Coronary artery calcium (CAC) poses a major challenge during percutaneous coronary intervention (PCI). The prevalence of significant calcium is reported to be as high as 32%, with higher incidences in the male sex, alongside hypertension, an ST-segment elevation myocardial infarction (STEMI) presentation, and an advancing age. The identification and modification of calcium is important as an association between the presence of CAC and the observation of major adverse cardiovascular events, even in asymptomatic patients. Although angiographically-identified calcium likely reflects the highest burden disease, an inability to assess the calcium, both qualitatively and quantitatively, limits the interventionists in their strategy to achieve an optimal PCI result. Additionally, treating a stent underexpansion in a heavily calcified vessel is more difficult than preventing it. Intra-coronary imaging modalities such as optical coherence tomography (OCT) and intra-vascular ultrasound (IVUS) offer upfront valuable information that may guide the choice of calcium modification tools, evaluate the efficacy of modification/debulking, and permit an optimal stent expansion. Contemporary randomised studies of intra-coronary imaging- vs angiography-guided intervention have demonstrated a clear benefit in adopting an image-guided approach. This review article summarises the value of IVUS and OCT in patients who present with severe calcific diseases.
Citation: Nitin Chandra Mohan, Thomas W. Johnson. Role of intracoronary imaging in severely calcific disease[J]. AIMS Medical Science, 2024, 11(4): 388-402. doi: 10.3934/medsci.2024027
Coronary artery calcium (CAC) poses a major challenge during percutaneous coronary intervention (PCI). The prevalence of significant calcium is reported to be as high as 32%, with higher incidences in the male sex, alongside hypertension, an ST-segment elevation myocardial infarction (STEMI) presentation, and an advancing age. The identification and modification of calcium is important as an association between the presence of CAC and the observation of major adverse cardiovascular events, even in asymptomatic patients. Although angiographically-identified calcium likely reflects the highest burden disease, an inability to assess the calcium, both qualitatively and quantitatively, limits the interventionists in their strategy to achieve an optimal PCI result. Additionally, treating a stent underexpansion in a heavily calcified vessel is more difficult than preventing it. Intra-coronary imaging modalities such as optical coherence tomography (OCT) and intra-vascular ultrasound (IVUS) offer upfront valuable information that may guide the choice of calcium modification tools, evaluate the efficacy of modification/debulking, and permit an optimal stent expansion. Contemporary randomised studies of intra-coronary imaging- vs angiography-guided intervention have demonstrated a clear benefit in adopting an image-guided approach. This review article summarises the value of IVUS and OCT in patients who present with severe calcific diseases.

| [1] |
Généreux P, Madhavan MV, Mintz GS, et al. (2014) Ischemic outcomes after coronary intervention of calcified vessels in acute coronary syndromes. Pooled analysis from the HORIZONS-AMI (Harmonizing Outcomes With Revascularization and Stents in Acute Myocardial Infarction) and ACUITY (Acute Catheterization and Urgent Intervention Triage Strategy) trials. J Am Coll Cardiol 63: 1845-1854. https://doi.org/10.1016/j.jacc.2014.01.034 
|
| [2] |
Petousis S, Skalidis E, Zacharis E, et al. (2023) The role of intracoronary imaging for the management of calcified lesions. J Clin Med 12: 4622. https://doi.org/10.3390/jcm12144622
|
| [3] |
O'Donnell CJ, Kavousi M, Smith AV, et al. (2011) Genome-wide association study for coronary artery calcification with follow-up in myocardial infarction. Circulation 124: 2855-2864. https://doi.org/10.1161/CIRCULATIONAHA.110.974899
|
| [4] |
Zhang M, Matsumura M, Usui E, et al. (2021) Intravascular ultrasound-derived calcium score to predict stent expansion in severely calcified lesions. Circ Cardiovasc Interv 14: e010296. https://doi.org/10.1161/CIRCINTERVENTIONS.120.010296
|
| [5] |
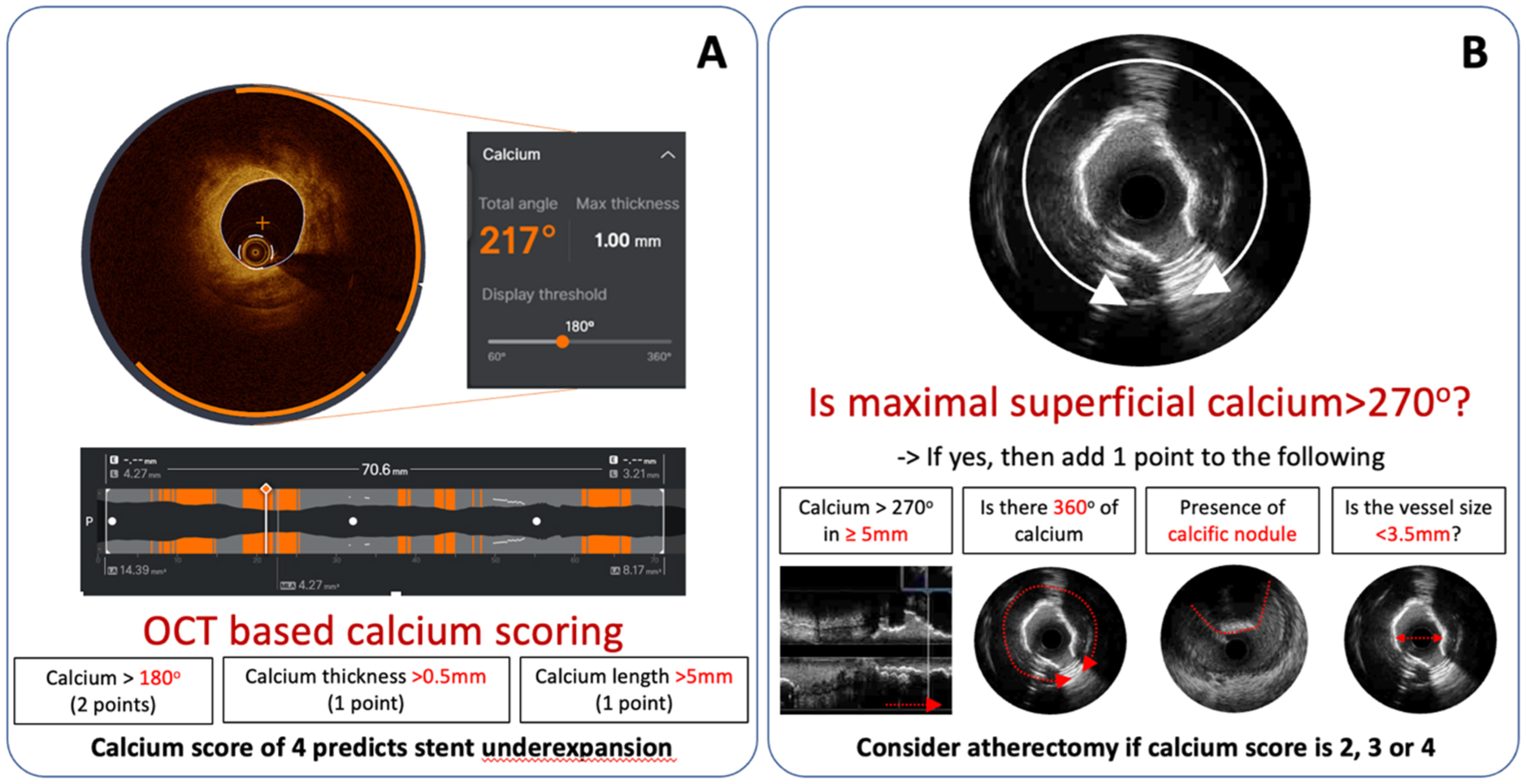
Fujino A, Mintz GS, Matsumura M, et al. (2018) A new optical coherence tomography-based calcium scoring system to predict stent underexpansion. EuroIntervention 13: e2182-e2189. https://doi.org/10.4244/EIJ-D-17-00962
|
| [6] |
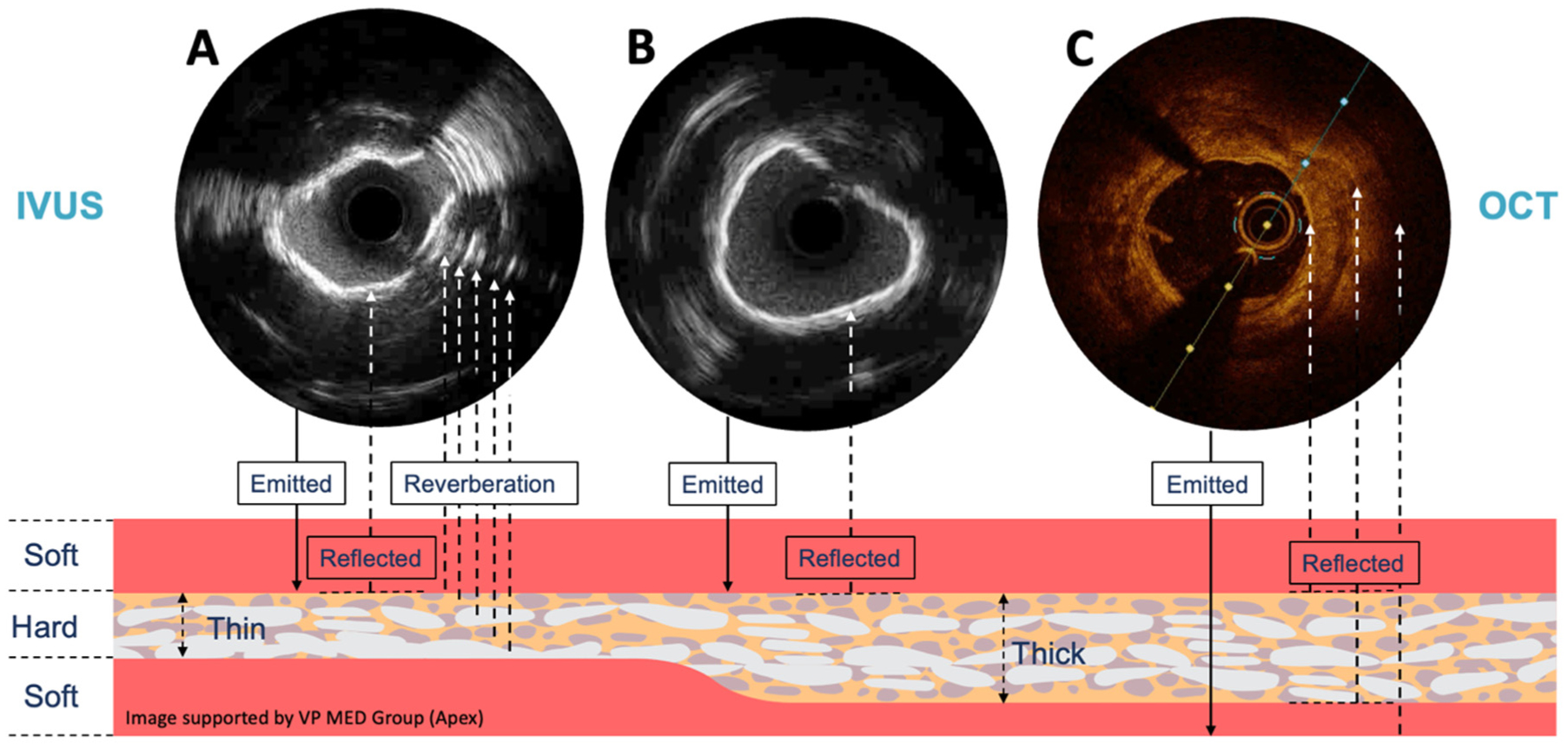
Wang X, Matsumura M, Mintz GS, et al. (2017) In vivo calcium detection by comparing optical coherence tomography, intravascular ultrasound, and angiography. JACC Cardiovasc Imaging 10: 869-879. https://doi.org/10.1016/j.jcmg.2017.05.014
|
| [7] |
Mintz GS, Painter JA, Pichard AD, et al. (1995) Atherosclerosis in angiographically “normal” coronary artery reference segments: an intravascular ultrasound study with clinical correlations. J Am Coll Cardiol 25: 1479-1485. https://doi.org/10.1016/0735-1097(95)00088-l
|
| [8] |
Lee JM, Choi KH, Song YB, et al. (2023) Intravascular imaging-guided or angiography-guided complex PCI. N Engl J Med 388: 1668-1679. https://doi.org/10.1056/NEJMoa2216607
|
| [9] |
Zhang J, Gao X, Kan J, et al. (2018) Intravascular ultrasound versus angiography-guided drug-eluting stent implantation: the ULTIMATE trial. J Am Coll Cardiol 72: 3126-3137. https://doi.org/10.1016/j.jacc.2018.09.013
|
| [10] |
Mintz GS (2015) Intravascular imaging of coronary calcification and its clinical implications. JACC Cardiovasc Imaging 8: 461-471. https://doi.org/10.1016/j.jcmg.2015.02.003
|
| [11] |
Mohan NC, Johnson TW (2022) Intracoronary optical coherence tomography—an introduction. Catheter Cardio Inte 100: S57-S65. https://doi.org/10.1002/ccd.30583
|
| [12] |
Chandramohan N, Hinton J, O'Kane P, et al. (2024) Artificial intelligence for the interventional cardiologist: powering and enabling OCT image interpretation. Interv Cardiol 19: e03. https://doi.org/10.15420/icr.2023.13
|
| [13] |
Tearney GJ, Regar E, Akasaka T, et al. (2012) Consensus standards for acquisition, measurement, and reporting of intravascular optical coherence tomography studies: a report from the international working group for intravascular optical coherence tomography standardization and validation. J Am Coll Cardiol 59: 1058-1072. https://doi.org/10.1016/j.jacc.2011.09.079
|
| [14] |
Kubo T, Shimamura K, Ino Y, et al. (2015) Superficial calcium fracture after PCI as assessed by OCT. JACC Cardiovasc Imaging 8: 1228-1229. https://doi.org/10.1016/j.jcmg.2014.11.012
|
| [15] |
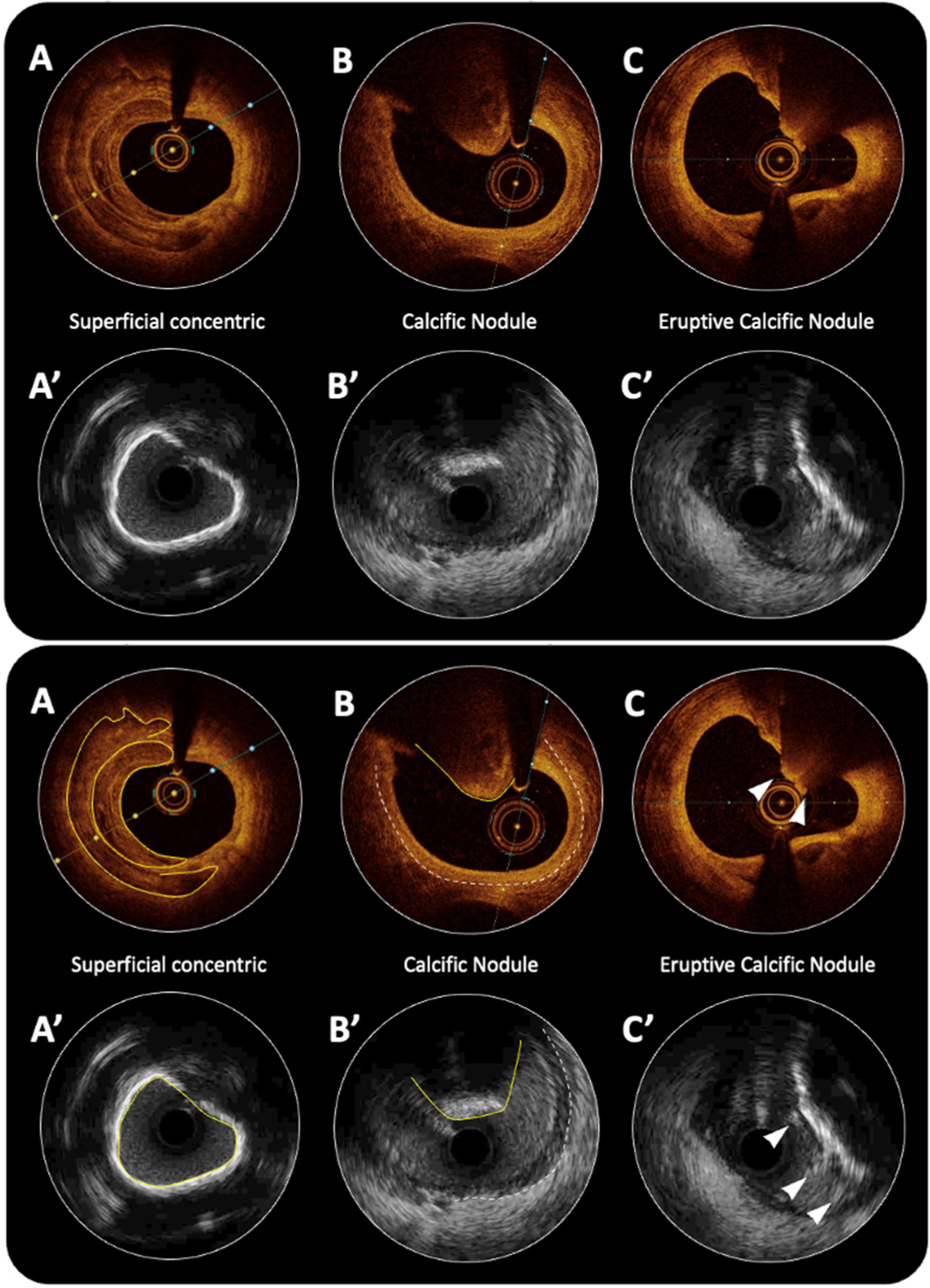
Shin D, Karimi Galougahi K, Spratt JC, et al. (2024) Calcified nodule in percutaneous coronary intervention: therapeutic challenges. JACC Cardiovasc Interv 17: 1187-1199. https://doi.org/10.1016/j.jcin.2024.03.032
|
| [16] |
Sato T, Matsumura M, Yamamoto K, et al. (2023) Impact of eruptive vs noneruptive calcified nodule morphology on acute and long-term outcomes after stenting. JACC Cardiovasc Interv 16: 1024-1035. https://doi.org/10.1016/j.jcin.2023.03.009
|
| [17] |
Malek AM, Alper SL, Izumo S (1999) Hemodynamic shear stress and its role in atherosclerosis. JAMA 282: 2035-2042. https://doi.org/10.1001/jama.282.21.2035
|
| [18] |
Xu Y, Mintz GS, Tam A, et al. (2012) Prevalence, distribution, predictors, and outcomes of patients with calcified nodules in native coronary arteries: a 3-vessel intravascular ultrasound analysis from Providing Regional Observations to Study Predictors of Events in the Coronary Tree (PROSPECT). Circulation 126: 537-545. https://doi.org/10.1161/CIRCULATIONAHA.111.055004
|
| [19] |
Torii S, Sato Y, Otsuka F, et al. (2021) Eruptive calcified nodules as a potential mechanism of acute coronary thrombosis and sudden death. J Am Coll Cardiol 77: 1599-1611. https://doi.org/10.1016/j.jacc.2021.02.016
|
| [20] |
Virmani R, Kolodgie FD, Burke AP, et al. (2000) Lessons from sudden coronary death: a comprehensive morphological classification scheme for atherosclerotic lesions. Arterioscler Thromb Vasc Biol 20: 1262-1275. https://doi.org/10.1161/01.atv.20.5.1262
|
| [21] |
Johnson TW, Räber L, Di Mario C, et al. (2019) Clinical use of intracoronary imaging. Part 2: acute coronary syndromes, ambiguous coronary angiography findings, and guiding interventional decision-making: an expert consensus document of the European Association of Percutaneous Cardiovascular Interventions: endorsed by the Chinese Society of Cardiology, the Hong Kong Society of Transcatheter Endocardiovascular Therapeutics (HKSTENT) and the Cardiac Society of Australia and New Zealand. Eur Heart J 40: 2566-2584. https://doi.org/10.1093/eurheartj/ehz332
|
| [22] |
Jia H, Abtahian F, Aguirre AD, et al. (2013) In vivo diagnosis of plaque erosion and calcified nodule in patients with acute coronary syndrome by intravascular optical coherence tomography. J Am Coll Cardiol 62: 1748-1758. https://doi.org/10.1016/j.jacc.2013.05.071
|
| [23] |
Sugiyama T, Yamamoto E, Fracassi F, et al. (2019) Calcified plaques in patients with acute coronary syndromes. JACC Cardiovasc Interv 12: 531-540. https://doi.org/10.1016/j.jcin.2018.12.013
|
| [24] |
Jeger RV, Eccleshall S, Wan Ahmad WA, et al. (2020) Drug-coated balloons for coronary artery disease: third report of the international DCB consensus group. JACC Cardiovasc Interv 13: 1391-1402. https://doi.org/10.1016/j.jcin.2020.02.043
|
| [25] |
Räber L, Mintz GS, Koskinas K C, et al. (2018) Clinical use of intracoronary imaging. Part 1: guidance and optimization of coronary interventions. An expert consensus document of the European Association of Percutaneous Cardiovascular Interventions. Eur Heart J 39: 3281-3300. https://doi.org/10.1093/eurheartj/ehy285
|
| [26] |
Osborn EA, Johnson M, Maksoud A, et al. (2023) Safety and efficiency of percutaneous coronary intervention using a standardised optical coherence tomography workflow. EuroIntervention 18: 1178-1187. https://doi.org/10.4244/EIJ-D-22-00512
|
| [27] |
Bergmark B, Dallan LAP, Pereira GTR, et al. (2022) Decision-making during percutaneous coronary intervention guided by optical coherence tomography: insights from the LightLab initiative. Circ Cardiovasc Interv 15: 872-881. https://doi.org/10.1161/CIRCINTERVENTIONS.122.011851
|
| [28] |
Shah M, Najam O, Bhindi R, et al. (2021) Calcium modification techniques in complex percutaneous coronary intervention. Circ Cardiovasc Interv 14: e009870. https://doi.org/10.1161/CIRCINTERVENTIONS.120.009870
|
| [29] |
De Maria GL, Scarsini R, Banning AP (2019) Management of calcific coronary artery lesions: Is it time to change our interventional therapeutic approach?. JACC Cardiovasc Interv 12: 1465-1478. https://doi.org/10.1016/j.jcin.2019.03.038
|
| [30] |
Maejima N, Hibi K, Saka K, et al. (2016) Relationship between thickness of calcium on optical coherence tomography and crack formation after balloon dilatation in calcified plaque requiring rotational atherectomy. Circ J 80: 1413-1419. https://doi.org/10.1253/circj.CJ-15-1059
|
| [31] |
Hoffmann R, Mintz GS, Popma JJ, et al. (1998) Treatment of calcified coronary lesions with Palmaz-Schatz stents. An intravascular ultrasound study. Eur Heart J 19: 1224-1231. https://doi.org/10.1053/euhj.1998.1028
|
| [32] |
Song J, Ascherman B, Eudailey KW, et al. (2017) Long-term failure of Amplatzer plugs in the treatment of aortic pathology. J Card Surg 32: 426-429. https://doi.org/10.1111/jocs.13166
|
| [33] |
Rheude T, Rai H, Richardt G, et al. (2021) Super high-pressure balloon versus scoring balloon to prepare severely calcified coronary lesions: the ISAR-CALC randomised trial. EuroIntervention 17: 481-488. https://doi.org/10.4244/EIJ-D-20-01000
|
| [34] |
Hill JM, Kereiakes DJ, Shlofmitz RA, et al. (2020) Intravascular lithotripsy for treatment of severely calcified coronary artery disease. J Am Coll Cardiol 76: 2635-2646. https://doi.org/10.1016/j.jacc.2020.09.603
|
| [35] | Ali ZA, Kereiakes DJ, Hill JM, et al. (2023) Impact of calcium eccentricity on the safety and effectiveness of coronary intravascular lithotripsy: pooled analysis from the disrupt CAD studies. Circ Cardiovasc Interv 16: e012898. https://doi.org/10.1161/CIRCINTERVENTIONS.123.012898 |
| [36] |
Honton B, Cayla G, Lhermusier T, et al. (2024) National france LILI registry on intravascular lithotripsy: 30 days follow up. Arch Cardiovasc Dis 117: S15-S16. https://doi.org/10.1016/j.acvd.2023.10.028
|
| [37] |
Hamana T, Kawamori H, Toba T, et al. (2023) Prediction of the debulking effect of rotational atherectomy using optical frequency domain imaging: a prospective study. Cardiovasc Interv Ther 38: 316-326. https://doi.org/10.1007/s12928-023-00928-9
|
| [38] |
Isogai T, Yasunaga H, Matsui H, et al. (2016) Relationship between hospital volume and major cardiac complications of rotational atherectomy: a nationwide retrospective cohort study in Japan. J Cardiol 67: 442-448. https://doi.org/10.1016/j.jjcc.2015.07.008
|
| [39] |
Meraj PM, Shlofmitz E, Kaplan B, et al. (2018) Clinical outcomes of atherectomy prior to percutaneous coronary intervention: a comparison of outcomes following rotational versus orbital atherectomy (COAP-PCI study). J Interv Cardiol 31: 478-485. https://doi.org/10.1111/joic.12511
|
| [40] |
Yamamoto MH, Maehara A, Karimi Galougahi K, et al. (2017) Mechanisms of orbital versus rotational atherectomy plaque modification in severely calcified lesions assessed by optical coherence tomography. JACC Cardiovasc Interv 10: 2584-2586. https://doi.org/10.1016/j.jcin.2017.09.031
|
| [41] |
Barbato E, Carrié D, Dardas P, et al. (2015) European expert consensus on rotational atherectomy. EuroIntervention 11: 30-36. https://doi.org/10.4244/EIJV11I1A6
|
| [42] |
Allali A, Toelg R, Abdel-Wahab M, et al. (2022) Combined rotational atherectomy and cutting balloon angioplasty prior to drug-eluting stent implantation in severely calcified coronary lesions: the PREPARE-CALC-COMBO study. Catheter Cardiovasc Interv 100: 979-989. https://doi.org/10.1002/ccd.30423
|
| [43] |
Abdel-Wahab M, Toelg R, Byrne RA, et al. (2018) High-speed rotational atherectomy versus modified balloons prior to drug-eluting stent implantation in severely calcified coronary lesions. Circ Cardiovasc Interv 11: e007415. https://doi.org/10.1161/CIRCINTERVENTIONS.118.007415
|
| [44] |
Généreux P, Bettinger N, Redfors B, et al. (2016) Two-year outcomes after treatment of severely calcified coronary lesions with the orbital atherectomy system and the impact of stent types: Insight from the ORBIT II trial. Catheter Cardiovasc Interv 88: 369-377. https://doi.org/10.1002/ccd.26554
|
| [45] |
Morlacchi S, Pennati G, Petrini L, et al. (2014) Influence of plaque calcifications on coronary stent fracture: a numerical fatigue life analysis including cardiac wall movement. J Biomech 47: 899-907. https://doi.org/10.1016/j.jbiomech.2014.01.007
|
| [46] |
Maehara A, Mintz GS, Bui AB, et al. (2002) Incidence, morphology, angiographic findings, and outcomes of intramural hematomas after percutaneous coronary interventions: an intravascular ultrasound study. Circulation 105: 2037-2042. https://doi.org/10.1161/01.cir.0000015503.04751.bd
|
| [47] |
Liu X, Tsujita K, Maehara A, et al. (2009) Intravascular ultrasound assessment of the incidence and predictors of edge dissections after drug-eluting stent implantation. JACC Cardiovasc Interv 2: 997-1004. https://doi.org/10.1016/j.jcin.2009.07.012
|
Figures(3)

Nitin Chandra Mohan, Thomas W. Johnson. Role of intracoronary imaging in severely calcific disease[J]. AIMS Medical Science, 2024, 11(4): 388-402. doi: 10.3934/medsci.2024027







 DownLoad:
DownLoad: