Among medical students, depression, anxiety, and stress (DAS) are key public wellbeing challenges that require epidemiological research. We aimed to evaluate potential sources of these psychological disturbances and assess the contribution of academic and non-academic life stressors in psychological morbidity among medical students.
This exploratory questionnaire-based survey was conducted in a Saudi Arabian public sector medical college. A total of 231 medical students were enrolled and completed the depression, anxiety, and stress scale-21 (DASS-21) questionnaire.
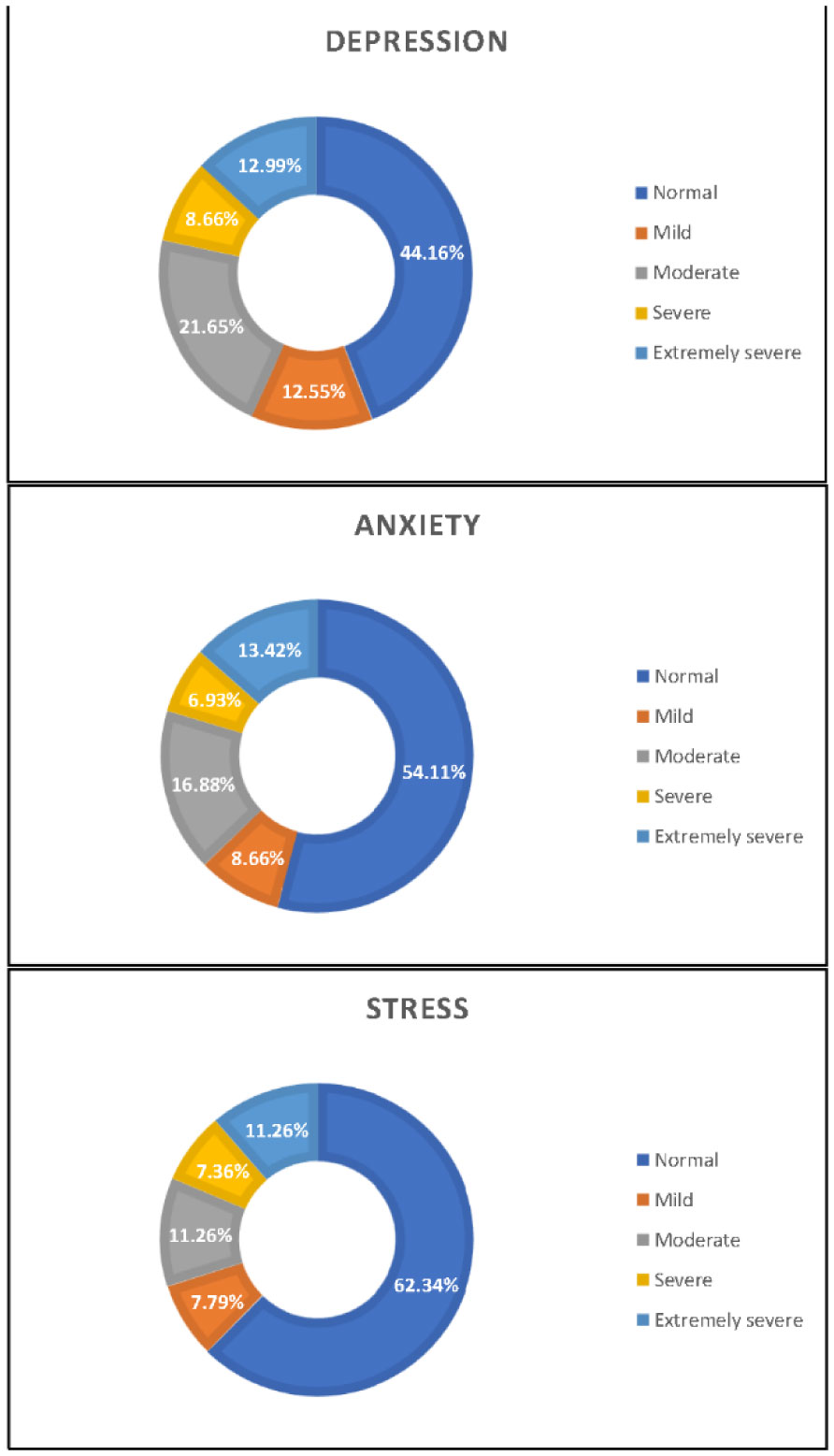
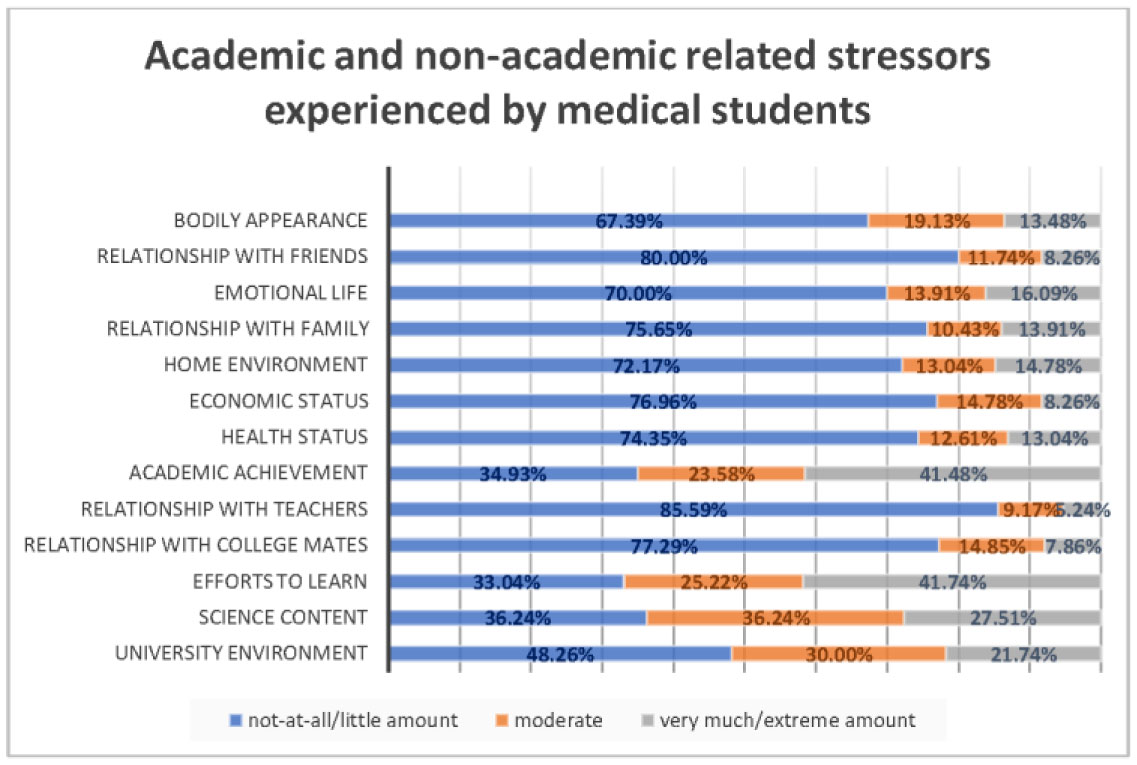
More than half of the medical students, 129 (55.8%), had depression, 106 (45.9%) students had anxiety, and 87 (37.7%) students had stress. Academic achievement was the largest explanatory factor for depression and stress, whereas bodily appearance constituted the largest explanatory factor of anxiety among the study sample. Academic and non-academic stressors score was significantly associated with depression (adjusted Odds Ratio, aOR = 1.13, 95% CI 1.07–1.19), anxiety (aOR = 1.07, 95% CI 1.03–1.12), and stress (aOR = 1.12, 95% CI 1.08–1.17).
Medical students have a high incidence of negative emotional states. These negative psychological states were explained by academic achievement and bodily appearance. The studied stressors influenced medical students' psychological wellbeing.
Citation: Ahmad A Mirza, Hammam Baarimah, Mukhtiar Baig, Abdulrahim A Mirza, Mohammed A Halawani, Ghada M Beyari, Khalid S AlRaddadi, Mahmoud Alreefi. Academic and non-academic life stressors and their impact on psychological wellbeing of medical students[J]. AIMS Public Health, 2021, 8(4): 563-580. doi: 10.3934/publichealth.2021046
Among medical students, depression, anxiety, and stress (DAS) are key public wellbeing challenges that require epidemiological research. We aimed to evaluate potential sources of these psychological disturbances and assess the contribution of academic and non-academic life stressors in psychological morbidity among medical students.
This exploratory questionnaire-based survey was conducted in a Saudi Arabian public sector medical college. A total of 231 medical students were enrolled and completed the depression, anxiety, and stress scale-21 (DASS-21) questionnaire.
More than half of the medical students, 129 (55.8%), had depression, 106 (45.9%) students had anxiety, and 87 (37.7%) students had stress. Academic achievement was the largest explanatory factor for depression and stress, whereas bodily appearance constituted the largest explanatory factor of anxiety among the study sample. Academic and non-academic stressors score was significantly associated with depression (adjusted Odds Ratio, aOR = 1.13, 95% CI 1.07–1.19), anxiety (aOR = 1.07, 95% CI 1.03–1.12), and stress (aOR = 1.12, 95% CI 1.08–1.17).
Medical students have a high incidence of negative emotional states. These negative psychological states were explained by academic achievement and bodily appearance. The studied stressors influenced medical students' psychological wellbeing.

| [1] |
Stanley N, Manthorpe J (2001) Responding to students' mental health needs: Impermeable systems and diverse users. J Ment Health 10: 41-52. doi: 10.1080/09638230020023606

|
| [2] |
Dyrbye LN, Thomas MR, Shanafelt TD (2006) Systematic review of depression, anxiety, and other indicators of psychological distress among U.S. and Canadian medical students. Acad Med 81: 354-373. doi: 10.1097/00001888-200604000-00009
|
| [3] |
Guthrie EA, Black D, Shaw CM, et al. (1997) Psychological Stress in Medical Students: A Comparison of Two Very Different University Courses. Stress Med 13: 179-184. doi: 10.1002/(SICI)1099-1700(199707)13:3<179::AID-SMI740>3.0.CO;2-E
|
| [4] | Sherina MS, Rampal L, Kaneson N (2004) Psychological stress among undergraduate medical students. Med J Malaysia 59: 207-211. |
| [5] | GBD 2015 Disease and Injury Incidence and Prevalence Collaborators (2016) Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet 388: 1545-1602. |
| [6] |
Ibrahim AK, Kelly SJ, Adams CE, et al. (2013) A systematic review of studies of depression prevalence in university students. J Psychiatr Res 47: 391-400. doi: 10.1016/j.jpsychires.2012.11.015
|
| [7] |
Ludwig AB, Burton W, Weingarten J, et al. (2015) Depression and stress amongst undergraduate medical students. BMC Med Educ 15: 141. doi: 10.1186/s12909-015-0425-z
|
| [8] |
Alharbi H, Almalki A, Alabdan F, et al. (2018) Depression among medical students in Saudi medical colleges: a cross-sectional study. Adv Med Educ Pract 9: 887-891. doi: 10.2147/AMEP.S182960
|
| [9] |
Albajjar MA, Bakarman MA (2019) Prevalence and correlates of depression among male medical students and interns in Albaha University, Saudi Arabia. J Family Med Prim Care 8: 1889-1894. doi: 10.4103/jfmpc.jfmpc_323_19
|
| [10] |
Aboalshamat K, Hou XY, Strodl E (2015) Psychological well-being status among medical and dental students in Makkah, Saudi Arabia: a cross-sectional study. Med Teach 37: S75-S81. doi: 10.3109/0142159X.2015.1006612
|
| [11] |
Hamasha AA, Kareem YM, Alghamdi MS, et al. (2019) Risk indicators of depression among medical, dental, nursing, pharmacology, and other medical science students in Saudi Arabia. Int Rev Psychiatr 31: 646-652. doi: 10.1080/09540261.2019.1584095
|
| [12] |
AlShamlan NA, AlShamlan RA, AlShamlan AA, et al. (2020) Prevalence of depression and its associated factors among clinical-year medical students in Eastern Province, Saudi Arabia. Postgrad Med J 96: 343-348. doi: 10.1136/postgradmedj-2020-137578
|
| [13] |
Khanagar SB, Al-Ehaideb A, Jamleh A, et al. (2021) Psychological Distress among Undergraduate Dental Students in Saudi Arabia and Its Coping Strategies-A Systematic Review. Healthcare (Basel) 9: 429. doi: 10.3390/healthcare9040429
|
| [14] |
AlJaber MI (2020) The prevalence and associated factors of depression among medical students of Saudi Arabia: A systematic review. J Family Med Prim Care 9: 2608-2614. doi: 10.4103/jfmpc.jfmpc_255_20
|
| [15] |
Hope V, Henderson M (2014) Medical student depression, anxiety and distress outside North America: a systematic review. Med Educ 48: 963-979. doi: 10.1111/medu.12512
|
| [16] | Ibrahim N, Al-Kharboush D, El-Khatib L, et al. (2013) Prevalence and Predictors of Anxiety and Depression among Female Medical Students in King Abdulaziz University, Jeddah, Saudi Arabia. Iran J Public Health 42: 726-736. |
| [17] | Inam SB (2007) Anxiety and Depression among Students of a Medical College in Saudi Arabia. Int J Health Sci (Qassim) 1: 295-300. |
| [18] | Alahmadi AM (2019) Prevalence of Anxiety Among College and School Students in Saudi Arabia: A systematic review. J Health Inf Dev Countries 13. |
| [19] |
Nuqali A, Al Nazzawi H, Felmban S, et al. (2018) Assessing the Correlation between Medical Students' Psychological Distress and Their Academic Performance in Makkah, Saudi Arabia. Creative Educ 09: 1332-1341. doi: 10.4236/ce.2018.99099
|
| [20] | Shadid A, Shadid AM, Shadid A, et al. (2020) Stress, Burnout, and Associated Risk Factors in Medical Students. Cureus 12: e6633. |
| [21] |
Gazzaz ZJ, Baig M, Al Alhendi BSM, et al. (2018) Perceived stress, reasons for and sources of stress among medical students at Rabigh Medical College, King Abdulaziz University, Jeddah, Saudi Arabia. BMC Med Educ 18: 29. doi: 10.1186/s12909-018-1133-2
|
| [22] | Kulsoom B, Afsar NA (2015) Stress, anxiety, and depression among medical students in a multiethnic setting. Neuropsychiatr Dis Treat 11: 1713-1722. |
| [23] |
Bramness JG, Fixdal TC, Vaglum P (1991) Effect of medical school stress on the mental health of medical students in early and late clinical curriculum. Acta Psychiatr Scand 84: 340-345. doi: 10.1111/j.1600-0447.1991.tb03157.x
|
| [24] |
Stewart SM, Betson C, Lam TH, et al. (1997) Predicting stress in first year medical students: a longitudinal study. Med Educ 31: 163-168. doi: 10.1111/j.1365-2923.1997.tb02560.x
|
| [25] |
Tyssen R, Vaglum P, Grønvold NT, et al. (2001) Factors in medical school that predict postgraduate mental health problems in need of treatment. A nationwide and longitudinal study. Med Educ 35: 110-120. doi: 10.1046/j.1365-2923.2001.00770.x
|
| [26] | El-Gilany AH, Amr M, Hammad S (2008) Perceived stress among male medical students in Egypt and Saudi Arabia: effect of sociodemographic factors. Ann Saudi Med 28: 442-448. |
| [27] |
Abdulghani HM, AlKanhal AA, Mahmoud ES, et al. (2011) Stress and its effects on medical students: a cross-sectional study at a college of medicine in Saudi Arabia. J Health Popul Nutr 29: 516-522. doi: 10.3329/jhpn.v29i5.8906
|
| [28] |
Alzahrani AM, Hakami A, AlHadi A, et al. (2020) The interplay between mindfulness, depression, stress and academic performance in medical students: A Saudi perspective. PLoS One 15: e0231088. doi: 10.1371/journal.pone.0231088
|
| [29] |
Bahhawi TA, Albasheer OB, Makeen AM, et al. (2018) Depression, anxiety, and stress and their association with khat use: a cross-sectional study among Jazan University students, Saudi Arabia. Neuropsychiatr Dis Treat 14: 2755-2761. doi: 10.2147/NDT.S182744
|
| [30] |
Aboalshamat K, Jawhari A, Alotibi S, et al. (2017) Relationship of self-esteem with depression, anxiety, and stress among dental and medical students in Jeddah, Saudi Arabia. J Int Med Dent 4: 61-68. doi: 10.18320/JIMD/201704.0261
|
| [31] |
Beiter R, Nash R, McCrady M, et al. (2015) The prevalence and correlates of depression, anxiety, and stress in a sample of college students. J Affect Disord 173: 90-96. doi: 10.1016/j.jad.2014.10.054
|
| [32] |
Shaikh BT, Kahloon A, Kazmi M, et al. (2004) Students, stress and coping strategies: a case of Pakistani medical school. Educ Health (Abingdon) 17: 346-353. doi: 10.1080/13576280400002585
|
| [33] |
Dyrbye LN, Thomas MR, Huntington JL, et al. (2006) Personal life events and medical student burnout: a multicenter study. Acad Med 81: 374-384. doi: 10.1097/00001888-200604000-00010
|
| [34] |
Dyrbye LN, Thomas MR, Harper W, et al. (2009) The learning environment and medical student burnout: a multicentre study. Med Educ 43: 274-282. doi: 10.1111/j.1365-2923.2008.03282.x
|
| [35] |
Santen SA, Holt DB, Kemp JD, et al. (2010) Burnout in medical students: examining the prevalence and associated factors. South Med J 103: 758-763. doi: 10.1097/SMJ.0b013e3181e6d6d4
|
| [36] |
Crawford JR, Henry JD (2003) The Depression Anxiety Stress Scales (DASS): normative data and latent structure in a large non-clinical sample. Br J Clin Psychol 42: 111-131. doi: 10.1348/014466503321903544
|
| [37] | Lovibond SH, Lovibond PF (1995) Manual for the depression anxiety stress scales (2nd ed.) Sydney: Psychology Foundation. |
| [38] |
Sinclair SJ, Siefert CJ, Slavin-Mulford JM, et al. (2012) Psychometric evaluation and normative data for the depression, anxiety, and stress scales-21 (DASS-21) in a nonclinical sample of U.S. adults. Eval Health Prof 35: 259-279. doi: 10.1177/0163278711424282
|
| [39] |
Daza P, Novy DM, Stanley MA, et al. (2002) The Depression Anxiety Stress Scale-21: Spanish Translation and Validation with a Hispanic Sample. J Psychopathol Behav Assess 24: 195-205. doi: 10.1023/A:1016014818163
|
| [40] |
Byrne DG, Davenport SC, Mazanov J (2007) Profiles of adolescent stress: the development of the adolescent stress questionnaire (ASQ). J Adolesc 30: 393-416. doi: 10.1016/j.adolescence.2006.04.004
|
| [41] | Abdel Wahed WY, Hassan SK (2017) Prevalence and associated factors of stress, anxiety and depression among medical Fayoum University students. Alex J Med 53: 77-84. |
| [42] |
Iqbal S, Gupta S, Venkatarao E (2015) Stress, anxiety and depression among medical undergraduate students and their socio-demographic correlates. Indian J Med Res 141: 354-357. doi: 10.4103/0971-5916.156571
|
| [43] | Azim SR, Baig M (2019) Frequency and perceived causes of depression, anxiety and stress among medical students of a private medical institute in Karachi: a mixed method study. J Pak Med Assoc 69: 840-845. |
| [44] |
Rehman R, Fatima K, Hussain M, et al. (2021) Association between depression and health risk behaviors among university students, Karachi, Pakistan. Cogent Psychology 8: 1886626. doi: 10.1080/23311908.2021.1886626
|
| [45] |
Oku A, Owoaje E, Oku O, et al. (2015) Prevalence of stress, stressors and coping strategies among medical students in a Nigerian medical school. Afr J Med Health Sci 14: 29-34. doi: 10.4103/2384-5589.153384
|
| [46] |
Niemi PM, Vainiomaki PT (2006) Medical students' distress--quality, continuity and gender differences during a six-year medical programme. Med Teach 28: 136-141. doi: 10.1080/01421590600607088
|
| [47] | Sharifirad G, Marjani A, Abdolrahman C, et al. (2012) Stress among Isfahan medical sciences students. J Res Med Sci 17: 402-406. |
| [48] |
Mirza AA, Baig M, Beyari GM, et al. (2021) Depression and Anxiety Among Medical Students: A Brief Overview. Adv Med Educ Pract 12: 393-398. doi: 10.2147/AMEP.S302897
|
| [49] |
Yusoff MSB, Yee LY, Wei LH, et al. (2011) A study on stress, stressors and coping strategies among Malaysian medical students. Int J Stud Res 1: 45-50. doi: 10.5549/IJSR.1.2.45-50
|
| [50] |
Yeh YC, Yen CF, Lai CS, et al. (2007) Correlations between Academic Achievement and Anxiety and Depression in Medical Students Experiencing Integrated Curriculum Reform. Kaohsiung J Med Sci 23: 379-386. doi: 10.1016/S0257-5655(07)70001-9
|
| [51] | Yusoff MSB, Rahim AFA, Yaacob MJ (2011) The Prevalence of Final Year Medical Students with Depressive Symptoms and Its Contributing Factors. Int Med J 18: 305-309. |
| [52] |
Saravanan C, Wilks R (2014) Medical students' experience of and reaction to stress: the role of depression and anxiety. Scientific World J 2014: 737382. doi: 10.1155/2014/737382
|
| [53] |
Liao Y, Knoesen NP, Deng Y, et al. (2010) Body dysmorphic disorder, social anxiety and depressive symptoms in Chinese medical students. Soc Psychiatry Psychiatr Epidemiol 45: 963-971. doi: 10.1007/s00127-009-0139-9
|
| [54] |
Taqui AM, Shaikh M, Gowani SA, et al. (2008) Body Dysmorphic Disorder: gender differences and prevalence in a Pakistani medical student population. BMC Psychiatr 8: 20. doi: 10.1186/1471-244X-8-20
|
| [55] |
Behere SP, Yadav R, Behere PB (2011) A comparative study of stress among students of medicine, engineering, and nursing. Indian J Psychol Med 33: 145-148. doi: 10.4103/0253-7176.92064
|
| [56] |
Tahir M, Butt MW, Gul S, et al. (2020) Factors contributing to stress and anxiety in undergraduate medical students. Professional Med J 27: 2769-2774. doi: 10.29309/TPMJ/2020.27.12.4598
|
| [57] |
Dunn LB, Iglewicz A, Moutier C (2008) A conceptual model of medical student well-being: promoting resilience and preventing burnout. Acad Psychiatr 32: 44-53. doi: 10.1176/appi.ap.32.1.44
|
| [58] | Rehman R, Katpar S, Hussain M, et al. (2017) A comparison between wellness awareness among medical students. J Pak Med Assoc 67: 196-199. |
Figures(2) / Tables(6)

Ahmad A Mirza, Hammam Baarimah, Mukhtiar Baig, Abdulrahim A Mirza, Mohammed A Halawani, Ghada M Beyari, Khalid S AlRaddadi, Mahmoud Alreefi. Academic and non-academic life stressors and their impact on psychological wellbeing of medical students[J]. AIMS Public Health, 2021, 8(4): 563-580. doi: 10.3934/publichealth.2021046







 DownLoad:
DownLoad: