Cerebral artery fenestration is a rare vascular anomaly, but its existence has been increasingly documented. The association of cerebral infarction and fenestration is of great clinical interest, and the exact underlying mechanism remains unclear. This study aims to identify risk factors contributing to cerebral infarction by computational hemodynamics analysis.
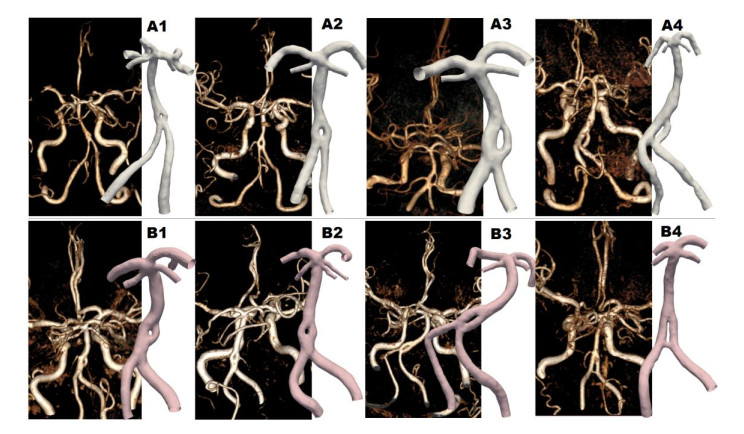
Eight patients with image findings of fenestration structure were recruited in this research, in which four suffered fenestration-related cerebral infarction (A series) while the other four (B series) were set as control matched by the fenestration size. Three-dimensional models were reconstructed from the MRA images and computational simulations with non-Newtonian flow model were performed to get interested hemodynamic characteristics.
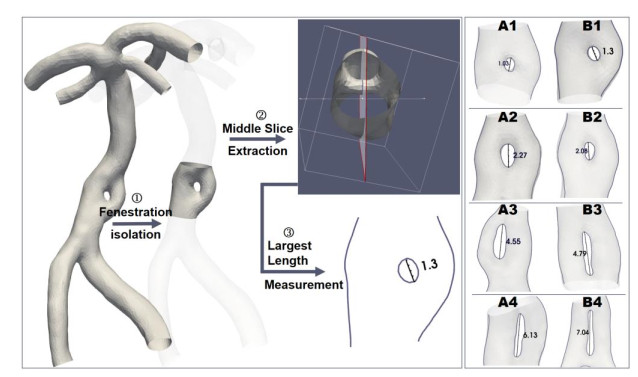
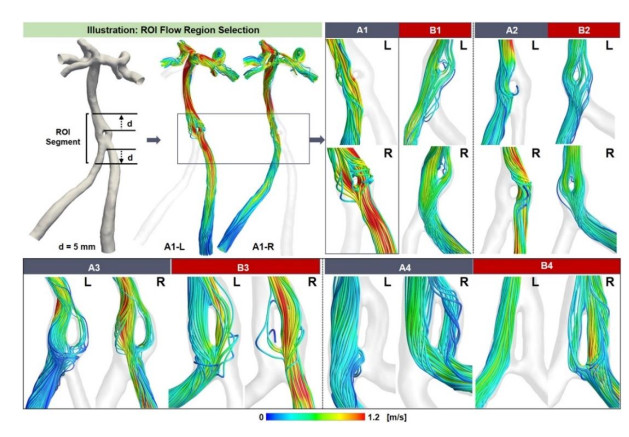
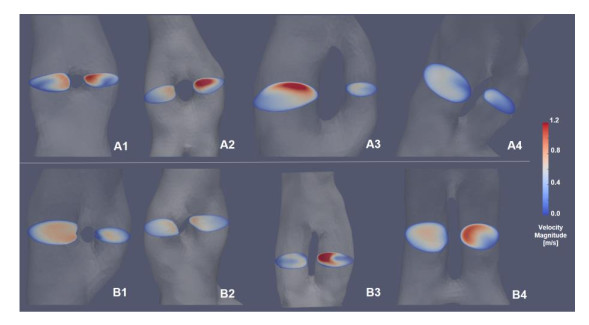
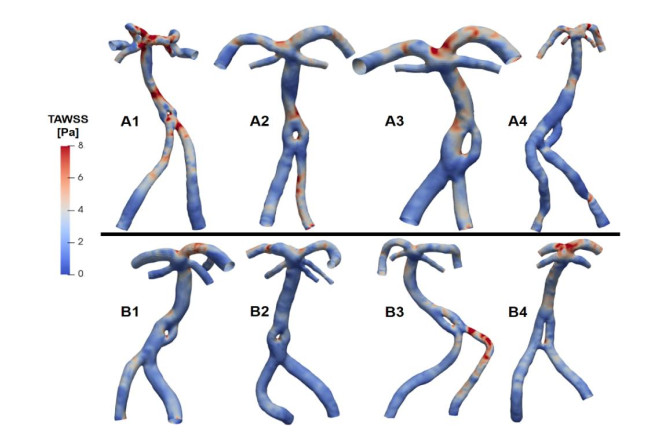
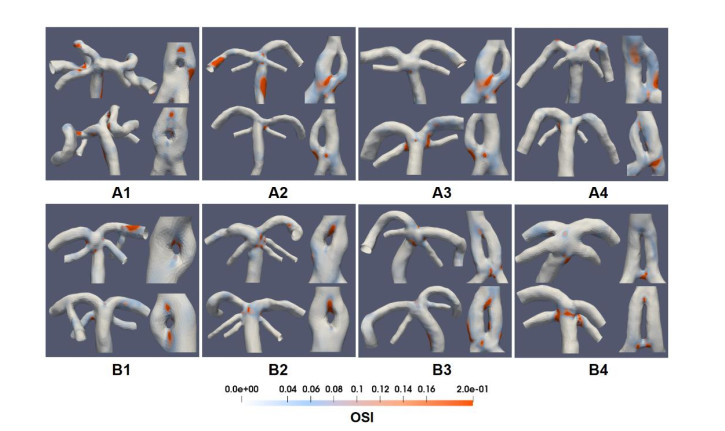
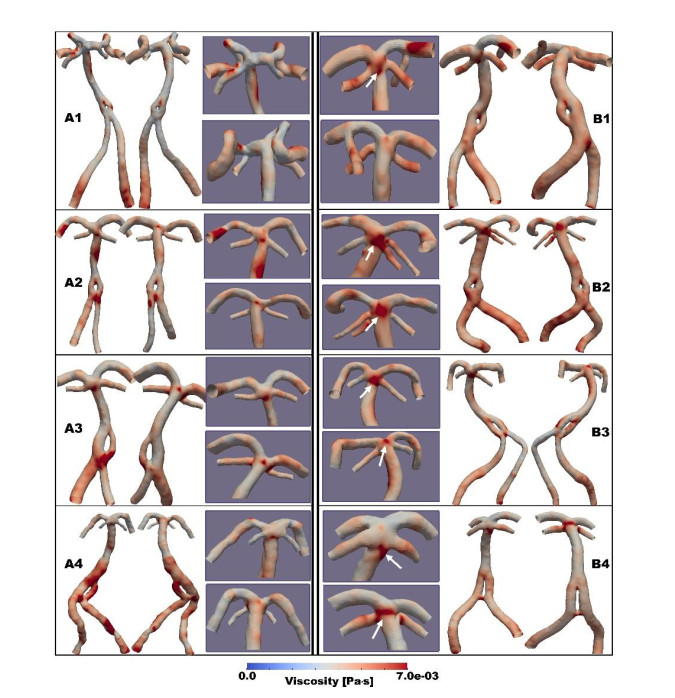
The blood flow pattern was relatively separated along two channels of fenestration in series A compared with series B cases in Group 1-2, however, no significant difference was shown in Group 3-4. Quantitatively, planes were cut in the middle of fenestrations and the ratio of mass flow rate and area was calculated at systolic peak. Results showed that the side of the dominant blood supply was opposite between A and B series, and the dominant side was also opposite between small and large fenestrations. In infarction cases, the basilar top was distributed with larger areas of detrimental hemodynamic indicators and a larger concentrated high viscosity region.
The flow division condition throughout the fenestration structure has a key impact on further flow redistribution and flow pattern. The blood viscosity has the potential to be a useful tool in identifying the risk factors for cerebral infarction and more emphasis should be placed on the hemodynamic environment at superior cerebellar arteries.
Citation: Yuqian Mei, Debao Guan, Xinyu Tong, Qian Liu, Mingcheng Hu, Guangxin Chen, Caijuan Li. Association of cerebral infarction with vertebral arterial fenestration using non-Newtonian hemodynamic evaluation[J]. Mathematical Biosciences and Engineering, 2022, 19(7): 7076-7090. doi: 10.3934/mbe.2022334
Cerebral artery fenestration is a rare vascular anomaly, but its existence has been increasingly documented. The association of cerebral infarction and fenestration is of great clinical interest, and the exact underlying mechanism remains unclear. This study aims to identify risk factors contributing to cerebral infarction by computational hemodynamics analysis.
Eight patients with image findings of fenestration structure were recruited in this research, in which four suffered fenestration-related cerebral infarction (A series) while the other four (B series) were set as control matched by the fenestration size. Three-dimensional models were reconstructed from the MRA images and computational simulations with non-Newtonian flow model were performed to get interested hemodynamic characteristics.
The blood flow pattern was relatively separated along two channels of fenestration in series A compared with series B cases in Group 1-2, however, no significant difference was shown in Group 3-4. Quantitatively, planes were cut in the middle of fenestrations and the ratio of mass flow rate and area was calculated at systolic peak. Results showed that the side of the dominant blood supply was opposite between A and B series, and the dominant side was also opposite between small and large fenestrations. In infarction cases, the basilar top was distributed with larger areas of detrimental hemodynamic indicators and a larger concentrated high viscosity region.
The flow division condition throughout the fenestration structure has a key impact on further flow redistribution and flow pattern. The blood viscosity has the potential to be a useful tool in identifying the risk factors for cerebral infarction and more emphasis should be placed on the hemodynamic environment at superior cerebellar arteries.

| [1] | P. Gailloud, S. Albayram, J. H. D. Fasel, N. J. Beauchamp, K. J. Murphy, Angiographic and embryologic considerations in five cases of middle cerebral artery fenestration, AJNR Am. J. Neuroradiol., 23 (2002), 585-587. |
| [2] | F. Cademartiri, D. Stojanov, D. W. J. Dippel, A. van der Lugt, H. Tanghe, Noninvasive detection of a ruptured aneurysm at a basilar artery fenestration with submillimeter multisection CT angiography, AJNR Am. J. Neuroradiol., 24 (2003), 2009-2010. |
| [3] | L. Hacein-Bey, C. A. Muszynski, P. N. Varelas, Saccular Aneurysm Associated with Posterior Cerebral Artery Fenestration Manifesting as a Subarachnoid Hemorrhage in a Child, Am. J. Neuroradiol., 23 (2002), 1291. |
| [4] |
L. Arráez-Aybar, A. Villar-Martin, C. Poyatos-Ruiperez, G. Rodriguez-Boto, J. Arrazola-Garcia, Prevalence of fenestrated basilar artery with magnetic resonance angiography: a transversal study, Surg. Radiol. Anat., 35 (2013), 487-493. https://doi.org/10.1007/s00276-012-1053-5 doi: 10.1007/s00276-012-1053-5

|
| [5] | H. Pleş, M. Loukas, N. Iacob, N. R. Andall, G. D. Miclăuş, R. S. Tubbs, et al., Duplication of the distal end of the left vertebral artery with fenestration of the right posterior cerebral artery, Rom. J. Morphol. Embryol., 56 (2015), 575-577. |
| [6] |
A. Uchino, N. Saito, M. Takahashi, N. Okano, M. Tanisaka, Variations of the posterior cerebral artery diagnosed by MR angiography at 3 tesla, Neuroradiol., 58 (2016), 141-146. https://doi.org/10.1007/s00234-015-1614-5 doi: 10.1007/s00234-015-1614-5
|
| [7] | W. P. Sanders, P. A. Sorek, B. A. Mehta, Fenestration of intracranial arteries with special attention to associated aneurysms and other anomalies, AJNR Am. J. Neuroradiol., 14 (1993), 675-680. |
| [8] |
S. Kathuria, L. Gregg, J. Chen, D. Gandhi, Normal cerebral arterial development and variations, Semin Ultrasound CT MR, 32 (2011), 242-251. https://doi.org/10.1053/j.sult.2011.02.002 doi: 10.1053/j.sult.2011.02.002
|
| [9] | Y. Y. Chen, F. C. Chang, H. H. Hu, A. C. Chao, Fenestration of the supraclinoid internal carotid artery associated with aneurysm and ischemic stroke, Surg. Neurol., 68 (2007), S60-63; discussion S63. https://doi.org/10.1016/j.surneu.2007.05.051 |
| [10] |
M. Kanematsu, K. Satoh, N. Nakajima, F. Hamazaki, S. Nagahiro, Ruptured aneurysm arising from a basilar artery fenestration and associated with a persistent primitive hypoglossal artery. Case report and review of the literature, J. Neurosurg., 101 (2004), 532-535. https://doi.org/10.3171/jns.2004.101.3.0532 doi: 10.3171/jns.2004.101.3.0532
|
| [11] |
M. A. Patel, J. M. Caplan, W. Yang, G. P. Colby, A. L. Coon, R. J. Tamargo, et al., Arterial fenestrations and their association with cerebral aneurysms, J. Clin. Neurosci., 21 (2014), 2184-2188. https://doi.org/10.1016/j.jocn.2014.07.005 doi: 10.1016/j.jocn.2014.07.005
|
| [12] |
E. Vörös, M. Kiss, J. Hankó, E. Nagy, Moyamoya with arterial anomalies: relevance to pathogenesis, Neuroradiol., 39 (1997), 852-856. https://doi.org/10.1007/s002340050519 doi: 10.1007/s002340050519
|
| [13] | M. A. Piccinin, S. Munakomi, Neuroanatomy, Vertebrobasilar System, 2019. |
| [14] | F. Yilmaz, M.Y. Gundogdu, A critical review on blood flow in large arteries; relevance to blood rheology, viscosity models, and physiologic conditions, Korea-Australia Rheol. J., 20 (2008), 197-211. |
| [15] |
J. Chen, X-Y Lu, Numerical investigation of the non-Newtonian blood flow in a bifurcation model with a non-planar branch, J. Biomech., 37 (2004), 1899-1911. https://doi.org/10.1016/j.jbiomech.2004.02.030 doi: 10.1016/j.jbiomech.2004.02.030
|
| [16] |
A. Arzani, Accounting for residence-time in blood rheology models: do we really need non-Newtonian blood flow modelling in large arteries?, J. R. Soc. Interface, 15 (2018), 20180486. https://doi.org/10.1098/rsif.2018.0486 doi: 10.1098/rsif.2018.0486
|
| [17] |
X. Tong, J. Dong, G. Zhou, X. Zhang, A. Wang, Z. Ji, et al., Hemodynamic effects of size and location of basilar artery fenestrations associated to pathological implications, Int. J. Numer. Methods Biomed. Eng., 37 (2021), e3507. https://doi.org/10.1002/cnm.3507 doi: 10.1002/cnm.3507
|
| [18] |
J. Bernsdorf, D. Wang, Non-Newtonian blood flow simulation in cerebral aneurysms, Comput. Math. Appl., 58 (2009), 1024-1029. https://doi.org/10.1016/j.camwa.2009.02.019 doi: 10.1016/j.camwa.2009.02.019
|
| [19] |
C. Fisher, J. S. Rossmann, Effect of non-Newtonian behavior on hemodynamics of cerebral aneurysms, J. Biomechan. Eng., 131 (2009). https://doi.org/10.1115/1.3148470 doi: 10.1115/1.3148470
|
| [20] | I. Husain, C. Langdon, J. Schwark, Non-Newtonian pulsatile blood flow in a modeled artery with a stenosis and an aneurysm, Rec. Res. Envi. Geo. Sc, 413-418. |
| [21] |
J. Xiang, V. M. Tutino, K. V. Snyder, H. Meng, CFD: computational fluid dynamics or confounding factor dissemination? The role of hemodynamics in intracranial aneurysm rupture risk assessment, Am. J. Neuroradiol., 35 (2014), 1849-1857. https://doi.org/10.3174/ajnr.A3710 doi: 10.3174/ajnr.A3710
|
| [22] |
S. Saalfeld, S. Voß, O. Beuing, B. Preim, P. Berg, Flow-splitting-based computation of outlet boundary conditions for improved cerebrovascular simulation in multiple intracranial aneurysms, Int. J. Comput. Assist. Radiol. Surg., 14 (2019), 1805-1813. https://doi.org/10.1007/s11548-019-02036-7 doi: 10.1007/s11548-019-02036-7
|
| [23] |
D. Ye, J. Huang, S. Wang, S. Sheng, M. Liu, Cerebral arterial fenestration associated with stroke and other cerebrovascular diseases, NeuroReport, 32 (2021), 1279-1286. https://doi.org/10.1097/WNR.0000000000001720 doi: 10.1097/WNR.0000000000001720
|
| [24] | M. Bruneau, O. De Witte, L. Regli, B. George, Anatomical variations. In Pathology and surgery around the vertebral artery, Springer, Paris, 2011. pp. 53-74. https://doi.org/10.1007/978-2-287-89787-0_7 |
| [25] |
N. Miyamoto, Y. Ueno, K. Hira, C. Kijima, S. Nakajima, K.Yamashiro, et al., Characteristics of Clinical Symptoms, Cerebral Images and Stroke Etiology in Vertebro-Basilar Artery Fenestration-Related Infarction, Brain Sci., 10 (2020), 243. https://doi.org/10.3390/brainsci10040243 doi: 10.3390/brainsci10040243
|
| [26] |
M. Kubo, L. Hacein-Bey, P. N. Varelas, J. L. Ulmer, D. M. Lemke, J. F. Cusick, Ruptured saccular aneurysm of distal vertebral artery fenestration managed with Guglielmi detachable coils and intraventricular tissue plasminogen activator, Surg. Neurol., 63 (2005), 244-248. https://doi.org/10.1016/j.surneu.2004.02.038 doi: 10.1016/j.surneu.2004.02.038
|
| [27] |
E.o. Ott, H. Lechner, A. Aranibar, High blood viscosity syndrome in cerebral infarction, Stroke, 5 (1974), 330-333. https://doi.org/10.1161/01.STR.5.3.330 doi: 10.1161/01.STR.5.3.330
|
| [28] |
K. Furukawa, T. Abumiya, K. Sakai, M. Hirano, T. Osanai, H. Shichinohe, Increased blood viscosity in ischemic stroke patients with small artery occlusion measured by an electromagnetic spinning sphere viscometer, J. Stroke Cerebrovasc. Dis., 25 (2016), 2762-2769. https://doi.org/10.1016/j.jstrokecerebrovasdis.2016.07.031 doi: 10.1016/j.jstrokecerebrovasdis.2016.07.031
|
| [29] |
S. H. Song, J. H. Kim, J. H. Lee, Y. M. Yun, D. H. Choi, H. Y. Kim, Elevated blood viscosity is associated with cerebral small vessel disease in patients with acute ischemic stroke, BMC Neurol., 17(2017), 1-10. https://doi.org/10.1186/s12883-017-0808-3 doi: 10.1186/s12883-017-0808-3
|
| [30] |
B. M. Coull, N. Beamer, P. De Garmo, G. Sexton, F. Nordt, R. Knox, et al., Chronic blood hyperviscosity in subjects with acute stroke, transient ischemic attack, and risk factors for stroke, Stroke, 22 (1991), 162-168. https://doi.org/10.1161/01.STR.22.2.162 doi: 10.1161/01.STR.22.2.162
|
| [31] |
E. Sim, A. R. Vaccaro, A. Berzlanovich, H. Thaler, C. G. Ullrich, Fenestration of the extracranial vertebral artery: review of the literature, Spine, 26 (2001), E139-E142. https://doi.org/10.1097/00007632-200103150-00007 doi: 10.1097/00007632-200103150-00007
|
| [32] | X. Meng, W. Ding, X. Wu, P. Di, Clinical investigation and characterization of vertebrobasilar dolichoectasia and vertebral artery dominance, Discov. Med., 25 (2018), 151-158. |
 mbe-19-07-334 S1.pdf mbe-19-07-334 S1.pdf |
 |
Figures(7) / Tables(3)

Yuqian Mei, Debao Guan, Xinyu Tong, Qian Liu, Mingcheng Hu, Guangxin Chen, Caijuan Li. Association of cerebral infarction with vertebral arterial fenestration using non-Newtonian hemodynamic evaluation[J]. Mathematical Biosciences and Engineering, 2022, 19(7): 7076-7090. doi: 10.3934/mbe.2022334







 DownLoad:
DownLoad: