Corneal blindness is the fourth leading cause of blindness worldwide, with 10 million people having bilateral corneal blindness, nearly 80% of all corneal blindness cases are avoidable and are reversible. Corneal transplantation (CT) is the most frequently performed type of transplant across the world. This review was conducted with the objective of identifying if it is safe to harvest the cornea from the patients died due to COVID-19 and preventing the chances of transmission from donor to the recipient or healthcare worker handling the harvested cornea. A total of 45 articles were found with the keywords and out of all, only 16 fulfilled the inclusion criteria. RT-PCR is the technique of choice for detection of virus in the corpse and the sample analyzed was a pharyngeal swab. Available literature states unavailability of sufficient evidence-based studies proving presence of virus in the cornea or tear of COVID affected patients There is no proven consensus on presence of Virus in cornea. It is important to follow preferred practice guidelines so as to restart eye banking and do at least the emergency surgeries without having risk of disease transmission and keeping ourselves safe.
Citation: Anuj Kumar Pandey, Nidhi Mudgil, Yogesh Wadgave, Sidharth Sekhar Mishra. Corneal transplantation during COVID-19 pandemic: need for special considerations—A live review[J]. AIMS Public Health, 2021, 8(2): 186-195. doi: 10.3934/publichealth.2021014
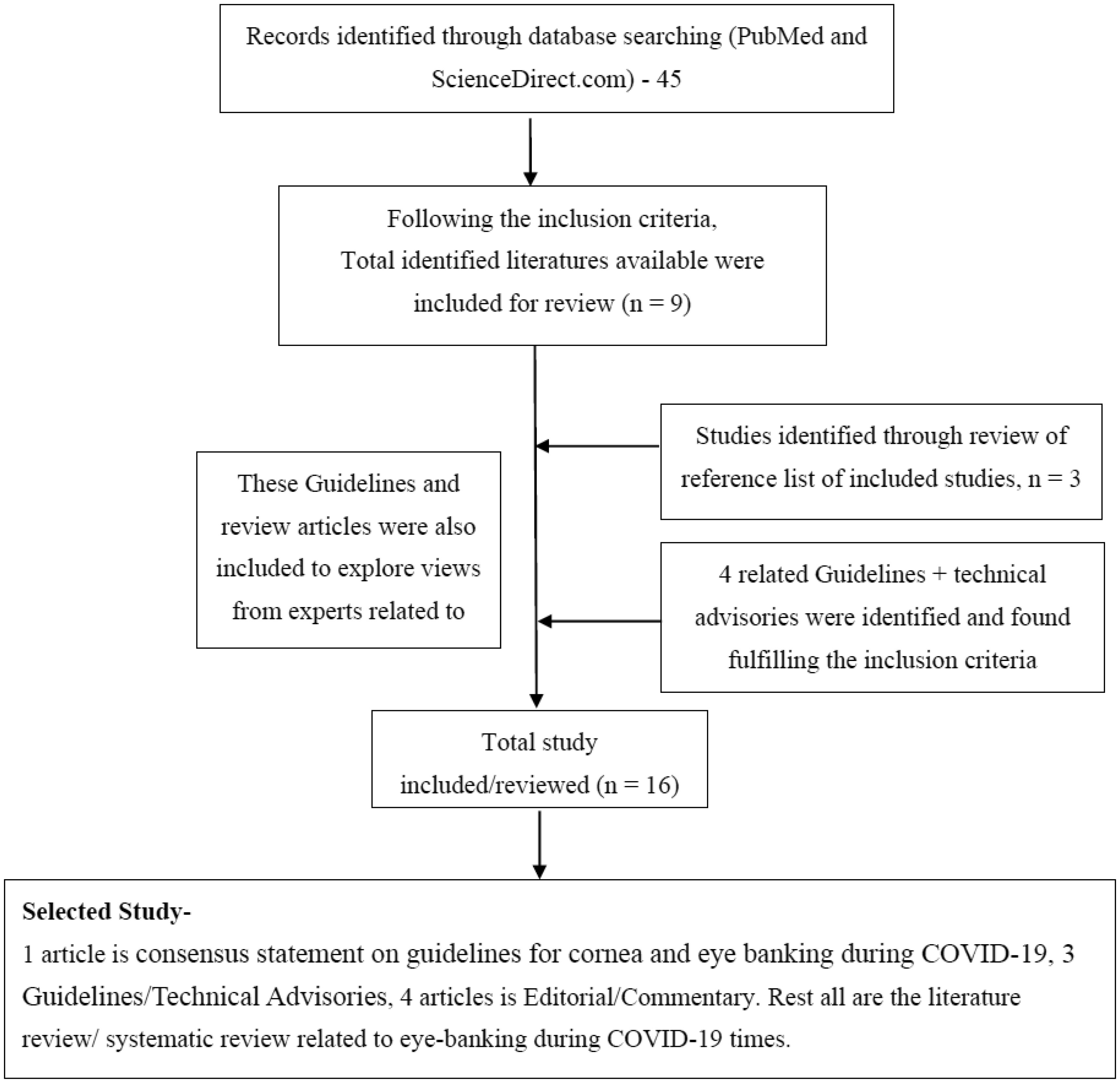
Corneal blindness is the fourth leading cause of blindness worldwide, with 10 million people having bilateral corneal blindness, nearly 80% of all corneal blindness cases are avoidable and are reversible. Corneal transplantation (CT) is the most frequently performed type of transplant across the world. This review was conducted with the objective of identifying if it is safe to harvest the cornea from the patients died due to COVID-19 and preventing the chances of transmission from donor to the recipient or healthcare worker handling the harvested cornea. A total of 45 articles were found with the keywords and out of all, only 16 fulfilled the inclusion criteria. RT-PCR is the technique of choice for detection of virus in the corpse and the sample analyzed was a pharyngeal swab. Available literature states unavailability of sufficient evidence-based studies proving presence of virus in the cornea or tear of COVID affected patients There is no proven consensus on presence of Virus in cornea. It is important to follow preferred practice guidelines so as to restart eye banking and do at least the emergency surgeries without having risk of disease transmission and keeping ourselves safe.

| [1] |
Gain P, Jullienne R, He Z, et al. (2016) Global Survey of Corneal Transplantation and Eye Banking. JAMA Ophthalmol 134: 167. doi: 10.1001/jamaophthalmol.2015.4776

|
| [2] |
Singh R, Gupta N, Vanathi M, et al. (2019) Corneal transplantation in the modern era. Indian J Med Res 150: 7. doi: 10.4103/ijmr.IJMR_141_19
|
| [3] |
Toro M, Choragiewicz T, Posarelli C, et al. (2020) European COVID-19 Cataract Group (#EUROCOVCAT). Early Impact of COVID-19 Outbreak on the Availability of Cornea Donors: Warnings and Recommendations. Clin Ophthalmol Auckl NZ 14: 2879-2882. doi: 10.2147/OPTH.S260960
|
| [4] |
Williams KA, Muehlberg SM, Lewis RF, et al. (1995) How successful is corneal transplantation? A report from the Australian Corneal Graft Register. Eye (Lond) 9: 219-227. doi: 10.1038/eye.1995.43
|
| [5] |
Verma R, Khanna P, Prinja S, et al. (2011) The National Programme for Control of Blindness in India. Australas Med J 4: 1-3. doi: 10.4066/AMJ.2011.646
|
| [6] |
Jose R, Rathore A, Rajshekar V, et al. (2009) Salient features of the National Program for Control of Blindness during the XI th five-year plan period. Indian J Ophthalmol 57: 339. doi: 10.4103/0301-4738.55064
|
| [7] | National health policy (2017) .Available from: https://www.nhp.gov.in/nhpfiles/national_health_policy_2017.pdf. |
| [8] | World Health Organization Coronavirus disease (COVID-19) Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019. |
| [9] | Ministry of Health and Family Welfare, Government of India Available from: https://www.mohfw.gov.in/. |
| [10] |
Sharma N, D'Souza S, Nathawat R, et al. (2020) All India Ophthalmological Society - Eye Bank Association of India consensus statement on guidelines for cornea and eyebanking during COVID-19 era. Indian J Ophthalmol 68: 1258. doi: 10.4103/ijo.IJO_1554_20
|
| [11] | Desautels JD, Moshirfar M, Martheswaran T, et al. (2020) Risks Posed to Corneal Transplant Recipients by COVID-19-Affected Donors. Ophthalmol Ther 6: 1-9. |
| [12] | World Health Organization Coronavirus Disease (COVID-19) Dashboard Available from: https://covid19.who.int/table. |
| [13] | Sawant OB, Singh S, Write RE, et al. (2020) Prevalence of SARS-CoV-2 in human post-mortem ocular tissues. medRxiv Available from: https://www.medrxiv.org/content/10.1101/2020.10.05.20201574v1. |
| [14] |
Roy A, Das S, Chaurasia S, et al. (2020) Corneal transplantation and eye banking practices during COVID-19-related lockdown period in India from a network of tertiary eye care centers. Indian J Ophthalmol 68: 2368. doi: 10.4103/ijo.IJO_2258_20
|
| [15] |
Fernández-Rodríguez A, Casas I, Culebras E, et al. (2020) COVID-19 and post-mortem microbiological studies. Span J Leg Med 46: 127-138. doi: 10.1016/j.remle.2020.05.007
|
| [16] | Global Alliance of Eye Banking Association Coronavirus (COVID-2019) and Ocular Tissue Donation November 2020 Available from: http://www.gaeba.org/wp-content/uploads/2020/11/GAEBA-COVID19-Alert-up-date-November-2020.pdf. |
| [17] | Llywodraeth Cymru Welsh Government Welsh Government COVID-19 Technical Advisory Group Consensus Statement: Post-mortem testing Available from: https://gov.wales/sites/default/files/publications/2020-07/technical-advisory-group-consensus-statement-post-mortem-testing.pdf. |
| [18] | Guidelines on Post Mortem Testing for Natural Deaths Available from: https://www.nicd.ac.za/wp-content/uploads/2020/10/Guidelines-on-Post-Mortem-Testing-for-Natural-Deaths_2020_Final_signed_20201013.pdf. |
| [19] |
Ang M, Moriyama A, Colby K, et al. (2020) Corneal transplantation in the aftermath of the COVID-19 pandemic: an international perspective. Br J Ophthalmol 104: bjophthalmol-2020-317013. doi: 10.1136/bjophthalmol-2020-317013
|
| [20] |
Amesty MA, Alió del Barrio JL, Alió JL (2020) COVID-19 Disease and Ophthalmology: An Update. Ophthalmol Ther 22: 1-12. doi: 10.1007/s40123-020-00260-y
|
| [21] |
Chaurasia S, Sharma N, Das S (2020) COVID-19 and eye banking. Indian J Ophthalmol 68: 1215-1216. doi: 10.4103/ijo.IJO_1033_20
|
| [22] |
Ballouz D, Mian SI (2020) Eye banking in the coronavirus disease 2019 era. Curr Opin Ophthalmol 31: 389-395. doi: 10.1097/ICU.0000000000000684
|
| [23] | Kates OS, Fisher CE, Rakita RM, et al. (2020) Use of SARS-CoV-2 infected deceased organ donors: Should we always “just say no?”. Am J Transplant 20. |
| [24] | Mukhra R, Krishan K, Kanchan T (2020) Possible modes of transmission of Novel coronavirus SARS-CoV-2: a review. Acta Bio-Medica Atenei Parm 91: e2020036. |
| [25] |
Sharma N, D'Souza S, Nathawat R, et al. (2020) All India Ophthalmological Society - Eye Bank Association of India consensus statement on guidelines for cornea and eyebanking during COVID-19 era. Indian J Ophthalmol 68: 1258-1262. doi: 10.4103/ijo.IJO_1554_20
|
| [26] |
Siedlecki J, Brantl V, Schworm B, et al. (2020) COVID-19: Ophthalmological Aspects of the SARS-CoV 2 Global Pandemic. Klin Monatsbl Augenheilkd 237: 675-680. doi: 10.1055/a-1164-9381
|
| [27] |
Sharma N, Arora T, Singhal D, et al. (2019) Procurement, storage and utilization trends of eye banks in India. Indian J Ophthalmol 67: 1056. doi: 10.4103/ijo.IJO_1551_18
|
| [28] | Guideline for Eye Care Available from: https://www.mohfw.gov.in/pdf/GuidelineforEyeCare.pdf. |
Figures(1) / Tables(1)

Anuj Kumar Pandey, Nidhi Mudgil, Yogesh Wadgave, Sidharth Sekhar Mishra. Corneal transplantation during COVID-19 pandemic: need for special considerations—A live review[J]. AIMS Public Health, 2021, 8(2): 186-195. doi: 10.3934/publichealth.2021014







 DownLoad:
DownLoad: