Community governance is the basic unit of social governance, and it is also an important direction for building a social governance pattern of co-construction, co-governance and sharing. Previous studies have solved the problems of data security, information traceability and participant enthusiasm in the process of community digital governance by building a community governance system based on blockchain technology and incentive mechanisms. The application of blockchain technology can solve the problems of low data security, difficulty in sharing and tracing and low enthusiasm on the part of multiple subjects regarding participation in community governance. The process of community governance involves the cooperation of multiple government departments and multiple social subjects. Under the blockchain architecture, the number of alliance chain nodes will reach 1000 with the expansion of community governance. The existing consensus algorithms for coalition chains are difficult to meet the high concurrent processing requirements under such large-scale nodes. An optimization algorithm has improved the consensus performance to a certain extent, but the existing systems still cannot meet the data needs of the community and are not suitable for community governance scenarios. Since the community governance process only involves the participation of relevant departments in users, all nodes in the network are not required to participate in the consensus under the blockchain architecture. Therefore, a practical Byzantine fault tolerance (PBFT) optimization algorithm based on community contribution (CSPBFT) is proposed here. First, consensus nodes are set according to different roles of participants in community activities, and participants are given different consensus permissions. Second, the consensus process is divided into different stages, and the amount of data processed by each consensus step is reduced. Finally, a two-level consensus network is designed to perform different consensus tasks, and reduce unnecessary communication between nodes to reduce the communication complexity of consensus among nodes. Compared with the PBFT algorithm, CSPBFT reduces the communication complexity from O(N2) to O(N2/C3). Finally, the simulation results show that, through rights management, network level setting and consensus phase division, when the number of nodes in the CSPBFT network is 100–400, the consensus throughput can reach 2000 TPS. When the node in the network is 1000, the instantaneous concurrency is guaranteed to be above 1000 TPS, which can meet the concurrent needs of the community governance scenario.
Citation: Pengpeng Wang, Xu Wang, Yumin Shen, Jinlong Wang, Xiaoyun Xiong. PBFT optimization algorithm based on community contributions[J]. Mathematical Biosciences and Engineering, 2023, 20(6): 10200-10222. doi: 10.3934/mbe.2023447
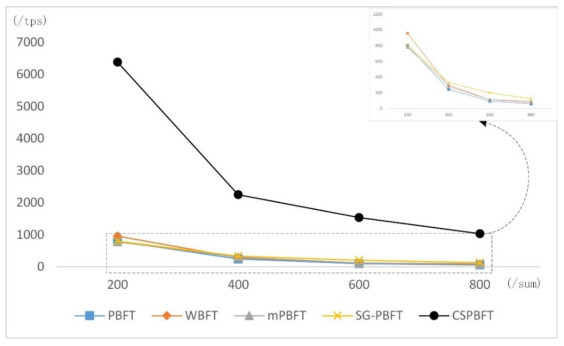
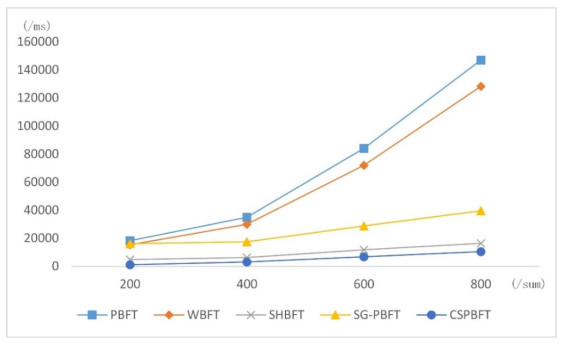
Community governance is the basic unit of social governance, and it is also an important direction for building a social governance pattern of co-construction, co-governance and sharing. Previous studies have solved the problems of data security, information traceability and participant enthusiasm in the process of community digital governance by building a community governance system based on blockchain technology and incentive mechanisms. The application of blockchain technology can solve the problems of low data security, difficulty in sharing and tracing and low enthusiasm on the part of multiple subjects regarding participation in community governance. The process of community governance involves the cooperation of multiple government departments and multiple social subjects. Under the blockchain architecture, the number of alliance chain nodes will reach 1000 with the expansion of community governance. The existing consensus algorithms for coalition chains are difficult to meet the high concurrent processing requirements under such large-scale nodes. An optimization algorithm has improved the consensus performance to a certain extent, but the existing systems still cannot meet the data needs of the community and are not suitable for community governance scenarios. Since the community governance process only involves the participation of relevant departments in users, all nodes in the network are not required to participate in the consensus under the blockchain architecture. Therefore, a practical Byzantine fault tolerance (PBFT) optimization algorithm based on community contribution (CSPBFT) is proposed here. First, consensus nodes are set according to different roles of participants in community activities, and participants are given different consensus permissions. Second, the consensus process is divided into different stages, and the amount of data processed by each consensus step is reduced. Finally, a two-level consensus network is designed to perform different consensus tasks, and reduce unnecessary communication between nodes to reduce the communication complexity of consensus among nodes. Compared with the PBFT algorithm, CSPBFT reduces the communication complexity from O(N2) to O(N2/C3). Finally, the simulation results show that, through rights management, network level setting and consensus phase division, when the number of nodes in the CSPBFT network is 100–400, the consensus throughput can reach 2000 TPS. When the node in the network is 1000, the instantaneous concurrency is guaranteed to be above 1000 TPS, which can meet the concurrent needs of the community governance scenario.

| [1] |
Y. W. Chai, W. B. Guo, Smart management and service of communities in Chinese cities, Prog. Geogr., 34 (2015), 466–472. https://doi.org/10.11820/dlkxjz.2015.04.008 doi: 10.11820/dlkxjz.2015.04.008

|
| [2] | F. Zhang, Study on the holistic governance of mega city community, Urban Dev. Stud., 28 (2021), 1–4+10. |
| [3] |
C. F. Han, Research on innovating mechanisms for community governance based on blockchain, Frontiers, 2020 (2020), 66–75. https://doi.org/10.16619/j.cnki.rmltxsqy.2020.05.007 doi: 10.16619/j.cnki.rmltxsqy.2020.05.007
|
| [4] | S. Nakamoto, Bitcoin: A peer-to-peer electronic cash system, 2022. Available from: https://assets.pubpub.org/d8wct41f/31611263538139.pdf. |
| [5] |
N. Elisa, L. Yang, F. Chao, Y. Cao, A framework of blockchain-based secure and privacy-preserving E-government system, Wireless Netw., 2018. https://doi.org/10.1007/s11276-018-1883-0 doi: 10.1007/s11276-018-1883-0
|
| [6] | Y. Li, H. Y. Duan, Y. Y. Yin, H. H. Gao, Survey of crowdsourcing applications in blockchain systems, Comput. Sci., 48 (2021), 12–27. |
| [7] |
S. Zhu, Z. Cai, H. Hu, Y. Li, W. Li, Zkcrowd: A hybrid blockchain-based crowdsourcing platform, IEEE Trans. Ind. Inf., 16 (2019), 4196–4205. https://doi.org/10.1109/TII.2019.2941735 doi: 10.1109/TII.2019.2941735
|
| [8] |
H. Qin, Y. Cheng, X. Ma, F. Li, J. Abawajy, Weighted Byzantine Fault Tolerance consensus algorithm for enhancing consortium blockchain efficiency and security, J. King Saud Univ. Comput. Inf. Sci., 34 (2022), 8370–8379. https://doi.org/10.1016/j.jksuci.2022.08.017 doi: 10.1016/j.jksuci.2022.08.017
|
| [9] |
Y. Min, The modification of pBFT algorithm to increase network operations efficiency in private blockchains, Appl. Sci., 11 (2021), 6313. https://doi.org/10.3390/app11146313 doi: 10.3390/app11146313
|
| [10] | J. Martins, B. Fernandes, I. Rohman, L. Veiga, The war on corruption: the role of electronic government, in EGOV 2018: Electronic Government, (2018), 98–109. https://doi.org/10.1007/978-3-319-98690-6_9 |
| [11] |
J. A. Garcia-Garcia, N. Sánchez-Gómez, D. Lizcano, M. J. Escalona, T. Wojdyński, Using blockchain to improve collaborative business process management: systematic literature review, IEEE Access, 8 (2020), 142312–142336. https://doi.org/10.1109/ACCESS.2020.3013911 doi: 10.1109/ACCESS.2020.3013911
|
| [12] |
Y. Meshcheryakov, A. Melman, O. Evsutin, V. Morozov, Y. Koucheryavy, On performance of PBFT blockchain consensus algorithm for IoT-applications with constrained devices, IEEE Access, 9 (2021), 80559–80570. https://doi.org/10.1109/ACCESS.2021.3085405 doi: 10.1109/ACCESS.2021.3085405
|
| [13] |
H. Xiong, M. Chen, C. Wu, Y. Zhao, W. Yi, Research on progress of blockchain consensus algorithm: a review on recent progress of blockchain consensus algorithms, Future Internet, 14 (2022), 47. https://doi.org/10.3390/fi14020047 doi: 10.3390/fi14020047
|
| [14] |
H. Samy, A. Tammam, A. Fahmy, B. Hasan, Enhancing the performance of the blockchain consensus algorithm using multithreading technology, Ain Shams Eng. J., 12 (2021), 2709–2716. https://doi.org/10.1016/j.asej.2021.01.019 doi: 10.1016/j.asej.2021.01.019
|
| [15] | M. Pandey, R. Agarwal, S. Shukl, N. K. Verma, Reputation-based PoS for the restriction of illicit activities on blockchain: algorand usecase, preprint, arXiv: 2112.11024. |
| [16] |
G. Xu, H. Bai, J. Xing, T. Luo, N. N. Xiong, X. Cheng, et al., SG-PBFT: A secure and highly efficient blockchain PBFT consensus algorithm for Internet of vehicles, J. Parallel Distrib. Comput., 164 (2022), 1–11. https://doi.org/10.1016/j.jpdc.2022.01.029 doi: 10.1016/j.jpdc.2022.01.029
|
| [17] |
Y. Na, Z. Wen, J. Fang, Y. Tang, Y. Li, A derivative PBFT blockchain consensus algorithm with dual primary nodes based on separation of powers-DPNPBFT, IEEE Access, 10 (2022), 76114–76124. https://doi.org/10.1109/ACCESS.2022.3192426 doi: 10.1109/ACCESS.2022.3192426
|
| [18] |
Y. Li, L. Qiao, Z. Lv, An optimized Byzantine fault tolerance algorithm for consortium blockchain, Peer-to-Peer Networking Appl., 14 (2021), 2826–2839. https://doi.org/10.1007/s12083-021-01103-8 doi: 10.1007/s12083-021-01103-8
|
| [19] |
S. Tang, Z. Wang, J. Jiang, S. Ge, G. Tan, Improved PBFT algorithm for high-frequency trading scenarios of alliance blockchain, Sci. Rep., 12 (2022), 4426. https://doi.org/10.1038/s41598-022-08587-1 doi: 10.1038/s41598-022-08587-1
|
| [20] | Decred btcsuite developers, in US and CA, Decred Documentation, 2023. Available from: https://docs.decred.org/getting-started/project-history/. |
| [21] |
J. L. Wang, X. Wang, Y. M. Shen, X. Y. Xiong, W. H. Zheng, P. Li, et al., Building operation and maintenance scheme based on sharding blockchain, Heliyon, 9 (2023), E13186. https://doi.org/10.1016/j.heliyon.2023.e13186 doi: 10.1016/j.heliyon.2023.e13186
|
| [22] |
H. W. Huang, W. Kong, X. W. Peng, Z. B. Zheng, Survey on blockchain sharding technology, Comput. Eng., 48 (2022), 1–10. https://doi.org/10.19678/j.issn.1000-3428.0063887 doi: 10.19678/j.issn.1000-3428.0063887
|



Figures(13) / Tables(2)

Pengpeng Wang, Xu Wang, Yumin Shen, Jinlong Wang, Xiaoyun Xiong. PBFT optimization algorithm based on community contributions[J]. Mathematical Biosciences and Engineering, 2023, 20(6): 10200-10222. doi: 10.3934/mbe.2023447







 DownLoad:
DownLoad: