Due to its chronic and progressive nature, chronic kidney disease (CKD) affects patients in many spheres including their perception of quality of life (QOL). Breathing training techniques have shown positive effects on health and QOL for different conditions.
The aim of this study was to perform a scoping review to examine the characteristics related to the application of breathing training on patients with CKD, and to identify the relevant outcomes and target group for the application of breathing training.
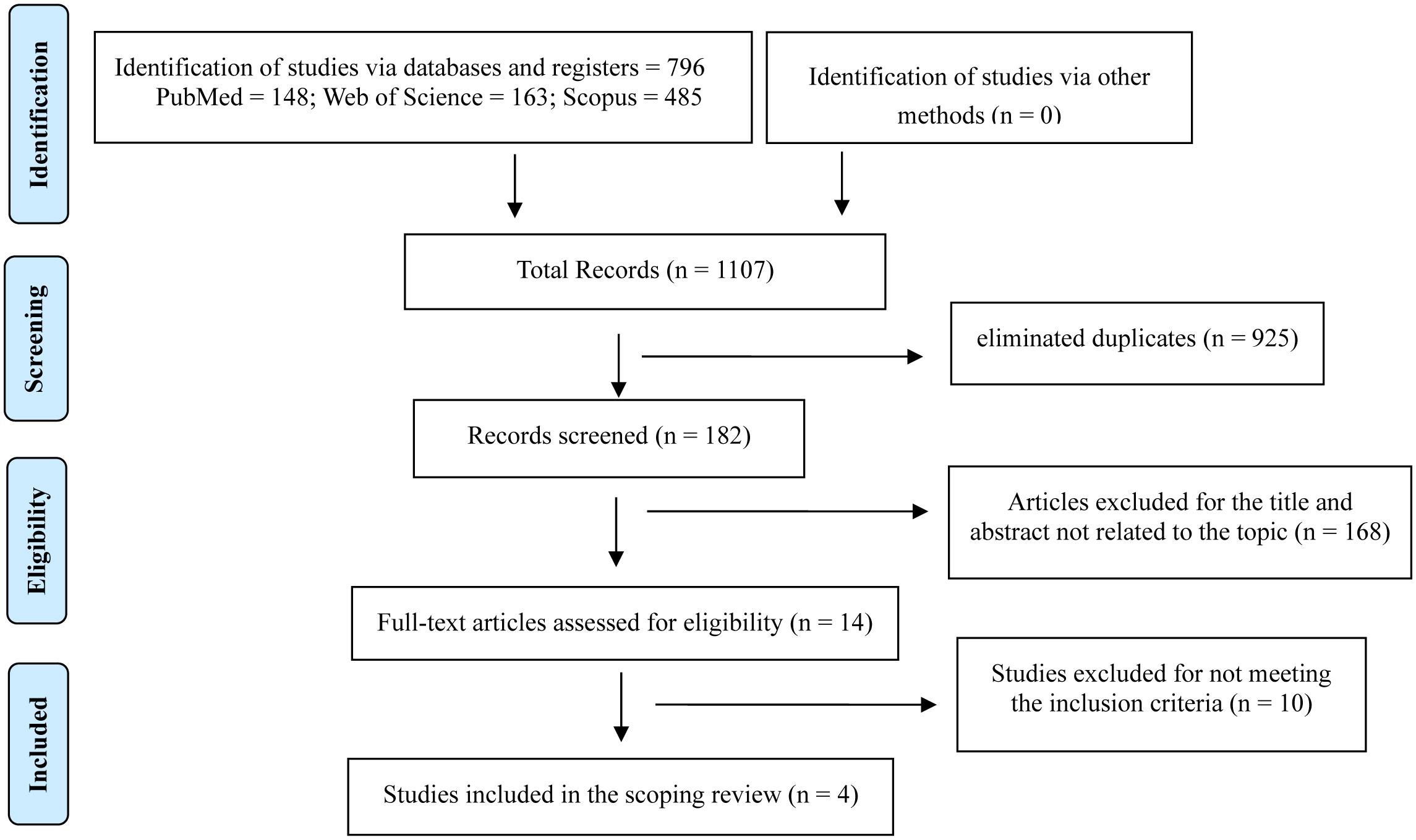
This scoping review was performed in accordance with PRISMA-SRc guidelines. We systematically searched three electronic databases for articles published before March 2022. The studies included patients with chronic kidney disease that received breathing training programs. The breathing training programs were compared to usual care or no treatment.
A total of four studies were included in this scoping review. The four studies had heterogeneous disease stages and breathing training programs. All the studies included reported positive effects of breathing training programs on QOL of CKD patients.
The breathing training programs were able to improve the quality of life of patients with CKD undergoing hemodialysis treatment.
Citation: Ana I. Rubio-López, Alejandro Heredia-Ciuró, Jorge L. Marin-DelaRosa, Javier Martín-Núñez, María Granados-Santiago, María C. De Gracia-Guindo, Marie C. Valenza. Role of breathing training programs on quality of life in chronic kidney disease patients[J]. AIMS Public Health, 2023, 10(2): 409-421. doi: 10.3934/publichealth.2023029
Due to its chronic and progressive nature, chronic kidney disease (CKD) affects patients in many spheres including their perception of quality of life (QOL). Breathing training techniques have shown positive effects on health and QOL for different conditions.
The aim of this study was to perform a scoping review to examine the characteristics related to the application of breathing training on patients with CKD, and to identify the relevant outcomes and target group for the application of breathing training.
This scoping review was performed in accordance with PRISMA-SRc guidelines. We systematically searched three electronic databases for articles published before March 2022. The studies included patients with chronic kidney disease that received breathing training programs. The breathing training programs were compared to usual care or no treatment.
A total of four studies were included in this scoping review. The four studies had heterogeneous disease stages and breathing training programs. All the studies included reported positive effects of breathing training programs on QOL of CKD patients.
The breathing training programs were able to improve the quality of life of patients with CKD undergoing hemodialysis treatment.

| [1] |
Hill NR, Fatoba ST, Oke JL, et al. (2016) Global Prevalence of Chronic Kidney Disease - A Systematic Review and Meta-Analysis. PLoS One 11: e0158765. https://doi.org/10.1371/journal.pone.0158765 
|
| [2] |
Garibotto G (2021) A Changing Perspective for Treatment of Chronic Kidney Disease. J Clin Med 10: 3840. https://doi.org/10.3390/jcm10173840
|
| [3] |
Neuen BL, Chadban SJ, Demaio AR, et al. (2017) Chronic kidney disease and the global NCDs agenda. BMJ Glob Health 2: e000380. https://doi.org/10.1136/bmjgh-2017-000380
|
| [4] |
Charles C, Ferris AH (2020) Chronic Kidney Disease. Prim Care Clin Off Pract 47: 585-595. https://doi.org/10.1016/j.pop.2020.08.001
|
| [5] |
Murabito S, Hallmark BF (2018) Complications of Kidney Disease. Nurs Clin North Am 53: 579-588. https://doi.org/10.1016/j.cnur.2018.07.010
|
| [6] |
Murphy D, McCulloch CE, Lin F, et al. (2016) Trends in Prevalence of Chronic Kidney Disease in the United States. Ann Intern Med 165: 473-481. https://doi.org/10.7326/M16-0273
|
| [7] |
Jesus NM, Souza GF de, Mendes-Rodrigues C, et al. (2019) Quality of life of individuals with chronic kidney disease on dialysis. J Bras Nefrol 41: 364-374. https://doi.org/10.1590/2175-8239-jbn-2018-0152
|
| [8] |
Navaneethan SD, Mandayam S, Arrigain S, et al. (2016) Obstructive and Restrictive Lung Function Measures and CKD: National Health and Nutrition Examination Survey (NHANES) 2007–2012. Am J Kidney Dis 68: 414-421. https://doi.org/10.1053/j.ajkd.2016.03.415
|
| [9] |
Mukai H, Ming P, Lindholm B, et al. (2018) Lung Dysfunction and Mortality in Patients with Chronic Kidney Disease. Kidney Blood Press Res 43: 522-535. https://doi.org/10.1159/000488699
|
| [10] |
Teixeira CG, Duarte MDCMB, Prado CM, et al. (2014) Impact of chronic kidney disease on quality of life, lung function, and functional capacity. J Pediatr 90: 580-586. https://doi.org/10.1016/j.jped.2014.03.002
|
| [11] |
Kunwar D, Kunwar R, Shrestha B, et al. (2020) Depression and Quality of Life among the Chronic Kidney Disease Patients. J Nepal Health Res Counc 18: 459-465. https://doi.org/10.33314/jnhrc.v18i3.2556
|
| [12] |
Bull FC, Al-Ansari SS, Biddle S, et al. (2020) World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports Med 54: 1451-1462. https://doi.org/10.1136/bjsports-2020-102955
|
| [13] | Liguori G, Feito Y, Fountaine C, et al. (2021) American College of Sports MedicineACSM's Guidelines for Exercise Testing and Prescription. Philadelphia, USA: Wolters Kluwer Health. |
| [14] |
Batrakoulis A (2019) European Fitness Trends for 2020. ACSMs Health Fit J 23: 28-35. https://doi.org/10.1249/FIT.0000000000000523
|
| [15] |
Kercher VM, Kercher K, Bennion T, et al. (2022) 2022 Fitness Trends from Around the Globe. ACSMs Health Fit J 26: 21-37. https://doi.org/10.1249/FIT.0000000000000737
|
| [16] |
Illi SK, Held U, Frank I, et al. (2012) Effect of respiratory muscle training on exercise performance in healthy individuals: a systematic review and meta-analysis. Sports Med 42: 707-724. https://doi.org/10.1007/BF03262290
|
| [17] |
Fabero-Garrido R, Del Corral T, Angulo-Díaz-Parreño S, et al. (2022) Respiratory muscle training improves exercise tolerance and respiratory muscle function/structure post-stroke at short term: A systematic review and meta-analysis. Ann Phys Rehabil Med 65: 101596. https://doi.org/10.1016/j.rehab.2021.101596
|
| [18] | Hamasaki H (2020) Effects of Diaphragmatic Breathing on Health: A Narrative Review. Med 7: 65. https://doi.org/10.3390/medicines7100065 |
| [19] |
Tricco AC, Lillie E, Zarin W, et al. (2018) PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med 169: 467-473. https://doi.org/10.7326/M18-0850
|
| [20] |
Arksey H, O'Malley L (2005) Scoping studies: towards a methodological framework. Int J Soc Res Methodol 8: 19-32. https://doi.org/10.1080/1364557032000119616
|
| [21] |
Munn Z, Peters MDJ, Stern C, et al. (2018) Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med Res Methodol 18: 143. https://doi.org/10.1186/s12874-018-0611-x
|
| [22] |
Downs SH, Black N (1998) The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Heal 52: 377-384. https://doi.org/10.1136/jech.52.6.377
|
| [23] |
Deeks JJ, Dinnes J, D'Amico R, et al. (2003) Evaluating non-randomised intervention studies. Health Technol Assess 7: iii-173. https://doi.org/10.3310/hta7270
|
| [24] |
Saunders LD, Soomro GM, Buckingham J, et al. (2003) Assessing the methodological quality of nonrandomized intervention studies. West J Nurs Res 25: 223-237. https://doi.org/10.1177/0193945902250039
|
| [25] | Higgins JP, Thomas J, Chandler J (2019) Cochrane Handbook for Systematic Reviews of Interventions. John Wiley & Sons . https://doi.org/10.1002/9781119536604 |
| [26] | Higgins JPT, Altman DG, Gøtzsche PC, et al. (2011) The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ 343. https://doi.org/10.1136/bmj.d5928 |
| [27] |
Tsai SH, Wang MY, Miao NF, et al. (2015) CE: Original Research: The Efficacy of a Nurse-Led Breathing Training Program in Reducing Depressive Symptoms in Patients on Hemodialysis: A Randomized Controlled Trial. Am J Nurs 115: 24-32. https://doi.org/10.1097/01.NAJ.0000463023.48226.16
|
| [28] |
Kharbteng L, Monaliza, Kumar V, et al. (2020) Effectiveness of a Breathing Training Program on Quality of Life in Patients with Predialysis Chronic Kidney Disease: A Randomized Controlled Trial. Indian J Palliat Care 26: 271-275. https://doi.org/10.4103/IJPC.IJPC_118_19
|
| [29] |
Huang HY, Hung KS, Yeh ML, et al. (2021) Breathing-based leg exercises during hemodialysis improve quality of life: A randomized controlled trial. Clin Rehabil 35: 1175-1184. https://doi.org/10.1177/02692155211000738
|
| [30] | Kaneko K, Taneichi A, Sato Y, et al. (2021) Effects of Slow Breathing Exercise in Chronic Kidney Disease Patients. Int Med J 28. |
| [31] |
Sovatzidis A, Chatzinikolaou A, Fatouros IG, et al. (2020) Intradialytic Cardiovascular Exercise Training Alters Redox Status, Reduces Inflammation and Improves Physical Performance in Patients with Chronic Kidney Disease. Antioxidants 9: 868. https://doi.org/10.3390/antiox9090868
|
| [32] |
Lu Y, Li P, Li N, et al. (2020) Effects of Home-Based Breathing Exercises in Subjects With COPD. Respir Care 65: 377-387. https://doi.org/10.4187/respcare.07121
|
| [33] | Levendoğlu F, Altintepe L, Okudan N, et al. (2004) A twelve-week exercise program improves the psychological status, quality of life and work capacity in hemodialysis patients. J Nephrol 17: 826-832. |
| [34] |
Wang MH, Yeh ML (2019) Respiratory training interventions improve health status of heart failure patients: A systematic review and network meta-analysis of randomized controlled trials. World J Clin cases 7: 2760-2775. https://doi.org/10.12998/wjcc.v7.i18.2760
|
| [35] |
Ubolnuar N, Tantisuwat A, Thaveeratitham P, et al. (2019) Effects of Breathing Exercises in Patients With Chronic Obstructive Pulmonary Disease: Systematic Review and Meta-Analysis. Ann Rehabil Med 43: 509-523. https://doi.org/10.5535/arm.2019.43.4.509
|
| [36] |
Menezes KKP, Nascimento LR, Ada L, et al. (2016) Respiratory muscle training increases respiratory muscle strength and reduces respiratory complications after stroke: a systematic review. J Physiother 62: 138-144. https://doi.org/10.1016/j.jphys.2016.05.014
|
 publichealth-10-02-029-s001.pdf publichealth-10-02-029-s001.pdf |
 |
Figures(1) / Tables(2)

Ana I. Rubio-López, Alejandro Heredia-Ciuró, Jorge L. Marin-DelaRosa, Javier Martín-Núñez, María Granados-Santiago, María C. De Gracia-Guindo, Marie C. Valenza. Role of breathing training programs on quality of life in chronic kidney disease patients[J]. AIMS Public Health, 2023, 10(2): 409-421. doi: 10.3934/publichealth.2023029







 DownLoad:
DownLoad: