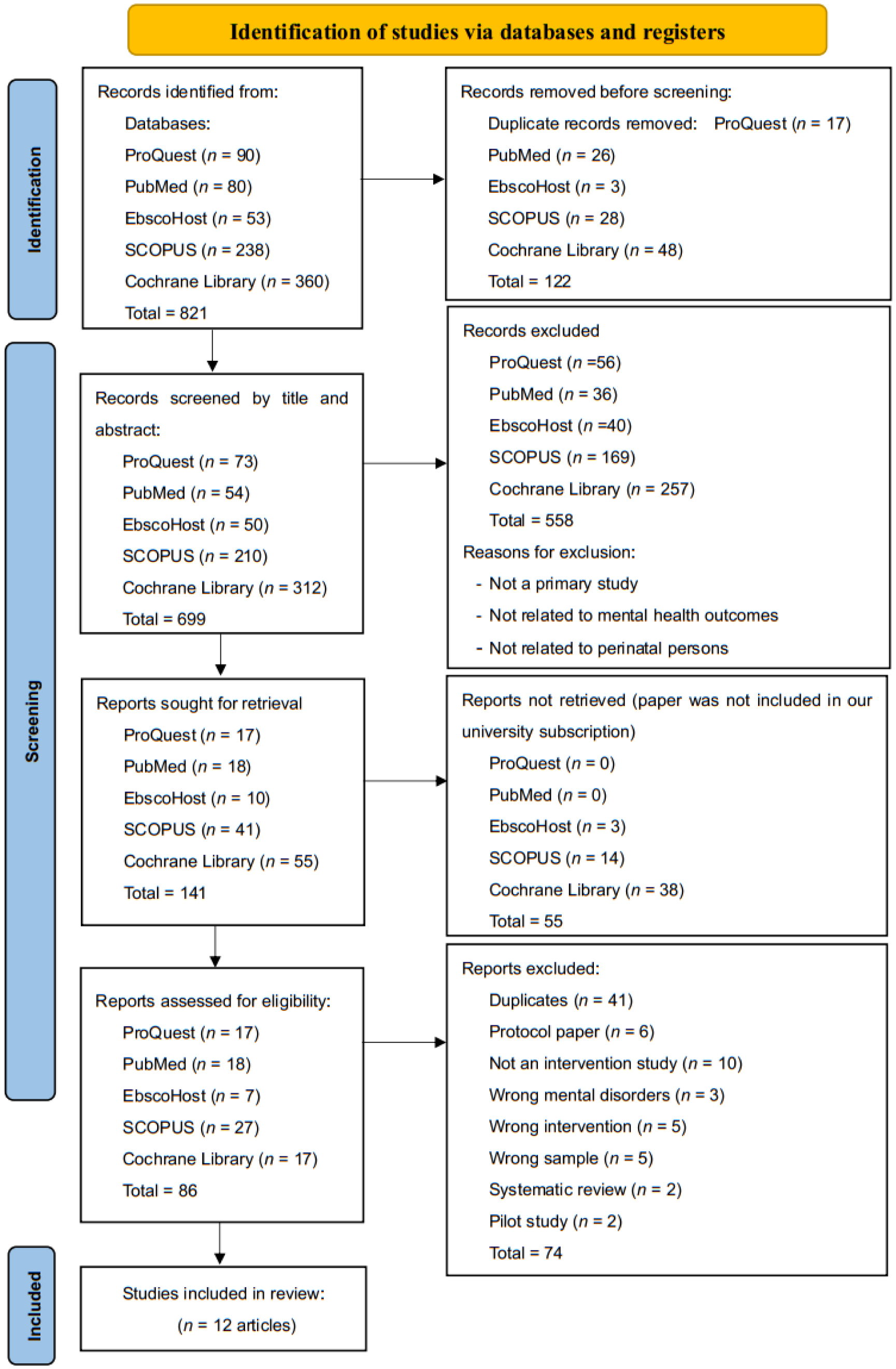
Digital intervention has been shown to be helpful in improving perinatal mental health. However, the design characteristics of such interventions have not been systematically reviewed. Considering that a lack of support—especially from a partner—is one of the major contributing factors to perinatal depression and anxiety, it is crucial to determine whether digital interventions have included partner participation. In this review, we systematically examined the design characteristics of digital interventions related to perinatal depression and anxiety and aimed to determine whether partner participation was incorporated as part of the interventions. Based on the PRISMA 2020 guidelines, five databases (PubMed, EBSCO, Cochrane, ProQuest, and Scopus) were searched. Narrative results of design characteristics were developed to provide a framework for the design and evaluation of the studies. A total of 12 intervention studies from China, Sweden, Australia, New Zealand, Singapore, Norway, and the United Kingdom were included. Across all studies, internet cognitive behavioral therapy and mindfulness therapy were overwhelmingly utilized as the major intervention approaches. While all studies reported reduced depressive symptoms after the intervention, only four studies reported subsequent decreased levels of both depressive and anxiety symptoms. Only one study included partner support in the intervention. Cognitive behavioral therapy and mindfulness therapy, two of the most common intervention approaches, were found to be effective in alleviating perinatal depression and anxiety. Partner participation should be prioritized in designing digital interventions to ensure comprehensive and easily accessible social support for persons in need.
Citation: Siti Roshaidai Mohd Arifin, Amalia Kamaruddin, Noor Azimah Muhammad, Mohd Said Nurumal, Hazwani Mohd Mohadis, Nik Hazlina Nik Hussain, Shanti Wardaningsih. An evaluation of digital intervention for perinatal depression and anxiety: A systematic review[J]. AIMS Public Health, 2024, 11(2): 499-525. doi: 10.3934/publichealth.2024025
Digital intervention has been shown to be helpful in improving perinatal mental health. However, the design characteristics of such interventions have not been systematically reviewed. Considering that a lack of support—especially from a partner—is one of the major contributing factors to perinatal depression and anxiety, it is crucial to determine whether digital interventions have included partner participation. In this review, we systematically examined the design characteristics of digital interventions related to perinatal depression and anxiety and aimed to determine whether partner participation was incorporated as part of the interventions. Based on the PRISMA 2020 guidelines, five databases (PubMed, EBSCO, Cochrane, ProQuest, and Scopus) were searched. Narrative results of design characteristics were developed to provide a framework for the design and evaluation of the studies. A total of 12 intervention studies from China, Sweden, Australia, New Zealand, Singapore, Norway, and the United Kingdom were included. Across all studies, internet cognitive behavioral therapy and mindfulness therapy were overwhelmingly utilized as the major intervention approaches. While all studies reported reduced depressive symptoms after the intervention, only four studies reported subsequent decreased levels of both depressive and anxiety symptoms. Only one study included partner support in the intervention. Cognitive behavioral therapy and mindfulness therapy, two of the most common intervention approaches, were found to be effective in alleviating perinatal depression and anxiety. Partner participation should be prioritized in designing digital interventions to ensure comprehensive and easily accessible social support for persons in need.

| [1] |
Korja R, Nolvi S, Kataja EL, et al. (2018) The courses of maternal and paternal depressive and anxiety symptoms during the prenatal period in the FinnBrain Birth Cohort study. PLoS One 13: e0207856. https://doi.org/10.1371/journal.pone.0207856 
|
| [2] |
Earls MF, Yogman MW, Mattson G, et al. (2019) Committee on Psychosocial Aspects of Child and Family Health. Incorporating recognition and management of perinatal depression into pediatric practice. Pediatrics 143: e20183259. https://doi.org/10.1542/peds.2018-3259
|
| [3] |
Dennis CL, Falah-Hassani K, Shiri R (2017) Prevalence of antenatal and postnatal anxiety: Systematic review and meta-analysis. Br J Psychiatry 210: 315-323. https://doi.org/10.1192/bjp.bp.116.187179
|
| [4] |
Yeaton-Massey A, Herrero T (2019) Recognizing maternal mental health disorders: Beyond postpartum depression. Curr Opin Obstet Gynecol 31: 116-119. https://doi.org/10.1097/GCO.0000000000000524
|
| [5] |
Abd Rahman FN, Wong YY, Khalib AQ (2022) Relationship between postnatal depression of mental health patients and the psychological health of their offspring. Front Psychiatry 12: 772744. https://doi.org/10.3389/fpsyt.2021.772744
|
| [6] |
Rees S, Channon S, Waters CS (2019) The impact of maternal prenatal and postnatal anxiety on children's emotional problems: A systematic review. Eur Child Adolesc Psychiatry 28: 257-280. https://doi.org/10.1007/s00787-018-1173-5
|
| [7] |
Ryan J, Mansell T, Fransquet P, et al. (2017) Does maternal mental well-being in pregnancy impact the early human epigenome?. Epigenomics 9: 313-332. https://doi.org/10.2217/epi-2016-0118
|
| [8] |
Oh S, Chew-Graham CA, Silverwood V, et al. (2020) Exploring women's experiences of identifying, negotiating and managing perinatal anxiety: A qualitative study. BMJ Open 10: e040731. https://doi.org/10.1136/bmjopen-2020-040731
|
| [9] |
Pebryatie E, Paek SC, Sherer P, Meemon N (2022) Associations between spousal relationship, husband involvement, and postpartum depression among postpartum mothers in West Java, Indonesia. J Prim Care Community Health 13: 21501319221088355. https://doi.org/10.1177/21501319221088355
|
| [10] |
Durankuş F, Aksu E (2022) Effects of the COVID-19 pandemic on anxiety and depressive symptoms in pregnant women: A preliminary study. J Matern Fetal Neonatal Med 35: 205-211. https://doi.org/10.1080/14767058.2020.1763946
|
| [11] |
Patabendige M, Gamage MM, Weerasinghe M, et al. (2020) Psychological impact of the COVID-19 pandemic among pregnant women in Sri Lanka. Int J Gynaecol Obstet 151: 150-153. https://doi.org/10.1002/ijgo.13335
|
| [12] |
Zimmermann M, Peacock-Chambers E, Merton C, et al. (2023) Equitable reach: Patient and professional recommendations for interventions to prevent perinatal depression and anxiety. Gen Hosp Psychiatry 85: 95-103. https://doi.org/10.1016/j.genhosppsych.2023.10.003
|
| [13] |
Beerli J, Ehlert U, Amiel RT (2022) Internet-based interventions for perinatal depression and anxiety symptoms: An ethnographic qualitative study exploring the views and opinions of midwives in Switzerland. BMC Primary Care 23: 172. https://doi.org/10.1186/s12875-022-01779-8
|
| [14] |
Mao F, Sun Y, Li Y, et al. (2023) Internet-delivered mindfulness-based interventions for mental health outcomes among perinatal women: A systematic review. Asian J Psychiatr 80: 103321. https://doi.org/10.1016/j.ajp.2022.103321
|
| [15] |
Ashford MT, Olander EK, Ayers S (2016) Computer- or web-based interventions for perinatal mental health: A systematic review. J Affect Disord 197: 134-146. https://doi.org/10.1016/j.jad.2016.02.057
|
| [16] |
Müller M, Matthies LM, Goetz M, et al. (2020) Effectiveness and cost-effectiveness of an electronic mindfulness-based intervention (eMBI) on maternal mental health during pregnancy: The mindmom study protocol for a randomized controlled clinical trial. Trials 21: 933. https://doi.org/10.1111/pere.12221
|
| [17] | Zingg A, Carter L, Rogith D, et al. (2021) Digital technology needs in maternal mental health: A qualitative inquiry. Stud Health Technol Inform 281: 979-983. https://doi.org/10.3233/SHTI210324 |
| [18] |
Sprenger M, Mettler T, Osma J (2017) Health professionals' perspective on the promotion of e-mental health apps in the context of maternal depression. PLoS One 12: e0180867. https://doi.org/10.1371/journal.pone.0180867
|
| [19] |
Haga SM, Kinser PA, Wentzel-Larsen T, et al. (2020) Mamma Mia–A randomized controlled trial of an internet intervention to enhance subjective well-being in perinatal women. J Posit Psychol 16: 446-454. https://doi.org/10.1080//17439760.2020.1738535
|
| [20] |
Saleem M, Kühne L, Karolina K, et al. (2021) Understanding engagement strategies in digital interventions for mental health promotion: Scoping review. JMIR Mental Health 8: e30000-e30000. https://doi.org/10.2196/30000
|
| [21] |
Page MJ, McKenzie JE, Bossuyt PM, et al. (2021) The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 372: n71. https://doi.org/10.1136/bmj.n71
|
| [22] | Kmet LM, Lee RC, Cook LS Standard quality assessment criteria for evaluating primary research papers from a variety of fields (2014). Available from: https://era.library.ualberta.ca/items/48b9b989-c221-4df6-9e35-af782082280e/download/a1cffdde-243e-41c3-be98-885f6d4dcb29 |
| [23] |
Sjömark J, Svanberg AS, Larsson M, et al. (2022) Effect of internet-based cognitive behaviour therapy among women with negative birth experiences on mental health and quality of life-a randomized controlled trial. BMC Pregnancy Childb 22: 835. https://doi.org/10.1186/s12884-022-05168-y
|
| [24] |
Bear KA, Barber CC, Medvedev ON (2022) The impact of a mindfulness app on postnatal distress. Mindfulness 13: 2765-2776. https://doi.org/10.1007/s12671-022-01992-7
|
| [25] |
Sun Y, Li Y, Wang J, et al. (2021) Effectiveness of smartphone-based mindfulness training on maternal perinatal depression: Randomized controlled trial. J Med Internet Res 23: e23410. https://doi.org/10.2196/23410
|
| [26] |
Chan KL, Leung WC, Tiwari A, et al. (2019) Using smartphone-based psychoeducation to reduce postnatal depression among first-time mothers: Randomized controlled trial. JMIR Mhealth Uhealth 7: e12794. https://doi.org/10.2196/12794
|
| [27] |
Shorey S, Ng ED (2019) Evaluation of a technology-based peer-support intervention program for preventing postnatal depression (Part 2): Qualitative study. J Med Internet Res 21: e12915. https://doi.org/10.2196/12915
|
| [28] |
Haga SM, Drozd F, Lisøy C, et al. (2019) Mamma Mia-A randomized controlled trial of an internet-based intervention for perinatal depression. Psychol Med 49: 1850-1858. https://doi.org/10.1017/S0033291718002544
|
| [29] |
Yang M, Jia G, Sun S, et al. (2019) Effects of an online mindfulness intervention focusing on attention monitoring and acceptance in pregnant women: A randomized controlled trial. J Midwifery Womens Health 64: 68-77. https://doi.org/10.1111/jmwh.12944
|
| [30] |
Guo L, Zhang J, Mu L, et al. (2020) Preventing postpartum depression with mindful self-compassion intervention: A randomized control study. J Nerv Ment Dis 208: 101-107. https://doi.org/10.1097/NMD.0000000000001096
|
| [31] |
Loughnan SA, Butler C, Sie AA, et al. (2019) A randomised controlled trial of ‘MUMentum postnatal’: Internet-delivered cognitive behavioural therapy for anxiety and depression in postpartum women. Behav Res Ther 116: 94-103. https://doi.org/10.1016/j.brat.2019.03.001
|
| [32] |
Krusche A, Dymond M, Murphy SE, et al. (2018) Mindfulness for pregnancy: A randomised controlled study of online mindfulness during pregnancy. Midwifery 65: 51-57. https://doi.org/10.1016/j.midw.2018.07.005
|
| [33] |
Forsell E, Bendix M, Holländare F, et al. (2017) Internet delivered cognitive behavior therapy for antenatal depression: A randomised controlled trial. J Affect Disord 221: 56-64. https://doi.org/10.1016/j.jad.2017.06.013
|
| [34] |
Milgrom J, Danaher BG, Gemmill AW, et al. (2016) Internet cognitive behavioral therapy for women with postnatal depression: A randomized controlled trial of MumMoodBooster. J Med Internet Res 18: e54. https://doi.org/10.2196/jmir.4993
|
| [35] |
Mu TY, Li YH, Xu RX, et al. (2021) Internet-based interventions for postpartum depression: A systematic review and meta-analysis. Nurs Open 8: 1125-1134. https://doi.org/10.1002/nop2.724
|
| [36] |
Lau Y, Htun TP, Wong SN, et al. (2017) Therapist-supported internet-based cognitive behavior therapy for stress, anxiety, and depressive symptoms among postpartum women: A systematic review and meta-analysis. J Med Internet Res 19: e138. https://doi.org/10.2196/jmir.6712
|
| [37] |
Nishi D, Imamura K, Watanabe K, et al. (2022) The preventive effect of internet-based cognitive behavioral therapy for prevention of depression during pregnancy and in the postpartum period (iPDP): A large scale randomized controlled trial. Psychiat Clin Neuros 76: 570-578. https://doi.org/10.1111/pcn.13458
|
| [38] |
Maguire PN, Clark GI, Cosh S, et al. (2023) Exploring experiences, barriers and treatment preferences for self-reported perinatal anxiety in Australian women: A qualitative study. Aust Psych 59: 46-59. https://doi.org/10.1080//00050067.2023.2236281
|
| [39] |
Stentzel U, Grabe HJ, Schmidt S, et al. (2023) Mental health-related telemedicine interventions for pregnant women and new mothers: A systematic literature review. BMC Psychiatry 23: 292. https://doi.org/10.1186/s12888-023-04790-0
|
| [40] |
Cox G, Hetrick S (2017) Psychosocial interventions for self-harm, suicidal ideation and suicide attempt in children and young people: What? How? Who? and Where?. Evid Based Ment Health 20: 35-40. https://doi.org/10.1136/eb-2017-102667
|
| [41] | Kumar V, Sattar Y, Bseiso A, et al. (2017) The effectiveness of internet-based cognitive behavioral therapy in treatment of psychiatric disorders. Cureus 9: e1626. https://doi.org/10.7759/cureus.1626 |
| [42] |
Li X, Laplante DP, Paquin V, et al. (2022) Effectiveness of cognitive behavioral therapy for perinatal maternal depression, anxiety and stress: A systematic review and meta-analysis of randomized controlled trials. Clin Psychol Rev 92: 102129. https://doi.org/10.1016/j.cpr.2022.102129
|
| [43] |
Chen C, Wang X, Xu H, et al. (2023) Effectiveness of digital psychological interventions in reducing perinatal depression: A systematic review of meta-analyses. Arch Womens Ment Health 26: 423-439. https://doi.org/10.1007/s00737-023-01327-y
|
| [44] |
Neo HS, Tan JH, How W, et al. (2022) Internet-delivered psychological interventions for reducing depressive, anxiety symptoms and fear of childbirth in pregnant women: A meta-analysis and meta-regression. J Psychosom Res 157: 110790-110790. https://doi.org/10.1016/j.jpsychores.2022.110790
|
| [45] |
Martinengo L, Stona AC, Griva K, et al. (2021) Self-guided cognitive behavioral therapy apps for depression: systematic assessment of features, functionality, and congruence with evidence. J Med Internet Res 23: e27619. https://doi.org/10.2196/27619
|
| [46] |
Wang C, Pan R, Wan X, et al. (2020) A longitudinal study on the mental health of general population during the COVID-19 epidemic in China. Brain Behav Immun 87: 40-48. https://doi.org/10.1016/j.bbi.2020.04.028
|
| [47] |
Rogers MA, Lemmen K, Kramer R, et al. (2017) Internet-delivered health interventions that work: Systematic review of meta-analyses and evaluation of website availability. J Med Internet Res 19: e90. https://doi.org/10.2196/jmir.7111
|
| [48] |
Clinkscales N, Golds L, Berlouis K, et al. (2022) The effectiveness of psychological interventions for anxiety in the perinatal period: A systematic review and meta-analysis. Psychol Psychother 96: 296-327. https://doi.org/10.1111/papt.12441
|
| [49] |
Suchan V, Peynenburg V, Thiessen D, et al. (2022) Transdiagnostic internet-delivered cognitive behavioral therapy for symptoms of postpartum anxiety and depression: Feasibility randomized controlled trial. JMIR Form Res 6: e37216. https://doi.org/10.2196/37216
|
| [50] |
Jannati N, Mazhari S, Ahmadian L, et al. (2020) Effectiveness of an app-based cognitive behavioral therapy program for postpartum depression in primary care: A randomized controlled trial. Int J Med Inform 141: 104-145. https://doi.org/10.1016/j.ijmedinf.2020.104145
|
| [51] |
Zhao L, Chen J, Lan L, et al. (2021) Effectiveness of telehealth interventions for women with postpartum depression: Systematic review and meta-analysis. JMIR Mhealth Uhealth 9: e32544. https://doi.org/10.2196/32544
|
| [52] |
Mahoney A, Shiner CT, Grierson AB, et al. (2023) Online cognitive behaviour therapy for maternal antenatal and postnatal anxiety and depression in routine care. J Affect Disord 338: 121-128. https://doi.org/10.1016/j.jad.2023.06.008
|
| [53] |
Morgan C, Mason E, Newby JM, et al. (2017) The effectiveness of unguided internet cognitive behavioural therapy for mixed anxiety and depression. Internet Interv 10: 47-53. https://doi.org/10.1016/j.invent.2017.10.003
|
| [54] |
Akbay AS (2018) How does spousal support affect women's quality of life in the postpartum period in Turkish culture?. Asian Women 34: 29-45. https://doi.org/10.14431/aw.2018.09.34.3.2
|
| [55] |
Stoll CRT, Izadi S, Fowler S, et al. (2019) The value of a second reviewer for study selection in systematic reviews. Res Synth Methods 10: 539-545. https://doi.org/10.1002/jrsm.1369
|
Figures(1) / Tables(2)

Siti Roshaidai Mohd Arifin, Amalia Kamaruddin, Noor Azimah Muhammad, Mohd Said Nurumal, Hazwani Mohd Mohadis, Nik Hazlina Nik Hussain, Shanti Wardaningsih. An evaluation of digital intervention for perinatal depression and anxiety: A systematic review[J]. AIMS Public Health, 2024, 11(2): 499-525. doi: 10.3934/publichealth.2024025







 DownLoad:
DownLoad: