multifactorial Cox analysis, the M1 stage and Nodes ≥ 9 were independent risk factors. An age between 70–75 was an independent protective factor for patients with rectal cancer in the R_S and S groups. The Marital_status, T4 stage, N2 stage, M1 stage, and Nodes ≥ 9 were independent risk factors for patients with rectal cancer in the S_R and S groups, and an age between 70–81 was an independent protective factor. The ROC curve area, the model C index, and the survival calibration curve suggested good agreement between the actual and predicted values of the model. The DCA for 3-year, 5-year, and 10-year survival periods indicated that the model had some potential for application.
The results of the study showed no significant difference in the overall survival (OS) between elderly patients who received neoadjuvant radiotherapy and surgery and those who received surgery alone; elderly patients who received surgery and adjuvant radiotherapy had some survival benefits compared with those who received surgery alone, though the benefit of adjuvant radiotherapy was not significant. Therefore, radiotherapy for rectal cancer patients older than 70 years old should be based on individual differences in condition, and a precise treatment plan should be developed.
Citation: Wei Wang, Tongping Shen, Jiaming Wang. Analysis of the impact of radiotherapy and surgical treatment regimens based on the SEER database on the survival outcomes of rectal cancer patients over 70 years[J]. Mathematical Biosciences and Engineering, 2024, 21(3): 4463-4484. doi: 10.3934/mbe.2024197
This study evaluates the impact of different combinations of treatment regimens, such as additional radiation, chemotherapy, and surgical treatments, on the survival of elderly rectal cancer patients ≥ 70 years of age to support physicians' clinical decision-making.
Data from a sample of elderly rectal cancer patients aged ≥ 70 years diagnosed from 2005–2015 from the US surveillance, epidemiology, and end results (SEER) database were retrospectively analyzed. The best cut-off point was selected using the x-tile software for the three continuity indices: age, tumor size, and number of regional lymph nodes. All patients were categorized into either the neoadjuvant radiotherapy and surgery group (R_S group), the surgical treatment group (S group), or the surgery and adjuvant radiotherapy group (S_R group). The propensity score allocation was used to match each included study subject in a 1:1 ratio, and the restricted mean survival time method (RMST) was used to predict the mean survival of rectal cancer patients within 5 and 10 years. The prognostic risk factors for rectal cancer patients were determined using univariate and multivariate Cox regression analyses, and nomograms were constructed. A subgroup stratification analysis of patients with different treatment combination regimens was performed using the Kaplan-Meier method, and log-rank tests were used for between-group comparisons. The model's predictive accuracy was assessed by receiver operating characteristic (ROC) curves, correction curves, and a clinical decision curve analysis (DCA).
A total of 7556 cases of sample data from 2005 to 2015 were included, which were categorized into 6639 patients (87.86%) in the S group, 408 patients (5.4%) in the R_S group, and 509 patients (6.74%) in the S_R group, according to the relevant order of radiotherapy and surgery. After propensity score matching (PSM), the primary clinical characteristics of the groups were balanced and comparable. The difference in the mean survival time before and after PSM was not statistically significant in both R_S and S groups (P value > 0.05), and the difference in the mean survival time after PSM was statistically substantial in S_R and S groups (P value < 0.05). In the multifactorial Cox analysis, the M1 stage and Nodes ≥ 9 were independent risk factors. An age between 70–75 was an independent protective factor for patients with rectal cancer in the R_S and S groups. The Marital_status, T4 stage, N2 stage, M1 stage, and Nodes ≥ 9 were independent risk factors for patients with rectal cancer in the S_R and S groups, and an age between 70–81 was an independent protective factor. The ROC curve area, the model C index, and the survival calibration curve suggested good agreement between the actual and predicted values of the model. The DCA for 3-year, 5-year, and 10-year survival periods indicated that the model had some potential for application.
The results of the study showed no significant difference in the overall survival (OS) between elderly patients who received neoadjuvant radiotherapy and surgery and those who received surgery alone; elderly patients who received surgery and adjuvant radiotherapy had some survival benefits compared with those who received surgery alone, though the benefit of adjuvant radiotherapy was not significant. Therefore, radiotherapy for rectal cancer patients older than 70 years old should be based on individual differences in condition, and a precise treatment plan should be developed.

| [1] |
L. S. Rebecca, D. M. Kimberly, E. F. Hannah, A. Jemal, Cancer statistics, 2021, CA Cancer J. Clin., 1 (2021), 7–33. https://doi.org/10.3322/caac.21654 doi: 10.3322/caac.21654

|
| [2] |
C. E. Bailey, C. Y. Hu, Y. N. You, Increasing disparities in the age-related incidences of colon and rectal cancers in the United States, 1975–2010, JAMA Surg., 150 (2015), 17–22. https://doi.org/10.1001/jamasurg.2014.1756 doi: 10.1001/jamasurg.2014.1756
|
| [3] |
R. A. Audisio, D. Papamichael, Treatment of colorectal cancer in older patients, Nat. Rev. Gastroenterol. Hepatol., 9 (2012), 716–725. https://doi.org/10.1038/nrgastro.2012.196 doi: 10.1038/nrgastro.2012.196
|
| [4] |
S. Pilleron, H. Charvat, M. Araghi, M. Arnold, M. M. Fidler-Benaoudia, A. Bardot, et al., Age disparities in stage‐specific colon cancer survival across seven countries: An International cancer benchmarking partnership SURVMARK‐2 population‐based study, Int. J. Cancer, 148 (2021), 1575–1585. https://doi.org/10.1002/ijc.33326 doi: 10.1002/ijc.33326
|
| [5] |
S. Pilleron, C. Maringe, H. Charvat, J. Atkinson, E. J. A. Morris, D. Sarfati, The impact of timely cancer diagnosis on age disparities in colon cancer survival, J. Geriatr. Oncol., 12 (2021), 1044–1051. https://doi.org/10.1016/j.jgo.2021.04.003 doi: 10.1016/j.jgo.2021.04.003
|
| [6] |
H. Khan, A. J. Olszewski, P. Somasundar, Lymph node involvement in colon cancer patients decreases with age; a population based analysis, Eur. J. Surg. Oncol., 40 (2014), 1474–1480. https://doi.org/10.1016/j.ejso.2014.06.002 doi: 10.1016/j.ejso.2014.06.002
|
| [7] |
H. B. Ding, L. H. Wang, G. Sun, G. Yu, X. Gao, K. Zheng, et al., Evaluation of the learning curve for conformal sphincter preservation operation in the treatment of ultralow rectal cancer, World J. Surg. Oncol., 20 (2022), 102. https://doi.org/10.1186/s12957-022-02541-1 doi: 10.1186/s12957-022-02541-1
|
| [8] |
D. M. Jiang, S. Raissouni, J. Mercer, A. Kumar, R. Goodwin, D. Y. Heng, et al., Clinical outcomes of elderly patients receiving neoadjuvant chemoradiation for locally advanced rectal cancer, Ann. Oncol., 26(2015), 2102–2106. https://doi.org/10.1093/annonc/mdv331 doi: 10.1093/annonc/mdv331
|
| [9] |
N. Mottet, M. J. Ribal, H. Boyle, M. De Santis, P. Caillet, A. Choudhury, et al., Management of bladder cancer in older patients: Position paper of a SIOG Task Force, J. Geriatr. Oncol., 11(2020), 1043–1053. https://doi.org/10.1016/j.jgo.2020.02.001 doi: 10.1016/j.jgo.2020.02.001
|
| [10] |
H. Rutten, M. D. Dulk, V. Lemmens, G. Nieuwenhuijzen, P. Krijnen, M. Jansen-Landheer, et al., Survival of elderly rectal cancer patients not improved: Analysis of population based data on the impact of TME surgery, Eur. J. Cancer, 43 (2007), 2295–2300. https://doi.org/10.1016/j.ejca.2007.07.009 doi: 10.1016/j.ejca.2007.07.009
|
| [11] |
H. Maas, V. Lemmens, P. H. A. Nijhuis, I. H. J. T. de Hingh, C. C. E. Koning, M. L. G. Janssen-Heijnen, Benefits and drawbacks of short-course preoperative radiotherapy in rectal cancer patients aged 75 years and older, Eur. J. Surg. Oncol., 39 (2013), 1087–1093. https://doi.org/10.1016/j.ejso.2013.07.094 doi: 10.1016/j.ejso.2013.07.094
|
| [12] |
M. A. Shahir, V. E. Lemmens, A. C. Voogd, A. C. Voogd, H. Martijn, M. L. G. Janssen-Heijnen, Elderly patients with rectal cancer have a higher risk of treatment-related complications and a poorer prognosis than younger patients: A population-based study, Eur. J. Cancer, 42 (2006), 3015–3021. https://doi.org/10.1016/j.ejca.2005.10.032 doi: 10.1016/j.ejca.2005.10.032
|
| [13] |
S. L. Liu, Y. Zhao, W. M. Hopman, N. Lamond, R. Ramjeesingh, Adjuvant treatment in older patients with rectal cancer: a population-based review, Curr. Oncol., 25(2018), 499–506. https://doi.org/10.3747/co.25.4102 doi: 10.3747/co.25.4102
|
| [14] |
R. Sauer, T. Liersch, S. Merkel, R. Fietkau, W. Hohenberger, C. Hess, et al., Preoperative versus postoperative chemo radiotherapy for locally advanced rectal cancer: Results of the German CAO/ARO/AIO-94 randomized phase Ⅲ trial after a median follow-up of 11 years, J. Clin. Oncol., 30 (2012), 1926–1933. https://doi.org/10.1200/JCO.2011.40.1836 doi: 10.1200/JCO.2011.40.1836
|
| [15] |
E. Kapiteijn, C. A. Marijnen, I. D. Nagtegaal, H. Putter, W. H. Steup, T. Wiggers, et al., Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer, N. Engl. J. Med., 345 (2001), 638–646. https://doi.org/10.1056/NEJMoa010580 doi: 10.1056/NEJMoa010580
|
| [16] |
D. Sebag-Montefiore, R. J. Stephens, R. Steele, J. Monson, R. Grieve, S. Khanna, et al., Preoperative radiotherapy versus selective postoperative chemoradiotherapy in patients with rectal cancer (MRC CR07 and NCIC-CTG C016): A multicentre, randomised trial, Lancet, 373 (2009), 811–820. https://doi.org/10.1016/S0140-6736(09)60484-0 doi: 10.1016/S0140-6736(09)60484-0
|
| [17] |
Q. Song, B. Bates, Y. R. Shao, F. Hsu, F. Liu, V. Madhira, et al., Risk and outcome of breakthrough COVID-19 infections in vaccinated patients with cancer: Real-world evidence from the National COVID Cohort Collaborative, J. Clin. Oncol., 40 (2022), 1414–1427. https://doi.org/10.1200/JCO.21.02419 doi: 10.1200/JCO.21.02419
|
| [18] |
A. Quaglia, A. Tavilla, L. Shack, H. Brenner, M. Janssen-Heijnen, C. Allemani, et al., The cancer survival gap between elderly and middle-aged patients in Europe is widening, Eur. J. Cancer, 45 (2009), 1006–1016. https://doi.org/10.1016/j.ejca.2008.11.028 doi: 10.1016/j.ejca.2008.11.028
|
| [19] |
A. L. Potosky, L. C. Harlan, R. S. Kaplan, K. A. Johnson, C. F. Lynch, Age, sex, and racial differences in the use of standard adjuvant therapy for colorectal cancer, J. Clin. Oncol., 20 (2002), 1192–1202. https://doi.org/10.1200/JCO.2002.20.5.1192 doi: 10.1200/JCO.2002.20.5.1192
|
| [20] |
N. Sharafeldin, B. Bates, Q. Song, V. Madhira, Y. Yan, S. Dong, et al., Outcomes of COVID-19 in patients with cancer: Report from the national COVID cohort collaborative (N3C), J. Clin. Oncol., 39 (2021), 2232–2246. https://doi.org/10.1200/JCO.21.01074 doi: 10.1200/JCO.21.01074
|
| [21] |
A. Wolski, N. Grafféo, R. Giorgi, A permutation test based on the restricted mean survival time for comparison of net survival distributions in non-proportional excess hazard settings, Stat. Methods Med. Res., 29 (2020), 1612–1623. https://doi.org/10.1177/0962280219870217 doi: 10.1177/0962280219870217
|
| [22] |
P. M. Arenas, S. Sabater, M. Bonet, M Gascón, EP-2303: Should radiotherapy be avoided after neoadjuvant chemotherapy in complete response breast cancer?, Radiother. Oncol., 127 (2018), S1271. https://doi.org/10.1016/S0167-8140(18)32612-4 doi: 10.1016/S0167-8140(18)32612-4
|
| [23] |
J. K. Logan, K. E. Huber, T. A. Dipetrillo, D. Wazer, K. Leonard, Patterns of care of radiation therapy in patients with stage Ⅳ rectal cancer: A surveillance, epidemiology, and end results analysis of patients from 2004 to 2009, Cancer, 120 (2014), 731–737. https://doi.org/10.1002/cncr.28467 doi: 10.1002/cncr.28467
|
| [24] |
J. A. Serra-Rexach, A. B. Jimenez, M. A. García-Alhambra, R. Pla, M. Vidán, P. Rodríguez, et al., Differences in the therapeutic approach to colorectal cancer in young and elderly patients, Oncologist, 17 (2012), 1277–1285. https://doi.org/10.1634/theoncologist.2012-0060 doi: 10.1634/theoncologist.2012-0060
|
| [25] |
L. I. Olsson, F. Granstrom, B. Glimelius, Socioeconomic inequalities in the use of radiotherapy for rectal cancer: A nationwide study, Eur. J. Cancer, 47 (2011), 347–353. https://doi.org/10.1016/j.ejca.2010.03.015 doi: 10.1016/j.ejca.2010.03.015
|
| [26] |
J. Faivre, V. E. Lemmens, V. Quipourt, A. M. Bouvier, Management and survival of colorectal cancer in the elderly in population-based studies, Eur. J. Cancer, 43 (2007), 2279–2284. https://doi.org/10.1016/j.ejca.2007.08.008 doi: 10.1016/j.ejca.2007.08.008
|








Figures(9) / Tables(8)

Wei Wang, Tongping Shen, Jiaming Wang. Analysis of the impact of radiotherapy and surgical treatment regimens based on the SEER database on the survival outcomes of rectal cancer patients over 70 years[J]. Mathematical Biosciences and Engineering, 2024, 21(3): 4463-4484. doi: 10.3934/mbe.2024197







 DownLoad:
DownLoad: