This study assessed the efficacy of a honey–grape blend in reducing the severity and onset of radiation oral mucositis (ROM) in patients with locally advanced squamous cell carcinoma of the head and neck. Oral mucositis is an acute side effect caused by chemotherapy or radiotherapy in the head and neck region. ROM affects patients' quality of life and treatment expenses. Various pharmaceutical and natural remedies, such as sucralfate, aloe vera, and amifostine are used to mitigate the effects of ROM. However, the available modalities' efficacy is low and is associated with many side effects.
This cohort study was conducted at the Ocean Road Cancer Institute and Besta Polyclinic in Tanzania. The study included 73 patients with locally advanced squamous cell carcinoma of the head and neck treated from March 2024 to August 2024. The World Health Organization mucositis grading system was used to assess patients' progress weekly. Data analysis was conducted using Statistical Package for Social Science (SPSS) version 27.
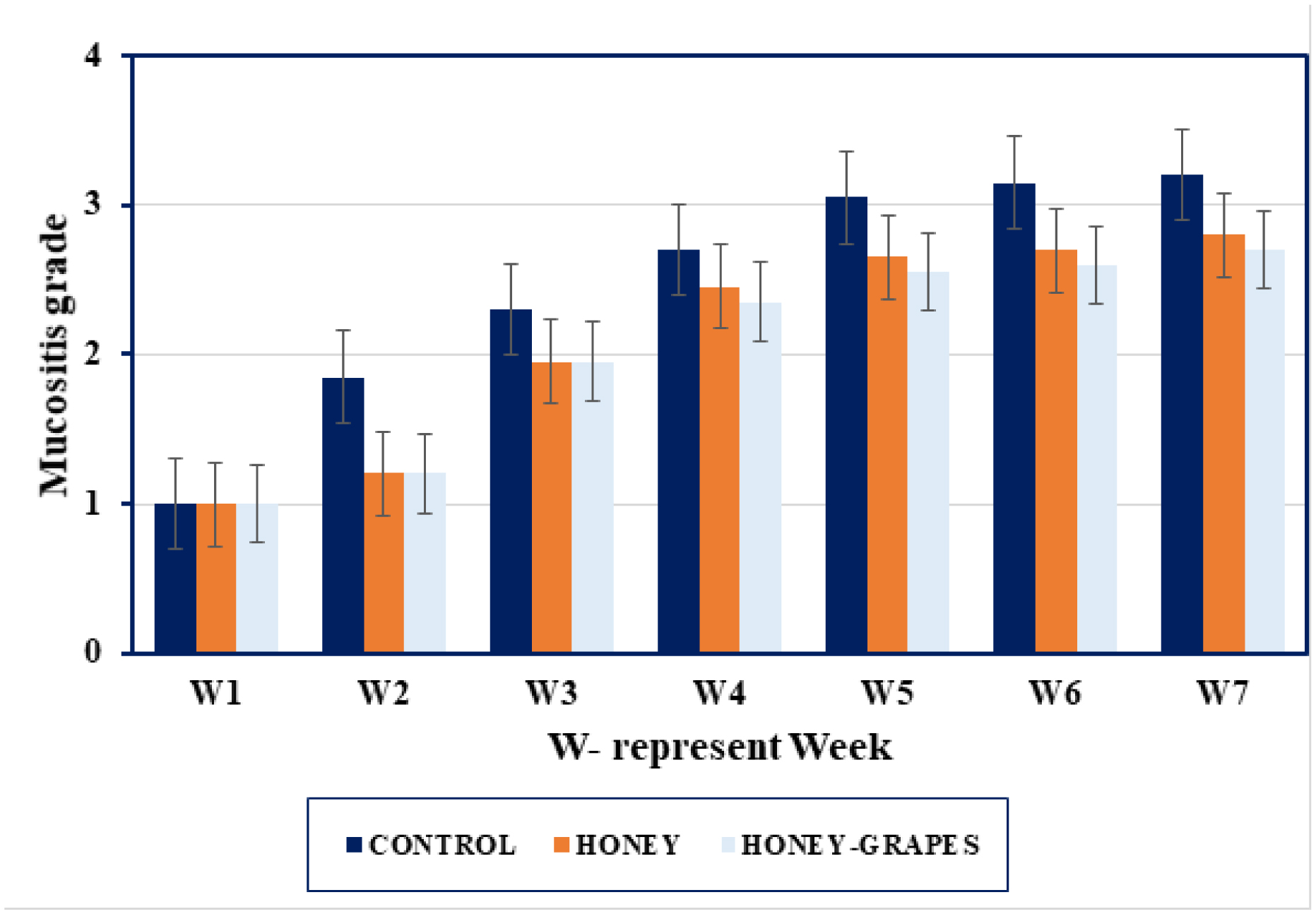
Delayed onset (15% Grade 3 for the honey–grape group and 45% Grade 3 for the control group at 28 days) and reduced the severity of ROM (only 20% Grade 3 with no Grade 4 for the honey–grape group while for the control group, it was 25% Grade 3 and 20% Grade 4 at 45 days) (p-value < 0.001). Body weight changes at starting and after completion of radiotherapy were observed (2.65 kg average weight loss for the control group and 1.8 kg, 0.45 kg weight gain for the honey group and honey–grape blend group). Prevalence between genders was 62% males and 38% females.
Honey and honey blended with grapes can minimize the severity and delay the onset of ROM in patients with locally advanced head and neck cancer. More studies are needed, since no study has been conducted addressing the efficacy of honey–grape blends in reducing ROM severity.
Citation: Magaisha Edward Kyomo, Nelson Mpumi, Elingarami Sauli, Salum J Lidenge. Efficiency of honey–grape blend in reducing radiation-induced mucositis in locally advanced head and neck squamous cell carcinoma[J]. AIMS Medical Science, 2025, 12(1): 90-104. doi: 10.3934/medsci.2025007
This study assessed the efficacy of a honey–grape blend in reducing the severity and onset of radiation oral mucositis (ROM) in patients with locally advanced squamous cell carcinoma of the head and neck. Oral mucositis is an acute side effect caused by chemotherapy or radiotherapy in the head and neck region. ROM affects patients' quality of life and treatment expenses. Various pharmaceutical and natural remedies, such as sucralfate, aloe vera, and amifostine are used to mitigate the effects of ROM. However, the available modalities' efficacy is low and is associated with many side effects.
This cohort study was conducted at the Ocean Road Cancer Institute and Besta Polyclinic in Tanzania. The study included 73 patients with locally advanced squamous cell carcinoma of the head and neck treated from March 2024 to August 2024. The World Health Organization mucositis grading system was used to assess patients' progress weekly. Data analysis was conducted using Statistical Package for Social Science (SPSS) version 27.
Delayed onset (15% Grade 3 for the honey–grape group and 45% Grade 3 for the control group at 28 days) and reduced the severity of ROM (only 20% Grade 3 with no Grade 4 for the honey–grape group while for the control group, it was 25% Grade 3 and 20% Grade 4 at 45 days) (p-value < 0.001). Body weight changes at starting and after completion of radiotherapy were observed (2.65 kg average weight loss for the control group and 1.8 kg, 0.45 kg weight gain for the honey group and honey–grape blend group). Prevalence between genders was 62% males and 38% females.
Honey and honey blended with grapes can minimize the severity and delay the onset of ROM in patients with locally advanced head and neck cancer. More studies are needed, since no study has been conducted addressing the efficacy of honey–grape blends in reducing ROM severity.

| [1] |
Machiels JP, René Leemans C, Golusinski W, et al. (2020) Squamous cell carcinoma of the oral cavity, larynx, oropharynx and hypopharynx: EHNS–ESMO–ESTRO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol 31: 1462-1475. https://doi.org/10.1016/j.annonc.2020.07.011 
|
| [2] |
Tsao SW, Yip YL, Tsang CM, et al. (2014) Etiological factors of nasopharyngeal carcinoma. Oral Oncol 50: 330-338. https://doi.org/10.1016/j.oraloncology.2014.02.006
|
| [3] | Akhtar A, Hussain I, Talha M, et al. (2016) Prevalence and diagnostic of head and neck cancer in Pakistan. Pak J Pharm Sci 29: 1839-1846. |
| [4] |
Iorio GC, Arcadipane F, Martini S, et al. (2021) Decreasing treatment burden in HPV-related OPSCC: a systematic review of clinical trials. Crit Rev Oncol Hematol 160: 103243. https://doi.org/10.1016/j.critrevonc.2021.103243
|
| [5] |
Liu TM, Luo YW, Tam KW, et al. (2019) Prophylactic and therapeutic effects of honey on radiochemotherapy-induced mucositis: a meta-analysis of randomized controlled trials. Support Care Cancer 27: 2361-2370. https://doi.org/10.1007/s00520-019-04722-3
|
| [6] |
Sonis ST (2021) A hypothesis for the pathogenesis of radiation-induced oral mucositis: when biological challenges exceed physiologic protective mechanisms. Implications for pharmacological prevention and treatment. Support Care Cancer 29: 4939-4947. https://doi.org/10.1007/s00520-021-06108-w
|
| [7] |
Soutome S, Yanamoto S, Nishii M, et al. (2021) Risk factors for severe radiation-induced oral mucositis in patients with oral cancer. J Dent Sci 16: 1241-1246. https://doi.org/10.1016/j.jds.2021.01.009
|
| [8] |
Maria OM, Eliopoulos N, Muanza T (2017) Radiation-induced oral mucositis. Front Oncol 7: 89. https://doi.org/10.3389/fonc.2017.00089
|
| [9] |
Lorini L, Perri F, Vecchio S, et al. (2022) Confounding factors in the assessment of oral mucositis in head and neck cancer. Support Care Cancer 30: 8455-8463. https://doi.org/10.1007/s00520-022-07128-w
|
| [10] |
Li J, Zhu C, Zhang Y, et al. (2023) Incidence and risk factors for radiotherapy-induced oral mucositis among patients with nasopharyngeal carcinoma: a meta-analysis. Asian Nurs Res 17: 70-82. https://doi.org/10.1016/j.anr.2023.04.002
|
| [11] |
Singh V, Singh AK (2020) Oral mucositis. Natl J Maxillofac Surg 11: 159-168. https://doi.org/10.4103/njms.NJMS_10_20
|
| [12] |
Chandra VC, Nur'aeny N, Wahyuni IS (2022) Anti-inflammatory potential of aloe vera in oral mucositis therapy: systematic review. Int J Appl Pharm 14: 22-27. https://doi.org/10.22159/ijap.2022.v14ti.21
|
| [13] |
Jayachandran S, Balaji N (2012) Evaluating the effectiveness of topical application of natural honey and benzydamine hydrochloride in the management of radiation mucositis. Indian J Palliat Care 18: 190-195. https://doi.org/10.4103/0973-1075.105689
|
| [14] |
Zhang X, Sun D, Qin N, et al. (2020) Comparative prevention potential of 10 mouthwashes on intolerable oral mucositis in cancer patients: a Bayesian network analysis. Oral Oncol 107: 104751. https://doi.org/10.1016/j.oraloncology.2020.104751
|
| [15] | Abeshu MA, Geleta B (2016) Medicinal uses of honey. Biol Med 8. https://doi.org/10.4172/0974-8369.1000276 |
| [16] |
Ribeiro Paiotti AP, Neto RA, Marchi P, et al. (2013) The anti-inflammatory potential of phenolic compounds in grape juice concentrate (G8000™) on 2,4,6-trinitrobenzene sulphonic acid-induced colitis. Br J Nutr 110: 973-980. https://doi.org/10.1017/S000711451300007X
|
| [17] | Ghasemzadeh A, Ghasemzadeh N (2011) Flavonoids and phenolic acids: role and biochemical activity in plants and human. J Med Plants Res 5: 6697-6703. https://doi.org/10.5897/JMPR11.1404 |
| [18] |
Chatterjee A (2013) Reduced glutathione: a radioprotector or a modulator of DNA-repair activity?. Nutrients 5: 525-542. https://doi.org/10.3390/nu5020525
|
| [19] |
Eslami H, Jamali Z, Babaei H, et al. (2022) Evaluation of the Effect of Grape Seed Extract (GSE) on oral mucositis in patients with head and neck radiotherapy history—a randomized clinical trial. Int J Cancer Manag 15: e130603. https://doi.org/10.5812/ijcm-130603
|
| [20] |
Afrasiabifar A, Dehkordi NJ, Mosavi A, et al. (2020) Oral mucositis: examining the combined solution of grape vinegar and rose water versus chlorhexidine mouthwash. Clin J Oncol Nurs 24: E71-E78. https://doi.org/10.1188/20.CJON.E71-E78
|
| [21] |
Yuce Sari S, Beduk Esen CS, Yazici G, et al. (2022) Do grape and black mulberry molasses have an effect on oral mucositis and quality of life in patients with head and neck cancer?. Support Care Cancer 30: 327-336. https://doi.org/10.1007/s00520-021-06411-6
|
| [22] | Bogdanov S (2016) Honey as nutrient and functional food. Available from: https://www.researchgate.net/publication/304011789_Honey_as_Nutrient_and_Functional_Food |
| [23] |
Mcgill CR, Keast DR, Painter JE, et al. (2013) Improved diet quality and increased nutrient intakes associated with grape product consumption by U.S. children and adults: national health and nutrition examination survey 2003 to 2008. J Food Sci 78: A1-A4. https://doi.org/10.1111/1750-3841.12066
|
| [24] |
de Sanctis V, Belgioia L, Cante D, et al. (2019) Lactobacillus brevis CD2 for prevention of oral mucositis in patients with head and neck tumors: a multicentric randomized study. Anticancer Res 39: 1935-1942. https://doi.org/10.21873/anticanres.13303
|
| [25] |
Sunaga T, Nagatani A, Fujii N, et al. (2021) The association between cumulative radiation dose and the incidence of severe oral mucositis in head and neck cancers during radiotherapy. Cancer Rep 4: e1317. https://doi.org/10.1002/cnr2.1317
|
| [26] |
Ingrosso G, Saldi S, Marani S, et al. (2021) Breakdown of symbiosis in radiation-induced oral mucositis. J Fungi 7: 290. https://doi.org/10.3390/jof7040290
|
| [27] |
Vera-Llonch M, Oster G, Hagiwara M, et al. (2006) Oral mucositis in patients undergoing radiation treatment for head and neck carcinoma: risk factors and clinical consequences. Cancer 106: 329-336. https://doi.org/10.1002/cncr.21622
|
| [28] |
Khanal B, Baliga M, Uppal N (2010) Effect of topical honey on limitation of radiation-induced oral mucositis: an intervention study. Int J Oral Maxillofac Surg 39: 1181-1185. https://doi.org/10.1016/j.ijom.2010.05.014
|
Figures(1) / Tables(8)

Magaisha Edward Kyomo, Nelson Mpumi, Elingarami Sauli, Salum J Lidenge. Efficiency of honey–grape blend in reducing radiation-induced mucositis in locally advanced head and neck squamous cell carcinoma[J]. AIMS Medical Science, 2025, 12(1): 90-104. doi: 10.3934/medsci.2025007







 DownLoad:
DownLoad: