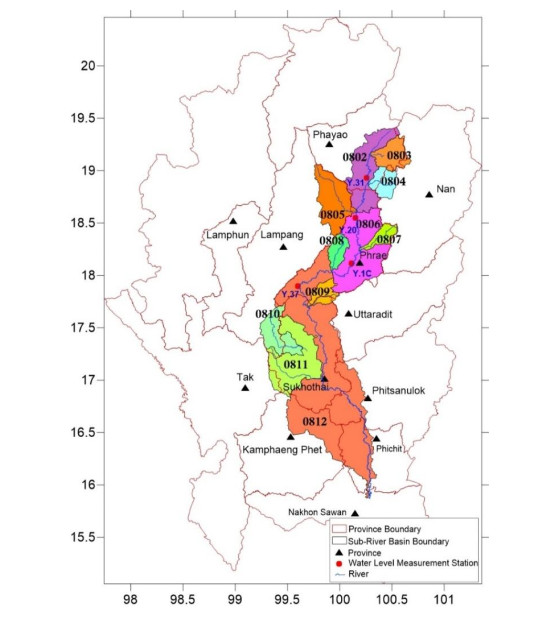
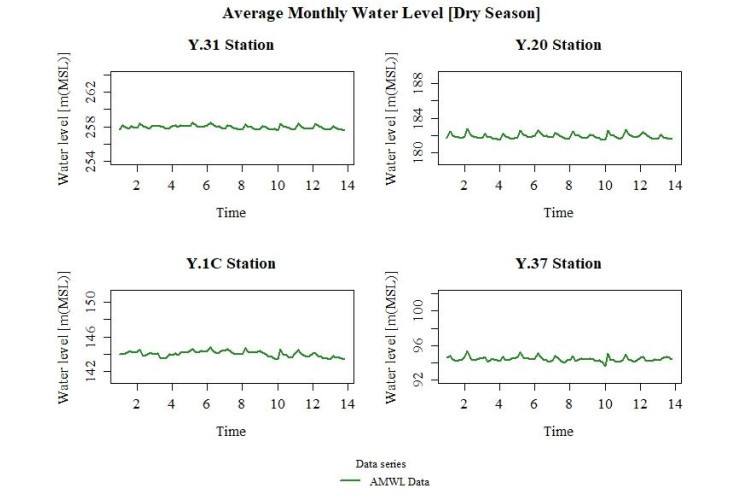
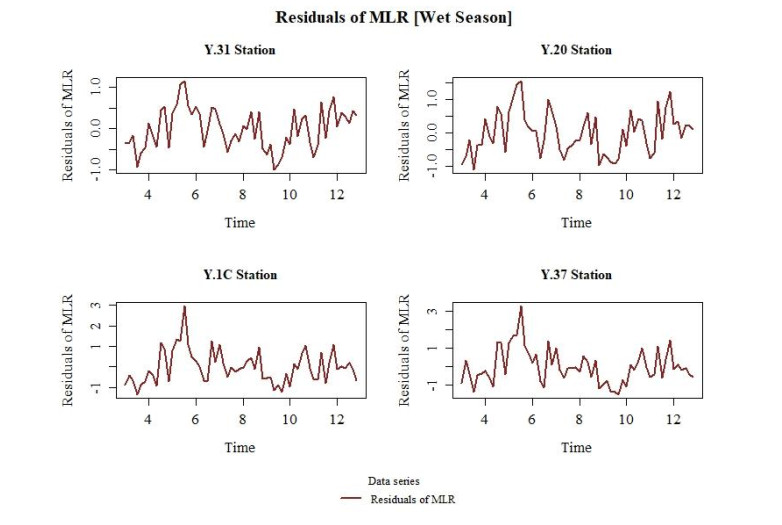
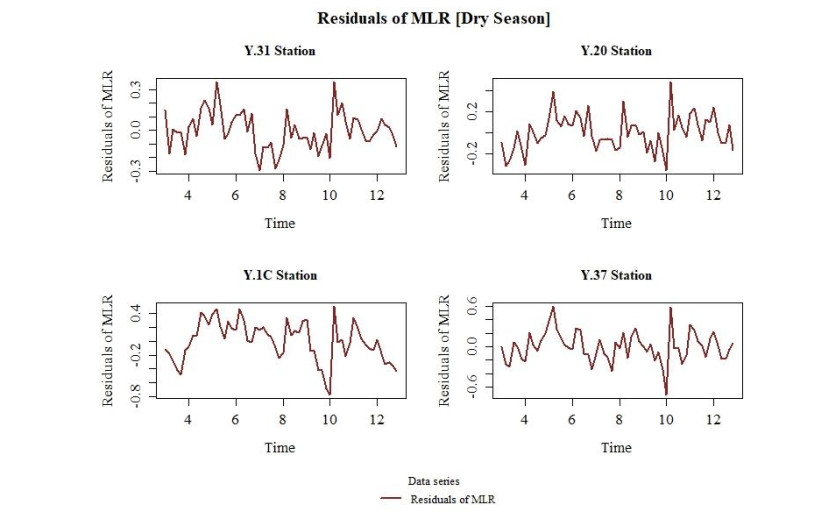
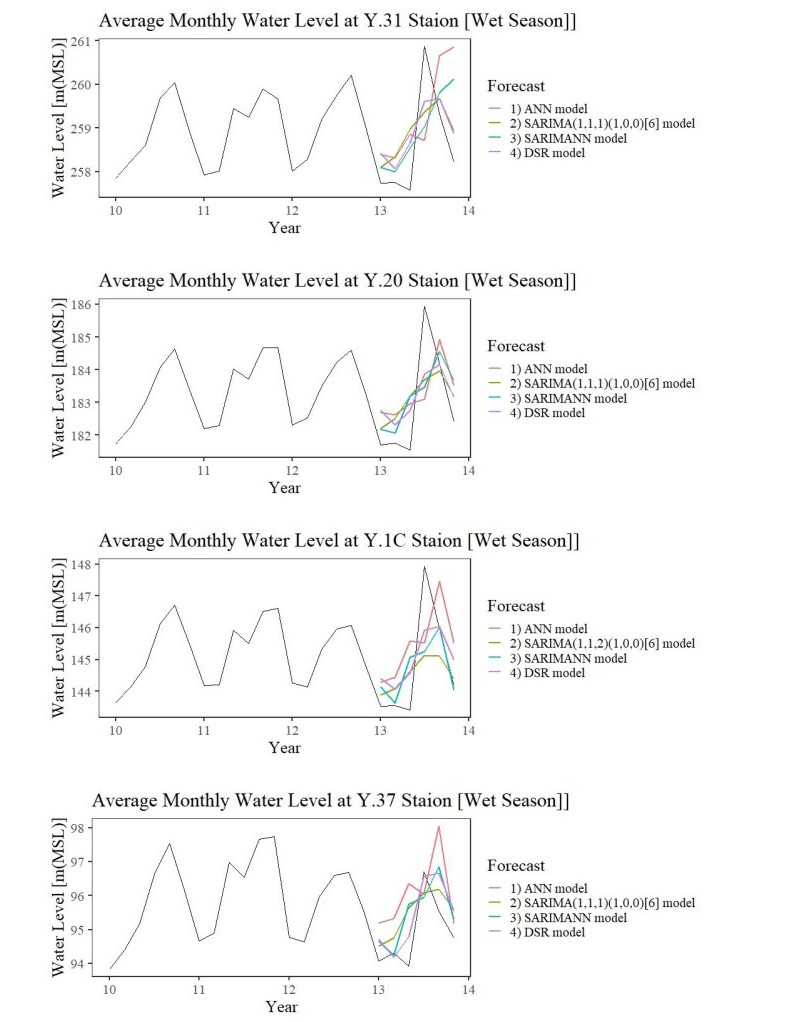
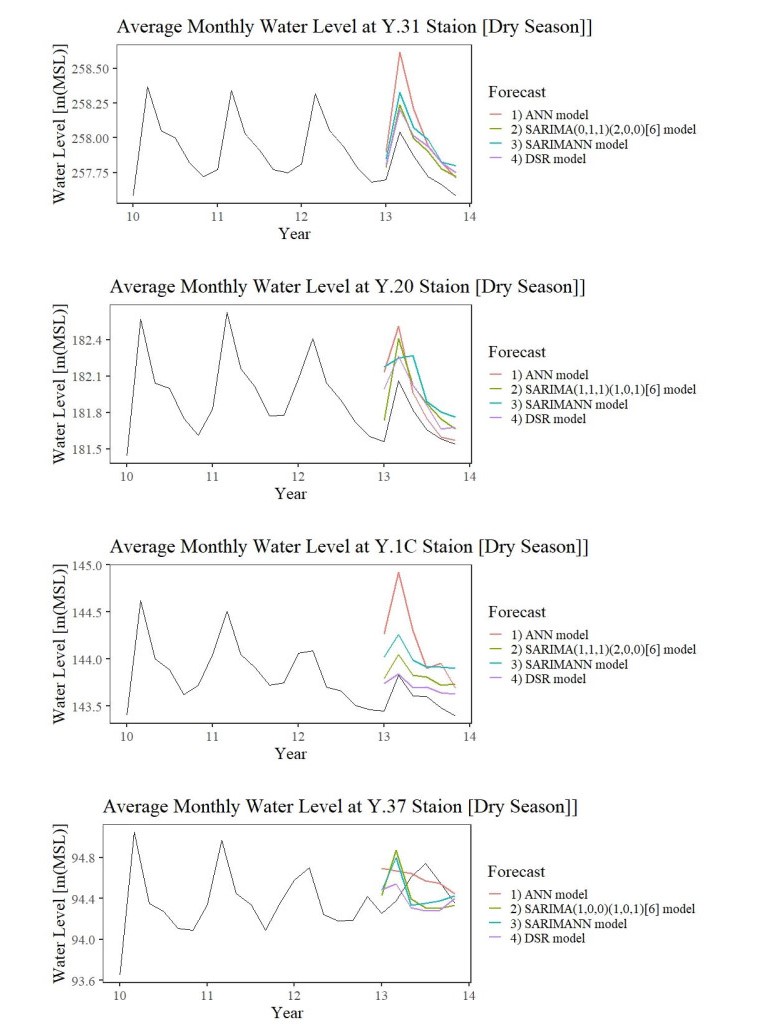
The Yom River Basin is one of 25 river basins in Thailand. The Yom River Basin experiences perennial droughts and floods that heavily impact the agricultural sector. In order to reduce the impact, water management, including water level estimation, must be applied to critical basins like the Yom River Basin. An important task of management is the quantitative prediction of water levels. Four different modeling approaches were applied to forecast the average monthly water level (AMWL) data from four water level measurement stations for the wet season (May–October) and dry season (November–April) from 2007 to 2020. The forecast patterns obtained from the four approaches were similar to the observed historical values, except the upstream in wet season and downstream in dry season. Furthermore, the artificial neural network (ANN) approach overestimated forecasts for almost every station in both seasons. All four approaches were more accurate in the dry season than the wet season. This study proposed a forecasting method called dynamic seasonal regression (DSR), which was obtained by combining multiple linear regression (MLR) and the autoregressive integrated moving average (ARIMA) model of the random error from MLR. DSR was more efficient than ANN, seasonal-ARIMA (SARIMA) and a hybridized SARIMA and ANN approach (SARIMANN). On average, for all stations in wet and dry seasons, DSR reduced RMSE by over 40.86%, 9.10% and 23.07% with respect to ANN, SARIMA and SARIMANN, and MAPE by over 35.01%, 13.02% and 15.96% with respect to ANN, SARIMA and SARIMANN. The RMSE of upstream was higher than the RMSE downstream in the wet season for all methods, and the MAPE of upstream was lower than the downstream in both seasons for all methods. Moreover, the RMSE of upstream was lower than the downstream in the dry season for all methods except the ANN method.
