Across the globe, the coronavirus (COVID-19) pandemic has altered the delivery of healthcare services as patients must maintain their distance from caregivers, and still receive medical treatment. This has triggered a necessity for exploring means which minimizes the physical gap between patients and healthcare givers while offering health care and ensuring high medical protection at a reduced risk of exposure. Even though telehealth services are no replacement for conventional healthcare, its' usefulness in the coronavirus (COVID-19) pandemic is immense.
This research reviews the ardent utilization, barriers and recommendations with telehealth services for healthcare delivery during the COVID-19 pandemic.
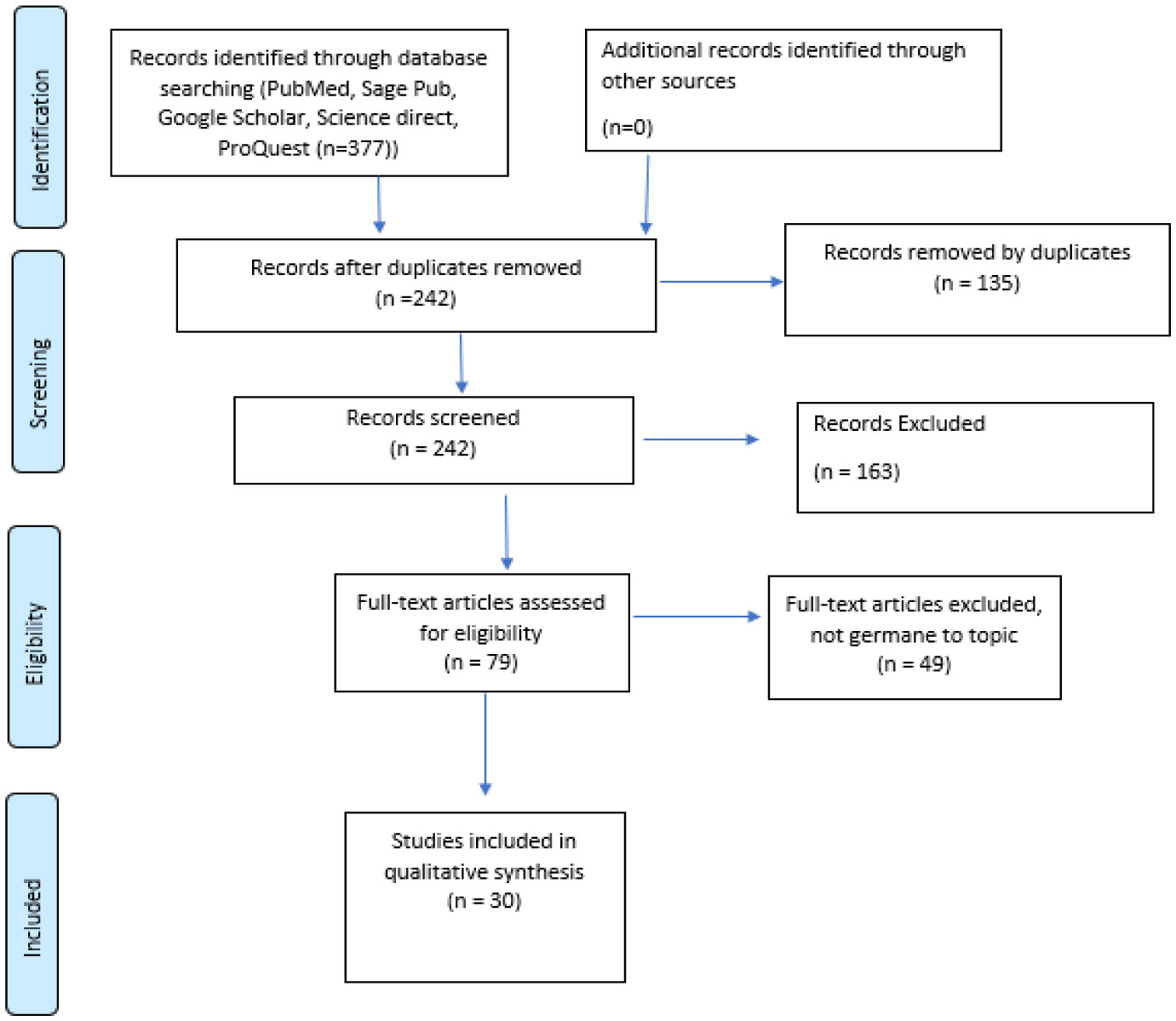
An assessment of literature in five large digital databases; PubMed, Science Direct, Sage Pub, ProQuest, and Google Scholar was conducted. Inclusion criteria included studies defining telehealth/telemedicine, utilization, barriers and recommendations during the COVID-19 pandemic from January 2020 to July 2021, written in English and published in peer-reviewed journals. Two reviewers independently assessed search results, extracted data, and assessed the quality of the included studies. Narrative synthesis was undertaken to summarize and report the findings.
Overall, the study discoveries which are most commonly stated as impediments for telehealth services' full utilization between patients and physicians beyond the scope of typical medical confinement are: infrastructure and internet access (20.00%), data privacy and security (13.33%), digital literacy (13.33%), reimbursement and liability (10.00%), and clinician and patient's unwillingness (6.67%).
The intrusion of coronavirus has accelerated the transition to telehealth services in healthcare delivery, but it has also provided a unique chance to demonstrate the critical role that telehealth can play in ensuring that people of all races, ethnicities, and communities receive high-quality treatment (justice). Healthcare professionals should emphasize the effectiveness of telehealth services as an alternate healthcare delivery method in promoting healthcare to all populace.
Citation: Jonathan Kissi, Daniel Kwame Kwansah Quansah, Jonathan Aseye Nutakor, Alex Boadi Dankyi, Yvette Adu-Gyamfi. Telehealth during COVID-19 pandemic era: a systematic review[J]. AIMS Medical Science, 2022, 9(1): 81-97. doi: 10.3934/medsci.2022008
Across the globe, the coronavirus (COVID-19) pandemic has altered the delivery of healthcare services as patients must maintain their distance from caregivers, and still receive medical treatment. This has triggered a necessity for exploring means which minimizes the physical gap between patients and healthcare givers while offering health care and ensuring high medical protection at a reduced risk of exposure. Even though telehealth services are no replacement for conventional healthcare, its' usefulness in the coronavirus (COVID-19) pandemic is immense.
This research reviews the ardent utilization, barriers and recommendations with telehealth services for healthcare delivery during the COVID-19 pandemic.
An assessment of literature in five large digital databases; PubMed, Science Direct, Sage Pub, ProQuest, and Google Scholar was conducted. Inclusion criteria included studies defining telehealth/telemedicine, utilization, barriers and recommendations during the COVID-19 pandemic from January 2020 to July 2021, written in English and published in peer-reviewed journals. Two reviewers independently assessed search results, extracted data, and assessed the quality of the included studies. Narrative synthesis was undertaken to summarize and report the findings.
Overall, the study discoveries which are most commonly stated as impediments for telehealth services' full utilization between patients and physicians beyond the scope of typical medical confinement are: infrastructure and internet access (20.00%), data privacy and security (13.33%), digital literacy (13.33%), reimbursement and liability (10.00%), and clinician and patient's unwillingness (6.67%).
The intrusion of coronavirus has accelerated the transition to telehealth services in healthcare delivery, but it has also provided a unique chance to demonstrate the critical role that telehealth can play in ensuring that people of all races, ethnicities, and communities receive high-quality treatment (justice). Healthcare professionals should emphasize the effectiveness of telehealth services as an alternate healthcare delivery method in promoting healthcare to all populace.

| [1] |
Blandford A, Wesson J, Amalberti R, et al. (2020) Opportunities and challenges for telehealth within, and beyond, a pandemic. Lancet Glob Health 8: e1364-e1365. https://doi.org/10.1016/S2214-109X(20)30362-4 
|
| [2] |
Hoffman DA (2020) Increasing access to care: telehealth during COVID-19. J Law Biosci 7: lsaa043. https://doi.org/10.1093/jlb/lsaa043
|
| [3] |
Abdel-Wahab M, Rosenblatt E, Prajogi B, et al. (2020) Opportunities in telemedicine, lessons learned after COVID-19 and the way into the future. Int J Radiat Oncol Biol Phys 108: 438-443. https://doi.org/10.1016/j.ijrobp.2020.07.006
|
| [4] |
Barney A, Buckelew S, Mesheriakova V, et al. (2020) The COVID-19 pandemic and rapid implementation of adolescent and young adult telemedicine: challenges and opportunities for innovation. J Adolesc Health 67: 164-171. https://doi.org/10.1016/j.jadohealth.2020.05.006
|
| [5] |
Gajarawala SN, Pelkowski JN (2020) Telehealth benefits and barriers. J Nurse Pract 17: 218-221. https://doi.org/10.1016/j.nurpra.2020.09.013
|
| [6] | Zhai Y (2020) A call for addressing barriers to telemedicine: health disparities during the COVID-19 pandemic. Psychother Psychosom 4: 1-3. https://doi.org/10.1159/000509000 |
| [7] |
Al-Samarraie H, Ghazal S, Alzahrani AI, et al. (2020) Telemedicine in Middle Eastern countries: Progress, barriers, and policy recommendations. Int J Med Inform 141: 104232. https://doi.org/10.1016/j.ijmedinf.2020.104232
|
| [8] |
Bakshi S, Tandon U (2021) Understanding barriers of telemedicine adoption : a study in North India. Syst Res Behav Sci 39: 128-142. https://doi.org/10.1002/sres.2774
|
| [9] |
Jalali MS, Landman A, Gordon WJ (2021) Telemedicine, privacy, and information security in the age of COVID-19. J Am Med Inform Assoc 28: 671-672. https://doi.org/10.1093/jamia/ocaa310
|
| [10] |
Chowdhury SR, Sunna TC, Ahmed S (2021) Telemedicine is an important aspect of healthcare services amid COVID-19 outbreak: Its barriers in Bangladesh and strategies to overcome. Int J Health Plann Manage 36: 4-12. https://doi.org/10.1002/hpm.3064
|
| [11] |
Triana AJ, Gusdorf RE, Shah KP, et al. (2020) Technology literacy as a barrier to telehealth during COVID-19. Telemed J E Health 26: 1118-1119. https://doi.org/10.1089/tmj.2020.0155
|
| [12] |
Smith AC, Thomas E, Snoswell CL, et al. (2020) Telehealth for global emergencies: Implications for coronavirus disease 2019 (COVID-19). J Telemed Telecare 26: 309-313. https://doi.org/10.1177/1357633X20916567
|
| [13] |
Dubin JM, Wyant WA, Balaji NC, et al. (2020) Telemedicine usage among urologists during the COVID-19 pandemic: cross-sectional study. J Med Internet Res 22: e21875. https://doi.org/10.2196/21875
|
| [14] |
Ahmed S, Sanghvi K, Yeo D (2020) Telemedicine takes centre stage during COVID-19 pandemic. BMJ Innov 6: 252-254. https://doi.org/10.1136/bmjinnov-2020-000440
|
| [15] |
Monaghesh E, Hajizadeh A (2020) The role of telehealth during COVID-19 outbreak: a systematic review based on current evidence. BMC Public Health 20: 1193. https://doi.org/10.1186/s12889-020-09301-4
|
| [16] | Okereafor K, Adebola O, Djehaiche R (2020) Exploring the potentials of telemedicine and other non-contact electronic health technologies in controlling the spread of the novel coronavirus disease (COVID-19). IJMR 8: 1-13. |
| [17] |
Bokolo AJ (2021) Exploring the adoption of telemedicine and virtual software for care of outpatients during and after COVID-19 pandemic. Ir J Med Sci 190: 1-10. https://doi.org/10.1007/s11845-020-02299-z
|
| [18] | Burroughs M, Urits I, Viswanath O, et al. (2020) Benefits and shortcomings of utilizing telemedicine during the COVID-19 pandemic. Proc (Bayl Univ Med Cent) 33: 699-700. https://doi.org/10.1080/08998280.2020.1792728 |
| [19] | Nouri S, Khoong EC, Lyles CR, et al. (2020) Addressing equity in telemedicine for chronic disease management during the COVID-19 pandemic. NEJM Catalyst 1–13. https://doi.org/10.1056/CAT.20.0123 |
| [20] |
Ortega G, Rodriguez JA, Maurer LR, et al. (2020) Telemedicine, COVID-19, and disparities: Policy implications. Health Policy Technol 9: 368-371. https://doi.org/10.1016/j.hlpt.2020.08.001
|
| [21] |
Vidal-Alaball J, Acosta-Roja R, Pastor Hernández N, et al. (2020) Telemedicine in the face of the COVID-19 pandemic. Aten Primaria 52: 418-422. https://doi.org/10.1016/j.aprim.2020.04.003
|
| [22] | Oyediran KA, Makinde OA, Adelakin O (2020) The role of telemedicine in addressing access to sexual and reproductive health services in sub-Saharan Africa during the COVID-19 pandemic. Afr J Reprod Health 24: 49-55. https://doi.org/10.29063/ajrh2020/v24i2s.8 |
| [23] |
Wosik J, Fudim M, Cameron B, et al. (2020) Telehealth transformation: COVID-19 and the rise of virtual care. J Am Med Inform Assoc 27: 957-962. https://doi.org/10.1093/jamia/ocaa067
|
| [24] |
Ohannessian R, Duong TA, Odone A (2020) Global telemedicine implementation and integration within health systems to fight the COVID-19 pandemic: a call to action. JMIR Public Health Surveill 6: e18810. https://doi.org/10.2196/18810
|
| [25] | Nittas V, Von Wyl V (2020) COVID-19 and telehealth: a window of opportunity and its challenges. Swiss Med Wkly 150: w20284. https://doi.org/10.4414/smw.2020.20284 |
| [26] |
Gifford AH, Ong T, Dowd C, et al. (2020) Evaluating barriers to and promoters of telehealth during the COVID-19 pandemic at U.S. cystic fibrosis programs. J Cyst Fibros 20: 9-13. https://doi.org/10.1016/j.jcf.2021.08.034
|
| [27] |
Garfan S, Alamoodi AH, Zaidan BB, et al. (2021) Telehealth utilization during the COVID-19 pandemic: a systematic review. Comput Biol Med 138: 104878. https://doi.org/10.1016/j.compbiomed.2021.104878
|
| [28] |
Akintunde TY, Akintunde OD, Musa TH, et al. (2021) Expanding telemedicine to reduce the burden on the healthcare systems and poverty in Africa for a post-coronavirus disease 2019 (COVID-19) pandemic reformation. Glob Health J 5: 128-134. https://doi.org/10.1016/j.glohj.2021.07.006
|
| [29] |
Rozga M, Handu D, Kelley K, et al. (2021) Telehealth during the COVID-19 pandemic: a cross-sectional survey of registered dietitian nutritionists. J Acad Nutr Diet 121: 2524-2535. https://doi.org/10.1016/j.jand.2021.01.009
|
| [30] |
Cunningham NR, Ely SL, Garcia BNB, et al. (2021) Addressing pediatric mental health using telehealth during coronavirus disease-2019 and beyond: a narrative review. Acad Pediatr 21: 1108-1117. https://doi.org/10.1016/j.acap.2021.06.002
|


Figures(3) / Tables(4)

Jonathan Kissi, Daniel Kwame Kwansah Quansah, Jonathan Aseye Nutakor, Alex Boadi Dankyi, Yvette Adu-Gyamfi. Telehealth during COVID-19 pandemic era: a systematic review[J]. AIMS Medical Science, 2022, 9(1): 81-97. doi: 10.3934/medsci.2022008







 DownLoad:
DownLoad: