




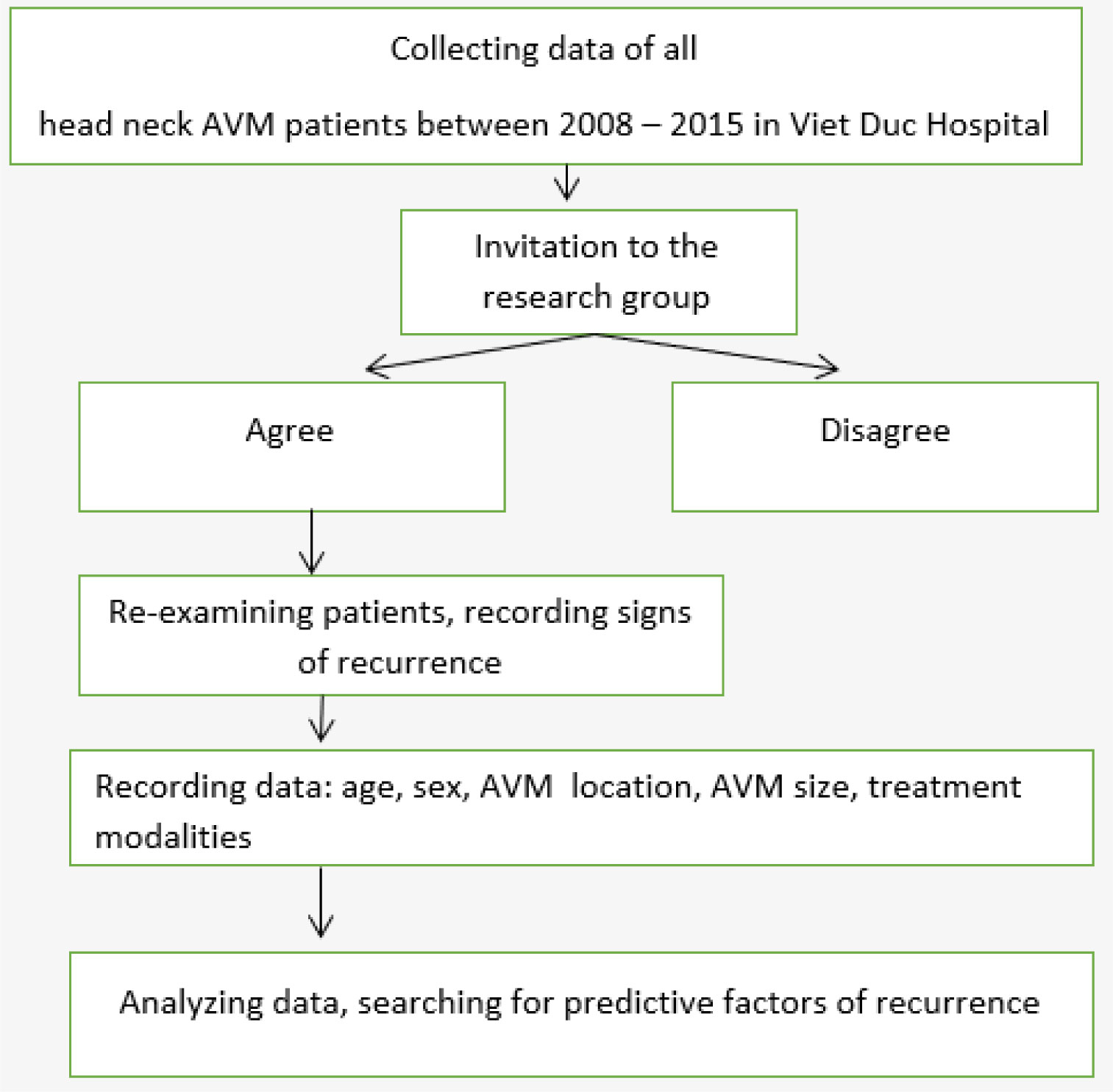
Figure 1.
Flow charts of the current study.
Arteriovenous malformations (AVMs) are aggressive diseases with a high tendency to recur. AVM treatment is complex, especially in the anatomically difficult head and neck region. This study analyzed correlations between extracranial head and neck AVM presentations and the frequency of recurrence.
We retrospectively assessed AVM recurrence among 55 patients with head and neck AVMs treated with embolization and resection between January 2008 and December 2015. Recurrence was defined as any evidence of AVM expansion following embolization and resection. Patient variables, including sex, age, AVM size, AVM location, stage, and treatment modalities, were examined for correlations with the recurrence of head and neck AVMs. Statistical analysis was performed using SPSS 20.0.
A total of 55 patients with at least 6 months of follow-up following AVM treatment with embolization and surgical resection were enrolled in this study. During follow-up, 14 of 55 patients experienced recurrence (the long-term recurrence rate was 25.5%). Sex, stage, AVM size, and treatment modality were identified as independent predictors of recurrence. Recurrence was less likely following the treatment of lower-stage or smaller lesions and did not correlate with age or location.
AVMs of the head and neck are among the most challenging conditions to manage due to a high risk of recurrence. Early and total AVM resection is the best method for preventing recurrence.
Citation: Do-Thi Ngoc Linh, Lam Khanh, Le Thanh Dung, Nguyen Hong Ha, Tran Thiet Son, Nguyen Minh Duc. Recurrence after treatment of arteriovenous malformations of the head and neck[J]. AIMS Medical Science, 2022, 9(1): 9-17. doi: 10.3934/medsci.2022003
| [1] | Gurpreet Singh, Demetrius K. Lopes, Neeraj Jolly . Neuro-endovascular Embolic Agent for Treatment of a Renal Arteriovenous Fistula. AIMS Medical Science, 2016, 3(1): 96-102. doi: 10.3934/medsci.2016.1.96 |
| [2] | Van Tuan Nguyen, Anh Tuan Tran, Nguyen Quyen Le, Thi Huong Nguyen . The features of computed tomography and digital subtraction angiography images of ruptured cerebral arteriovenous malformation. AIMS Medical Science, 2021, 8(2): 105-115. doi: 10.3934/medsci.2021011 |
| [3] | Vivek Radhakrishnan, Mark S. Swanson, Uttam K. Sinha . Monoclonal Antibodies as Treatment Modalities in Head and Neck Cancers. AIMS Medical Science, 2015, 2(4): 347-359. doi: 10.3934/medsci.2015.4.347 |
| [4] | Renjith Parameswaran Nair, Gulshan Sunavala-Dossabhoy . Promising Gene Therapeutics for Salivary Gland Radiotoxicity. AIMS Medical Science, 2016, 3(4): 329-344. doi: 10.3934/medsci.2016.4.329 |
| [5] | Divya Seth, Deepak Kamat . Anaphylaxis: recognition, treatment, and outcomes. AIMS Medical Science, 2022, 9(1): 65-80. doi: 10.3934/medsci.2022007 |
| [6] | Charing Ching-Ning Chong, Grace Lai-Hung Wong . Treatments of Hepatocellular Carcinoma Patients with Hepatitis B Virus Infection: Treat HBV-related HCC. AIMS Medical Science, 2016, 3(1): 162-178. doi: 10.3934/medsci.2016.1.162 |
| [7] | Magaisha Edward Kyomo, Nelson Mpumi, Elingarami Sauli, Salum J Lidenge . Efficiency of honey–grape blend in reducing radiation-induced mucositis in locally advanced head and neck squamous cell carcinoma. AIMS Medical Science, 2025, 12(1): 90-104. doi: 10.3934/medsci.2025007 |
| [8] | Elzbieta Marczak, Maria Szarras-Czapnik, Elzbieta Moszczyńska . Endocrine manifestations in Joubert syndrome—literature review. AIMS Medical Science, 2023, 10(4): 343-352. doi: 10.3934/medsci.2023027 |
| [9] | Turki M. Bin Mahfoz, Ahmad K. Alnemare . Optic neuropathy related to Onodi cell mucocele: a systematic review and meta-analysis of randomized controlled trials. AIMS Medical Science, 2021, 8(3): 203-223. doi: 10.3934/medsci.2021018 |
| [10] | Fauwaz Fahad Alrashid, Saadeldin Ahmed Idris, Abdul Ghani Qureshi . Current trends in the management of pilonidal sinus disease and its outcome in a periphery hospital. AIMS Medical Science, 2021, 8(1): 70-79. doi: 10.3934/medsci.2021008 |
Arteriovenous malformations (AVMs) are aggressive diseases with a high tendency to recur. AVM treatment is complex, especially in the anatomically difficult head and neck region. This study analyzed correlations between extracranial head and neck AVM presentations and the frequency of recurrence.
We retrospectively assessed AVM recurrence among 55 patients with head and neck AVMs treated with embolization and resection between January 2008 and December 2015. Recurrence was defined as any evidence of AVM expansion following embolization and resection. Patient variables, including sex, age, AVM size, AVM location, stage, and treatment modalities, were examined for correlations with the recurrence of head and neck AVMs. Statistical analysis was performed using SPSS 20.0.
A total of 55 patients with at least 6 months of follow-up following AVM treatment with embolization and surgical resection were enrolled in this study. During follow-up, 14 of 55 patients experienced recurrence (the long-term recurrence rate was 25.5%). Sex, stage, AVM size, and treatment modality were identified as independent predictors of recurrence. Recurrence was less likely following the treatment of lower-stage or smaller lesions and did not correlate with age or location.
AVMs of the head and neck are among the most challenging conditions to manage due to a high risk of recurrence. Early and total AVM resection is the best method for preventing recurrence.
Arteriovenous malformations (AVMs) are fast-flow vascular malformations comprised of complex networks of primitive vessels directly connecting feeding arteries to draining veins and lacking a normal capillary network [1]; the area containing the abnormal vasculature and shunting is referred to as the nidus.
The behavior of extracranial AVMs is locally aggressive. As AVMs progress, they destroy normal tissues, eventually leading to complications, such as severe disfigurement, uncontrollable bleeding, ulceration, pain, and cardiac volume overload. The only currently available curative AVM treatment is complete removal or ablation of the nidus, with complete radical resection representing the recommended surgical treatment [2]–[4]. The radical resection of a AVM mass can be very difficult, resulting in disfigurement and functional damage, particularly in the head and neck region, where AVMs commonly occur. Completely improved outcome was observed in only 35–60% of patients treated at the hospital [5]. In addition, there is a high chance of recurrence or progression of AVMs, even after treatment: Recurrence rates of over 80% after embolization and surgical resection have been reported [6], although recent advances and improved multidisciplinary care approaches may result in future improvements. Recurrent mechanisms were explained by some hypotheses such as hypoxia, trauma, inflammation, even embolic and surgical treatments. The aim of the present study was to identify correlations between patterns of extracranial head and neck AVM presentations and the frequency of recurrence.
This retrospective study was approved by the Ethics Committee of Hanoi Medical University (20NCS17/HMU IRB). Informed consent from patients was obtained or waived. Flow chart of this study was introduced in Figure 1.
We reviewed all patients with head and neck AVMs who were treated by the Department of Maxillofacial and Plastic Surgery, Viet Duc Hospital, between January 2008 and December 2015. Using chart review, we recorded the location, clinical symptoms, clinical stage according to the Schöbinger staging system (Table 1), and treatment modalities applied to each AVM case.
To determine clinical or imaging indications of recurrence after treatment, we reviewed all documents associated with all follow-up clinical appointments and reports associated with any post-treatment Doppler ultrasound, magnetic resonance imaging (MRI), or digital subtraction angiography (DSA) studies.
We considered the reappearance of a mass, pulsation, or both, to represent a clinical sign of recurrence. The reappearance of a mass, flow voids, or both (on MRI), or any indication of arteriovenous shunting (DSA or Doppler ultrasound) were recorded as imaging signs of recurrence.
Age, sex, AVM location, AVM size, and treatment modalities were recorded to determine whether any of these variables were predictive factors for AVM recurrence.
| Stage | Features |
| Stage I (Quiescence) | Skin warmth, discoloration |
| Stage II (Expansion) | Enlargement, pulsation, bruit, thrill |
| Stage III (Destruction) | Pain, ulceration, bleeding |
| Stage IV (Decompensation) | Cardiac failure due to volume overload |
 DownLoad:
CSV
DownLoad:
CSV
Data were analyzed using SPSS v.20.0. Data are presented as the mean with 95 percent confidence intervals or standard deviation. Proportions were compared using Chi-square analysis and Fisher's exact test. Two-tailed values of p < 0.05 were considered significant.
A total of 55 patients met the selection criteria and were enrolled in the study. The mean age at the time of treatment was 29.9 ± 12.73 years (range: 3–67 years). The male to female ratio was 2 to 1. The Schöbinger stage was II in 38 patients and III in 17 patients. No patients were classified as Schöbinger stages I or IV (Table 2).
All patients were treated using a combination of embolization and surgical resection (Figures 2 and 3).
N-butyl-2-cyanoacrylate (NBCA) was typically used to embolize the nidus. In complicated cases, other agents were also used, including polyvinyl alcohol (PVA), Amplatzer, coils, and gelatin sponge plugs. Superselective intra-arterial embolization (SIAE) was performed in 30 patients (54.5%); direct puncture into the nidus was performed in 25 patients, either alone or combined with SIAE.
Total resection of the nidus was performed in 50 patients, whereas the remaining 5 patients presented with large and diffuse AVMs that could not be totally removed. To cover defects following resection, direct closure was applied in 41 patients. Skin grafts were required in 5 patients, local flaps were used in 11 patients, and a distal flap was used in 1 patient. No patients were treated using free flaps.
AVM recurrence following treatment was documented in 25.5% of patients during an average follow-up time of 3.5 ± 2.02 years.
Multivariate analysis showed that age (p = 0.703) and AVM location (p = 0.32) were not correlated with recurrence. By contrast, sex (p = 0.045), Schöbinger stage (p = 0.005), AVM size (p = 0.026), and treatment modality (p = 0.001) were independent predictors of recurrence. Patients managed by total resection had the lowest recurrence rate compared with patients who were managed by subtotal resection.


| Recurrence | Total | Rate (%) | p | ||
| Sex | Male | 6 | 37 | 16.2 | 0.045 |
| Female | 8 | 18 | 44.4 | ||
| Age (y) | ≤18 | 3 | 10 | 30 | 0.703 |
| >18 | 11 | 45 | 24.4 | ||
| Size (cm) | <5 | 2 | 23 | 8.7 | 0.026 |
| ≥5 | 12 | 32 | 37.5 | ||
| Location | Scalp | 1 | 12 | 8.3 | 0.32 |
| Mouth floor | 1 | 2 | 50 | ||
| Ear | 8 | 14 | 57.1 | ||
| Cheek | 4 | 12 | 33.3 | ||
| Stage | Stage II | 5 | 38 | 11.4 | 0.005 |
| Stage III | 9 | 17 | 52.9 | ||
| Treatment modality | Total resection | 9 | 50 | 18 | 0.001 |
| Partial resection | 5 | 5 | 100 |
DownLoad:
CSV
Current management of AVMs generally involves close observation, surgical excision, intravascular embolization, or some combination of these treatment modalities. Extracranial head and neck AVM are a locally aggressive lesion located in a complex anatomical region, associated with a high recurrence rate after intervention [2],[8]. The pathogenesis of head and neck AVMs remains unclear [1],[9]–[12].
In a series of 272 patients with head and neck AVMs reported by Liu et al., which underscored the difficulty of achieving a long-term cure for peripheral AVM, the reported recurrence rates after surgical resection were 81% for head AVMs and 98% for neck AVMs after embolization [5]. In a series of 81 patients, Kohout et al. reported an overall cure rate of 60% [5]. In our series, the recurrence rate was 25.5%, which may be associated with the shorter follow-up for our study, which averaged only 3.5 years compared with 4.6 years reported by Liu et al. study and 12.7 years reported by Kohout et al. According to Fernández-Alvarez and Richter, recurrence can occur as long as 10 years after treatment [13],[14].
Koshima, Pekkola, Kohout and some other authors have suggested that recurrence mechanisms include a proangiogenic environment involving hypoxia, trauma, and inflammation, embolic and surgical treatments which can support the continued development of any remaining nidus remnant, leading to recurrence, often with a complex architecture and extensive vascular recruitment [2],[5],[12],[15].
Our results suggest that early and total nidus resection can reduce the risk of recurrence. Richter and Suen also supposed that vigilant observation, early treatment, and radical therapy are necessary for AVMs of the head and neck [14]. However, total resection is not always easy or possible, particularly for large and diffuse lesions in the head and neck region [1],[16],[17]. We postulate that the use of a pedicled or free flap to cover the tissue defect after resection may minimize AVM recurrence by reducing tissue hypoxia [15].
In our series, the 55 patients with head and neck AVMs were categorized as Schöbinger stages II or III, and 8 of 18 female patients experienced recurrence (44.4%), which was a significantly higher rate than observed in male patients (16.2%; p = 0.024). This finding differs from that reported by Liu et al., for which the recurrence rate was not correlated with sex [6]. In our study group, 2 of the patients who experienced recurrence were pregnant. Some authors [9],[18] believe that pregnancy or puberty may increase the risk of progression because hormonal changes associated with these periods may stimulate AVMs by promoting angiogenesis. However, in quiescent lesions (stage I), Liu et al. did not find progression in pregnant women [6]. The rate of recurrence was 30% (n = 3) among the younger group and 24.4% (n = 11) among the adult group, which was not significantly different.
Of the 14 patients who had auricular AVMs, 8 patients experienced recurrence, which may be due to the surgical treatment, as some patients (n = 10; 71.4%) were not prepared to undergo auricular resection and preferentially chose embolization and partial nidus resection. However, this recurrence rate was not significantly higher than that for other AVM locations (p = 0.32). In the series of 41 patients with auricular AVMs (Wu et al.), 20 patients (48.78%) had recurrence after mean time of 5.19 years follow-up. The high rate of recurrence in auricular region might be explained by patients' desire of auricular conservation at the lower-staged and the recurrent tendency after treatment at higher-staged AVMs. According to Lu et al., higher-staged AVMs exhibit increased expression of endothelial progenitor cells and factors that stimulate their recruitment [18].
Although the pathology underlying AVM development remains unclear, Lu and Colletti postulated that pharmacotherapy may be able to control the re-expansion and recurrence through the inhibition of vascular endothelial growth factor and angiopoietin 2, which have been detected in AVM tissue [18],[19].
The management of AVMs that occur in the head and neck region is challenging and requires a multidisciplinary approach. The rate of recurrence after treatment is high, particularly for diffuse AVMs. Sex, stage, and AVM size, in addition to the treatment modality, were predictive factors for recurrence. Early treatment allowing for total AVM resection is the optimal approach for preventing recurrence.
| [1] |
Uller W, Alomari AI, Richter GT (2014) Arteriovenous malformation. Semin Pediatr Surg 23: 203-207. https://doi.org/10.1053/j.sempedsurg.2014.07.005 
|
| [2] |
Pekkola J, Lappalainen K, Vuola P, et al. (2013) Head and neck arteriovenous malformations: Results of ethanol sclerotherapy. American J Neuroradiol 34: 198-204. http://doi.org:10.3174/ajnr.A3180
|
| [3] |
Mulliken JB, Fishman SJ, Burrows PE (2000) Vascular anomalies. Curr Probl Surg 37: 517-584. https://doi.org/10.1016/S0011-3840(00)80013-1
|
| [4] |
Mulliken JB, Burrows PE, Fishman SJ (2013) Mulliken and Young's vascular anomalies: Hemangiomas and malformations.Oxford University Press. https://doi.org/10.1093/med/9780195145052.001.0001
|
| [5] |
Kohout MP, Hansen M, Pribaz JJ, et al. (1998) Arteriovenous malformations of the head and neck: natural history and management. Plast Reconstr Surg 102: 643-654. https://doi.org/10.1097/00006534-199809010-00006
|
| [6] |
Liu AS, Mulliken JB, Zurakowski D, et al. (2010) Extracranial arteriovenous malformations: natural progression and recurrence after treatment. Plast Reconstr Surg 125: 1185-1194. https://doi.org/10.1097/PRS.0b013e3181d18070
|
| [7] |
Wu JK, Bisdorff A, Gelbert F, et al. (2005) Auricular arteriovenous malformation: evaluation, management, and outcome. Plast Reconstr Surg 115: 985-995. https://doi.org/10.1097/01.PRS.0000154207.87313
|
| [8] |
Lee BB, Do YS, Yakes W, et al. (2004) Management of arteriovenous malformations: a multidisciplinary approach. J Vasc Surg 39: 590-600. https://doi.org/10.1016/j.jvs.2003.10.048
|
| [9] |
Richter GT, Suen JY (2010) Clinical course of arteriovenous malformations of the head and neck: a case series. Otolaryngol Head Neck Surg 142: 184-190. https://doi.org/10.1016/j.otohns.2009.10.023
|
| [10] |
Rosenberg TL, Suen JY, Richter GT (2018) Arteriovenous malformations of the head and neck. Otolaryngol Clin North Am 51: 185-195. https://doi.org/10.1016/j.otc.2017.09.005
|
| [11] |
Jeong HS, Baek CH, Son YI, et al. (2006) Treatment for extracranial arteriovenous malformation of the head and neck. Acta Otolaryngol 126: 295-300. https://doi.org/10.1080/00016480500388950
|
| [12] |
Kim JY, Kim DI, Do YS, et al. (2006) Surgical treatment for congenital arteriovenous malformation: 10 years' experience. Eur J Vasc Endovasc Surg 32: 101-106. https://doi.org/10.1016/j.ejvs.2006.01.004
|
| [13] |
Fernández-Alvarez V, Suárez C, De Bree R, et al. (2020) Management of extracranial arteriovenous malformations of the head and neck. Auris Nasus Larynx 47: 181-190. https://doi.org/10.1016/j.anl.2019.11.008
|
| [14] |
Richter GT, Suen JY (2011) Pediatric extracranial arteriovenous malformations. Curr Opin Otolaryngol Head Neck Surg 19: 455-461. https://doi.org/10.1097/MOO.0b013e32834cd57c
|
| [15] |
Koshima I, Nanba Y, Tsutsui T, et al. (2003) Free perforator flap for the treatment of defects after resection of huge arteriovenous malformations in the head and neck regions. Ann Plast Surg 51: 194-199. https://doi.org/10.1097/01.SAP.0000044706.58478.73
|
| [16] |
Fowell C, Jones R, Nishikawa H, et al. (2016) Arteriovenous malformations of the head and neck: current concepts in management. Br J Oral Maxillofac Surg 54: 482-487. https://doi.org/10.1016/j.bjoms.2016.01.034
|
| [17] |
Greene AK, Orbach DB (2011) Management of arteriovenous malformations. Clin Plast Surg 38: 95-106. https://doi.org/10.1016/j.cps.2010.08.005
|
| [18] |
Lu L, Bischoff J, Mulliken JB, et al. (2011) Progression of arteriovenous malformation: possible role of vasculogenesis. Plast Reconstr Surg 128: 260e-269e. https://doi.org/10.1097/PRS.0b013e3182268afd
|
| [19] |
Colletti G, Dalmonte P, Moneghini L, et al. (2015) Adjuvant role of anti-angiogenic drugs in the management of head and neck arteriovenous malformations. Med Hypotheses 85: 298-302. https://doi.org/10.1016/j.mehy.2015.05.016
|

Do-Thi Ngoc Linh, Lam Khanh, Le Thanh Dung, Nguyen Hong Ha, Tran Thiet Son, Nguyen Minh Duc. Recurrence after treatment of arteriovenous malformations of the head and neck[J]. AIMS Medical Science, 2022, 9(1): 9-17. doi: 10.3934/medsci.2022003

| Stage | Features |
| Stage I (Quiescence) | Skin warmth, discoloration |
| Stage II (Expansion) | Enlargement, pulsation, bruit, thrill |
| Stage III (Destruction) | Pain, ulceration, bleeding |
| Stage IV (Decompensation) | Cardiac failure due to volume overload |
DownLoad:
CSV
| Recurrence | Total | Rate (%) | p | ||
| Sex | Male | 6 | 37 | 16.2 | 0.045 |
| Female | 8 | 18 | 44.4 | ||
| Age (y) | ≤18 | 3 | 10 | 30 | 0.703 |
| >18 | 11 | 45 | 24.4 | ||
| Size (cm) | <5 | 2 | 23 | 8.7 | 0.026 |
| ≥5 | 12 | 32 | 37.5 | ||
| Location | Scalp | 1 | 12 | 8.3 | 0.32 |
| Mouth floor | 1 | 2 | 50 | ||
| Ear | 8 | 14 | 57.1 | ||
| Cheek | 4 | 12 | 33.3 | ||
| Stage | Stage II | 5 | 38 | 11.4 | 0.005 |
| Stage III | 9 | 17 | 52.9 | ||
| Treatment modality | Total resection | 9 | 50 | 18 | 0.001 |
| Partial resection | 5 | 5 | 100 |
DownLoad:
CSV
| Stage | Features |
| Stage I (Quiescence) | Skin warmth, discoloration |
| Stage II (Expansion) | Enlargement, pulsation, bruit, thrill |
| Stage III (Destruction) | Pain, ulceration, bleeding |
| Stage IV (Decompensation) | Cardiac failure due to volume overload |
| Recurrence | Total | Rate (%) | p | ||
| Sex | Male | 6 | 37 | 16.2 | 0.045 |
| Female | 8 | 18 | 44.4 | ||
| Age (y) | ≤18 | 3 | 10 | 30 | 0.703 |
| >18 | 11 | 45 | 24.4 | ||
| Size (cm) | <5 | 2 | 23 | 8.7 | 0.026 |
| ≥5 | 12 | 32 | 37.5 | ||
| Location | Scalp | 1 | 12 | 8.3 | 0.32 |
| Mouth floor | 1 | 2 | 50 | ||
| Ear | 8 | 14 | 57.1 | ||
| Cheek | 4 | 12 | 33.3 | ||
| Stage | Stage II | 5 | 38 | 11.4 | 0.005 |
| Stage III | 9 | 17 | 52.9 | ||
| Treatment modality | Total resection | 9 | 50 | 18 | 0.001 |
| Partial resection | 5 | 5 | 100 |