Citation: Kitipol Nualtong, Ronnason Chinram, Piyawan Khwanmuang, Sukrit Kirtsaeng, Thammarat Panityakul. An efficiency dynamic seasonal regression forecasting technique for high variation of water level in Yom River Basin of Thailand[J]. AIMS Environmental Science, 2021, 8(4): 283-303. doi: 10.3934/environsci.2021019
The Yom River Basin is one of 25 river basins in Thailand. The Yom River Basin experiences perennial droughts and floods that heavily impact the agricultural sector. In order to reduce the impact, water management, including water level estimation, must be applied to critical basins like the Yom River Basin. An important task of management is the quantitative prediction of water levels. Four different modeling approaches were applied to forecast the average monthly water level (AMWL) data from four water level measurement stations for the wet season (May–October) and dry season (November–April) from 2007 to 2020. The forecast patterns obtained from the four approaches were similar to the observed historical values, except the upstream in wet season and downstream in dry season. Furthermore, the artificial neural network (ANN) approach overestimated forecasts for almost every station in both seasons. All four approaches were more accurate in the dry season than the wet season. This study proposed a forecasting method called dynamic seasonal regression (DSR), which was obtained by combining multiple linear regression (MLR) and the autoregressive integrated moving average (ARIMA) model of the random error from MLR. DSR was more efficient than ANN, seasonal-ARIMA (SARIMA) and a hybridized SARIMA and ANN approach (SARIMANN). On average, for all stations in wet and dry seasons, DSR reduced RMSE by over 40.86%, 9.10% and 23.07% with respect to ANN, SARIMA and SARIMANN, and MAPE by over 35.01%, 13.02% and 15.96% with respect to ANN, SARIMA and SARIMANN. The RMSE of upstream was higher than the RMSE downstream in the wet season for all methods, and the MAPE of upstream was lower than the downstream in both seasons for all methods. Moreover, the RMSE of upstream was lower than the downstream in the dry season for all methods except the ANN method.

| [1] | Office of the National Water Resources, The National Water Resources Management Strategies (2015-2026), 2019. Available from: http://www.onwr.go.th/?page id=3684 |
| [2] | Department of Water Resources, Water Situation: Drought area, 2019. Available from: http://data.dwr.go.th/dwr/watersituation/drought/index |
| [3] | Department of Water Resources, Water Situation: Flood Area, 2019. Available from: http://data.dwr.go.th/dwr/watersituation/deluge/index |
| [4] | P. Khwanmuang, R. Chinram, T. Panityakul. (2020) The Hydrological and Water Level Data in Yom River Basin of Thailand. J Math Comput Sci 10: 3026-3047. |
| [5] |
Zhang Q, Gu X, David CY, et al (2009) Abrupt behaviors of the streamflow of the Pearl River basin and implications for hydrological alterations across the Pearl River Delta, China. J Hydrol 377: 274-283. doi: 10.1016/j.jhydrol.2009.08.026

|
| [6] |
Zhang Q, Gu X, Singh V P, et al. (2015) Evaluation of ecological instream flow using multiple ecological indicators with consideration of hydrological alterations. J Hydrol 529: 711-722. doi: 10.1016/j.jhydrol.2015.08.066
|
| [7] |
Zhang Q, Gu X, Singh V P, et al. (2015) Homogenization of precipitation and flow regimes across China: changing properties, causes and implications. J Hydrol 530: 462-475. doi: 10.1016/j.jhydrol.2015.09.041
|
| [8] | Sopipan N (2014) Forecasting Rainfall in Thailand: A Case Study of Nakhon Ratchasima Province, Int J Environ Ecol Geol Mar Eng 8: 712-716. |
| [9] |
Fashae O A, Olusola A O, Ndubuisi I, et al. (2018) Comparing ANN and ARIMA model in predicting the discharge of River Opeki from 2010 to 2020. River Res Appl 35: 169-177. doi: 10.1002/rra.3391
|
| [10] | Siripanich P. Time series forecasting using a combined ARIMA and artificial neural network model, 2019. Available from: http://www.sure.su.ac.th/xmlui/bitstream/handle/123456789/11717/Fulltext.pdf?sequence=1&isAllowed=y |
| [11] | Hyndman R J, Athanasopoulos G (2018) Forecasting: Principles and Practice, 2018. Available from: https://otexts.com/fpp2/ |
| [12] | Box GEP, Jenkins GM, Reinsel GC, et al. (2015) Time series analysis: Forecasting and control, 5 Eds., Hoboken, New Jersey: John Wiley & Sons. |
| [13] | Fu C, Ding F, Li Y, et al. (2021) Learning dynamic regression with automatic distractor repression for real-time UAV tracking, Engineering Applications of Artificial Intelligence. 98: 104116. |
| [14] | Hydro - Informatics Institute (Public Organization), Implementation of data collection and analysis of data on the 25 river basin data warehouse of the system development project, and modeling flood and drought (Yom River basin), 2019. Available from: http://www.thaiwater.net/web/attachments/25basins/08-yom.pdf |
| [15] | Bureau of Water Management and Hydrology (Royal Irrigation Department), Water allocation and cultivation plan for irrigation area during the dry season in 2019 - 2020, 2019. Available from: http://water.rid.go.th/hwm/wmoc/planing/dry/manage water2562-63.pdf |
| [16] | Upper Northern Region Irrigation Hydrology Center (Royal Irrigation Department), Average daily of water level - water content data, 2019. Available from: http://hydro-1.rid.go.th/ |
| [17] | Upper Northern Region Irrigation Hydrology Center (Royal Irrigation Department), Station history: Hydrological station of Yom River (Y.1C), Ban Nam Khong, Pa Maet sub-district, Mueang Phrae district, Phrae province, 2019. Available from: https://www.hydro-1.net/Data/STATION/History/Y1c.pdf |
| [18] | Upper Northern Region Irrigation Hydrology Center (Royal Irrigation Department), Station history: Hydrological station of Yom River (Y.20), Ban Huai Sak, Tao Pun sub-district, Song district, Phrae province, 2019. Available from: https://www.hydro-1.net/Data/STATION/History/Y20.pdf |
| [19] | Upper Northern Region Irrigation Hydrology Center (Royal Irrigation Department), Station history: Hydrological station of Yom River (Y.31), Ban Thung Nong, Sa sub-district, Chiang Muan district, Phayao province, 2019. Available from: https://www.hydro-1.net/Data/STATION/History/Y31.pdf |
| [20] | Upper Northern Region Irrigation Hydrology Center (Royal Irrigation Department), Station history: Hydrological station of Yom River (Y.37), Ban Wang Chin, Wang Chin sub-district, Wang Chin district, Phrae province, 2019. Available from: https://www.hydro-1.net/Data/STATION/History/Y37. |
| [21] | Fouli H, Fouli R, Bashir B, et al. (2018) Seasonal Forecasting of Rainfall and Runoff Volumes in Riyadh Region, KSA, KSCE Journal of Civil Engineering. 22: 2637-2647. |
| [22] | R. Nau, Statistical forecasting: notes on regression and time series analysis. Available from https://people.duke.edu/~rnau/411home.htm |
| [23] | Nualtong K, Panityakul T, Khwanmuang P, et al. (2021) A Hybrid Seasonal Box Jenkins-ANN Approach for Water Level Forecasting in Thailand, Environment and Ecology Research. 9: 93-106. |
| [24] | TAN PN, Steinbach M, Kumar V (2014) Introduction to data mining, Pearson Education Limited, U.S.A. |
Figures(11) / Tables(7)

Kitipol Nualtong, Ronnason Chinram, Piyawan Khwanmuang, Sukrit Kirtsaeng, Thammarat Panityakul. An efficiency dynamic seasonal regression forecasting technique for high variation of water level in Yom River Basin of Thailand[J]. AIMS Environmental Science, 2021, 8(4): 283-303. doi: 10.3934/environsci.2021019







 DownLoad:
DownLoad: