Citation: Fazle Khuda, Nur Najmi Mohamad Anuar, Badiah Baharin, Nurrul Shaqinah Nasruddin. A mini review on the associations of matrix metalloproteinases (MMPs) -1, -8, -13 with periodontal disease[J]. AIMS Molecular Science, 2021, 8(1): 13-31. doi: 10.3934/molsci.2021002

| [1] |
Beck JD, Philips K, Moss K, et al. (2020) Periodontal disease classifications and incident coronary heart disease in the atherosclerosis risk in communities study. J Periodontol 91: 1409-1408. doi: 10.1002/JPER.19-0723

|
| [2] | Preethanath RS, Ibraheem WI, Anil A (2020) Pathogenesis of gingivitis. Oral Diseases 1-19. |
| [3] |
Yakob M, Meurman J, Sorsa T, et al. (2013) Treponema denticola associates with increased levels of MMP-8 and MMP-9 in gingival crevicular fluid. Oral Dis 19: 694-701. doi: 10.1111/odi.12057
|
| [4] |
Sorsa T, Ding YL, Ingman T, et al. (2016) Cellular source, activation and inhibition of dental plaque collagenase. J Clin Periodontol 22: 709-717. doi: 10.1111/j.1600-051X.1995.tb00831.x
|
| [5] | Dom TNM, Ayob R, Abd Muttalib K, et al. (2016) National economic burden sssociated with management of periodontitis in Malaysia. Int J Dent Article ID 1891074. |
| [6] | Nazir M, Al-Ansari A, Al-Khalifa K, et al. (2020) Global prevalence of periodontal disease and lack of its surveillance. Sci World J Article ID 2146160. |
| [7] | Dyke TEV, Dave S (2006) Risk factors for periodontitis. J Int Acad Periodontol 7: 3-7. |
| [8] |
Charles K, Honibald E, Palani A, et al. (2014) Role of matrix metalloproteinases (MMPs) in periodontitis and its management. J Indian Acad Dent Spec Res 1: 65-69. doi: 10.4103/2229-3019.148262
|
| [9] |
Ye S (2015) Putative targeting of matrix metalloproteinase-8 in atherosclerosis. Pharmacol Ther 147: 111-122. doi: 10.1016/j.pharmthera.2014.11.007
|
| [10] |
Zhang Z, Yang X, Zhang H, et al. (2018) The role of ECM metalloproteinase inducer glycosylation in regulating matrix metalloproteinases in periodontitis. J Periodontal Res 53: 391-402. doi: 10.1111/jre.12524
|
| [11] |
Rangasamy L, Di Geronimo B, Ortín I, et al. (2019) Molecular imaging probes based on matrix metalloproteinase inhibitors (MMPIs). Molecules 24: 2982. doi: 10.3390/molecules24162982
|
| [12] | Anuar NNM, Zulkafali NIN, Ugusman A (2020) Modulation of matrix metalloproteinases by plant-derived products. Curr Cancer Drug Targets PMID 33222671. |
| [13] |
Letra A, Silva RM, Rylands RJ, et al. (2012) MMP-3 and TIMP-1 variants contribute to chronic periodontitis and may be implicated in disease progression. J Clin Periodontol 39: 707-716. doi: 10.1111/j.1600-051X.2012.01902.x
|
| [14] |
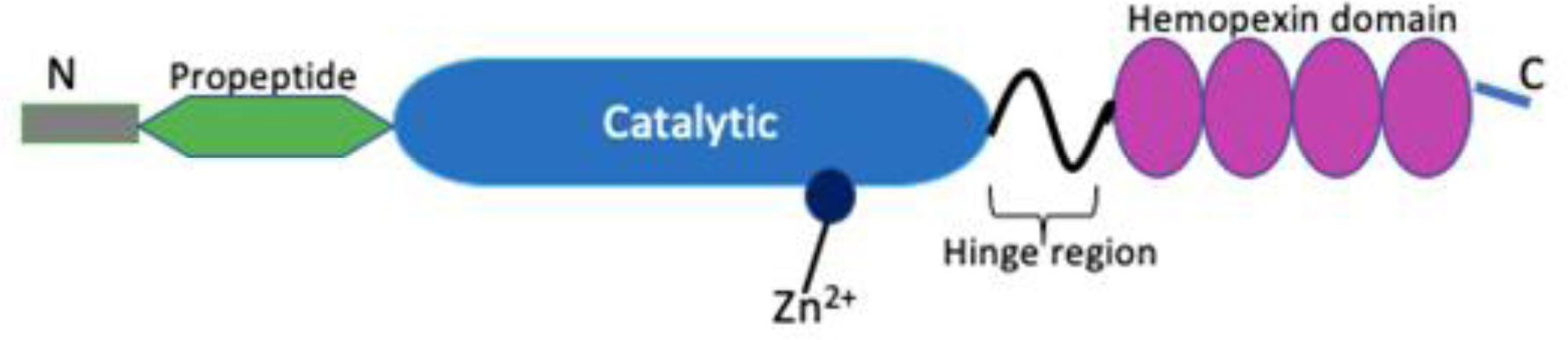
Caldeira J, Laronha H (2020) Structure and function of human matrix metalloproteinases. Cells 9: 1076. doi: 10.3390/cells9051076
|
| [15] |
Checchi V, Maravic T, Bellini P, et al. (2020) The role of matrix metalloproteinases in periodontal disease. Int J Environ Res Public Health 17: 1-13. doi: 10.3390/ijerph17144923
|
| [16] |
Gonzalez-Avila G, Sommer B, Mendoza-Posada DA, et al. (2019) Matrix metalloproteinases participation in the metastatic process and their diagnostic and therapeutic applications in cancer. Crit Rev Oncol Hematol 137: 57-83. doi: 10.1016/j.critrevonc.2019.02.010
|
| [17] |
Hannas AR, Pereira JC, Granjeiro JM, et al. (2007) The role of matrix metalloproteinases in the oral environment. Acta Odontol Scand 65: 1-13. doi: 10.1080/00016350600963640
|
| [18] |
Verma RP, Hansch C (2007) Matrix metalloproteinases (MMPs): chemical-biological functions and (Q)SARs. Bioorg Med Chem 15: 2223-2268. doi: 10.1016/j.bmc.2007.01.011
|
| [19] |
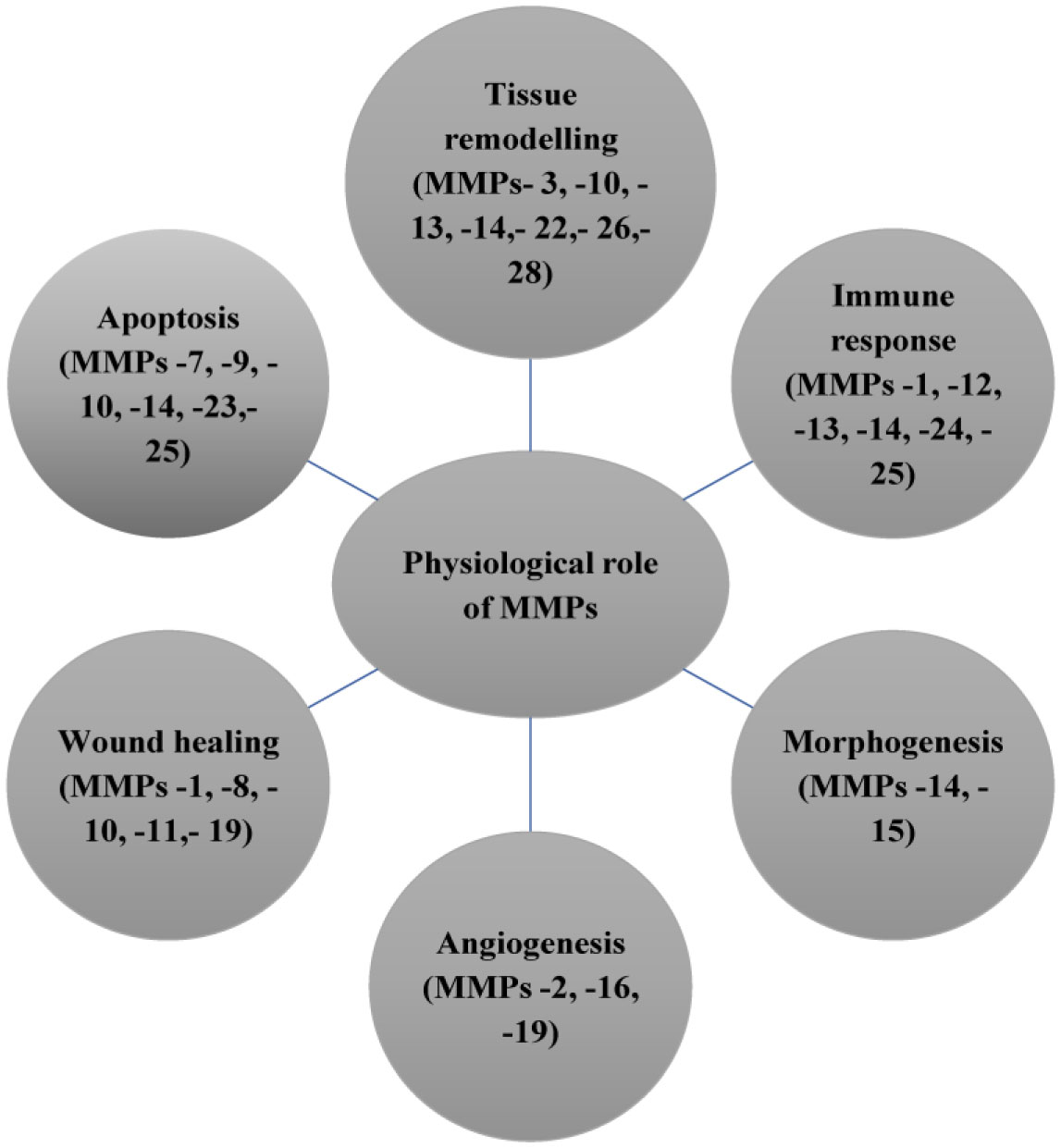
Klein T, Bischoff R (2011) Physiology and pathophysiology of matrix metalloproteases. Amino Acids 41: 271-290. doi: 10.1007/s00726-010-0689-x
|
| [20] |
Nagase H, Visse R, Murphy G (2006) Structure and function of matrix metalloproteinases and TIMPs. Cardiovasc Res 69: 562-573. doi: 10.1016/j.cardiores.2005.12.002
|
| [21] | Cui N, Hu M, Khalil RA (2017) Biochemical and biological attributes of matrix metalloproteinases. Progress in Molecular Biology and Translational Science Elsevier Inc. |
| [22] |
Pérez-García S, Carrión M, Gutiérrez-Cañas I, et al. (2019) Profile of matrix-remodeling proteinases in osteoarthritis: Impact of fibronectin. Cells 9: 40. doi: 10.3390/cells9010040
|
| [23] |
Sapna G, Gokul S (2013) Matrix metalloproteinases and periodontal diseases. Oral Dis 20: 538-550. doi: 10.1111/odi.12159
|
| [24] | Franco C, Patricia HR, Timo S, et al. (2017) Matrix metalloproteinases as regulators of periodontal inflammation. Int J Mol Sci 18: 1-12. |
| [25] |
Verstappen J, Hoff JWVD (2006) Critical reviews in oral biology and medicine tissue inhibitors of metalloproteinases (TIMPs). J Dent Res 85: 1074-1084. doi: 10.1177/154405910608501202
|
| [26] |
Visse R, Nagase H (2003) Matrix metalloproteinases and tissue inhibitors of metalloproteinases: Structure, function, and biochemistry. Circ Res 92: 827-839. doi: 10.1161/01.RES.0000070112.80711.3D
|
| [27] |
Lahdentausta LSJ, Paju S, Mäntylä P, et al. (2018) Saliva and serum biomarkers in periodontitis and coronary artery disease. J Clin Periodontol 45: 1045-1055. doi: 10.1111/jcpe.12976
|
| [28] | Li W, Zhu Y, Singh P, et al. (2016) Association of common variants in MMPs with periodontitis risk. Dis Markers 2016: 1-20. |
| [29] |
Yamamoto K, Okano H, Miyagawa W, et al. (2015) MMP-13 is constitutively produced in human chondrocytes and co-endocytosed with ADAMTS-5 and TIMP-3 by the endocytic receptor LRP1. Matrix Biol 56: 57-73. doi: 10.1016/j.matbio.2016.03.007
|
| [30] | Chow YY, Chin KY (2020) The Role of Inflammation in the Pathogenesis of Osteoarthritis. Mediat Inflamm Article ID 8293921. |
| [31] | Navjot KP, Nisha KJ, Sanjeela GSP (2018) Role of matrixmetalloproteinases in periodontal disease - A Review. Biomed J Sci Tech Res 2: 2099. |
| [32] |
Pardo A, Selman M (2005) MMP-1: The elder of the family. Int J Biochem Cell Biol 37: 283-288. doi: 10.1016/j.biocel.2004.06.017
|
| [33] | Chang YT, Chu LJ, Liu YC, et al. (2020) Verification of saliva matrix metalloproteinase-1 as a strong diagnostic marker of oral cavity cancer. Cancers (Basel) 12: 1-18. |
| [34] | Balli U, Cetinkaya BO, Keles GC, et al. (2016) Assessment of MMP-1, MMP-8 and TIMP-2 in experimental periodontitis treated with kaempferol. JPIS 46: 84-95. |
| [35] |
Wang J, Yang D, Li C, et al. (2014) Expression of ECM metalloproteinase inducer glycosylation and caveolin-1 in healthy and inflamed human gingiva. J Periodontal Res 49: 197-204. doi: 10.1111/jre.12095
|
| [36] |
Hazzaa H, Abo Hager E (2017) Expression of MMP-1 and MMP-9 in localized aggressive periodontitis patients before and after treatment: A clinical and immunohistochemical study. Egypt Dent J 63: 667-684. doi: 10.21608/edj.2017.75015
|
| [37] |
Popat RP, Bhavsar NV, Popat PR (2014) Gingival crevicular fluid levels of matrix metalloproteinase-1 (MMP-1) and tissue inhibitor of metalloproteinase-1 (TIMP-1) in periodontal health and disease. Singapore Dent J 35: 59-64. doi: 10.1016/j.sdj.2014.07.003
|
| [38] |
Ghodpage PS, Kolte RA, Kolte AP, et al. (2014) Influence of phase I periodontal therapy on levels of matrix metalloproteinase 1 and tissue inhibitor of metalloproteinase 1. Saudi Dent J 26: 171-175. doi: 10.1016/j.sdentj.2014.05.003
|
| [39] |
Beklen A (2017) Effects of IL-13 on TGF-β and MMP-1 in periodontitis. Biotech Histochem 92: 374-380. doi: 10.1080/10520295.2017.1312526
|
| [40] |
Nokhbehsaim M, Nogueira AVB, Damanaki A, et al. (2020) Regulation of matrix metalloproteinase-1 by filifactor alocis in human gingival and monocytic cells. Clin Oral Investig 24: 1987-1995. doi: 10.1007/s00784-019-03062-0
|
| [41] |
Sorsa T, Gursoy UK, Nwhator S, et al. (2016) Analysis of matrix metalloproteinases, especially MMP-8, in gingival creviclular fluid, mouthrinse and saliva for monitoring periodontal diseases. Periodontology 2000 70: 142-163. doi: 10.1111/prd.12101
|
| [42] |
Kraft-Neumärker M, Lorenz K, Koch R, et al. (2012) Full-mouth profile of active MMP-8 in periodontitis patients. J Periodontal Res 47: 121-128. doi: 10.1111/j.1600-0765.2011.01416.x
|
| [43] | Sorsa T, Alassiri S, Grigoriadis A, et al. (2020) Active MMP-8 (AMMP-8) as a grading and staging biomarker in the periodontitis classification. Diagnostics (Basel) 10: 1-10. |
| [44] |
Juurikka K, Butler GS, Salo T, et al. (2019) The role of MMP-8 in cancer: A systematic review. Int J Mol Sci 20: 1-27. doi: 10.3390/ijms20184506
|
| [45] |
Lenglet S, Mach F, Montecucco F (2013) Role of matrix metalloproteinase-8 in atherosclerosis. Mediat Inflamm 2013: 659282. doi: 10.1155/2013/659282
|
| [46] |
Yakob M, Kari K, Tervahartiala T, et al. (2012) Associations of periodontal microorganisms with salivary proteins and MMP-8 in gingival crevicular fluid. J Clin Periodontol 39: 256-263. doi: 10.1111/j.1600-051X.2011.01813.x
|
| [47] |
Honibald E, Mathew S, Padmanaban J, et al. (2012) Perioceutics: Matrix metalloproteinase inhibitors as an adjunctive therapy for inflammatory periodontal disease. J Pharm Bioallied Sci 4: 417-421. doi: 10.4103/0975-7406.100315
|
| [48] |
Leppilahti JM, Ahonen MM, Hernández M, et al. (2011) Oral rinse MMP-8 point-of-care immuno test identifies patients with strong periodontal inflammatory burden. Oral Dis 17: 115-122. doi: 10.1111/j.1601-0825.2010.01716.x
|
| [49] |
Rathnayake N, Gieselmann DR, Heikkinen A, et al. (2017) Salivary diagnostics point-of-care diagnostics of MMP-8 in dentistry and medicine. Diagnostics (Basel) 7: 7. doi: 10.3390/diagnostics7010007
|
| [50] |
Munhoz F, Branco F, Souza R, et al. (2019) MMP-13 polymorphism as a risk factor in implant loss. Int J Oral Maxillofac Implant 34: 768-771. doi: 10.11607/jomi.7057
|
| [51] |
Virtanen E, Yakob M, Tervahartiala T, et al. (2017) Salivary MMP-13 gender differences in periodontitis: A cross-sectional study from Sweden. Clin Exp Dent Res 3: 165-170. doi: 10.1002/cre2.76
|
| [52] |
Choi JY, Fuerst R, Knapinska AM, et al. (2017) Structure-based design and synthesis of potent and selective matrix metalloproteinase-13 inhibitors. J Med Chem 60: 5816-5825. doi: 10.1021/acs.jmedchem.7b00514
|
| [53] |
Stura EA, Visse R, Cuniasse P, et al. (2013) Crystal structure of full-length human collagenase 3 (MMP-13) with peptides in the active site defines exosites in the catalytic domain. FASEB J 27: 4395-4405. doi: 10.1096/fj.13-233601
|
| [54] |
Leppilahti JM, Hernández-Ríos PA, Gamonal JA, et al. (2014) Matrix metalloproteinases and myeloperoxidase in gingival crevicular fluid provide site-specific diagnostic value for chronic periodontitis. J Clin Periodontol 41: 348-356. doi: 10.1111/jcpe.12223
|
| [55] |
Gursoy UK, Könönen E, Huumonen S, et al. (2013) Salivary type i collagen degradation end-products and related matrix metalloproteinases in periodontitis. J Clin Periodontol 40: 18-25. doi: 10.1111/jcpe.12020
|
| [56] | Aleksandrowicz P, Zelechowska P, Agier J, et al. (2017) Evaluation of metalloproteinase-8 levels in crevicular fluid of patients with healthy implants or periodontitis. Mediat Inflamm Article ID 4920847. |
| [57] |
Pawar DD, Mehta DS (2015) Effect of phase 1 periodontal therapy on gingival crevicular fluid levels of matrix metalloproteinases-3 and -13 in chronic periodontitis patients. J Investig Clin Dent 6: 118-124. doi: 10.1111/jicd.12072
|
| [58] |
Räisänen IT, Sorsa T, Schoor G, et al. (2019) Active matrix metalloproteinase-8 Point-Of-Care (POC)/chairside mouthrinse test vs. bleeding on probing in diagnosing subclinical periodontitis in adolescents. Diagnostics 9: 6-11. doi: 10.3390/diagnostics9010034
|
| [59] | Alassiri S, Parnanen P, Rathnayake N, et al. (2018) The ability of quantitative, specific, and sensitive point-of-care/chair-side oral fluid immunotests for aMMP-8 to detect periodontal and peri-implant diseases. Dis Markers Article ID 1306396. |
| [60] |
Srivastava N, Nayak PA, Rana S (2017) Point of care- A novel approach to periodontal diagnosis-A review. J Clin Diagnostic Res 11: 1-6. doi: 10.1111/crj.12541
|
| [61] |
Räisänen I, Heikkinen A, Siren E, et al. (2018) Point-of-care/chairside aMMP-8 analytics of periodontal diseases' Activity and Episodic Progression. Diagnostics 8: 74. doi: 10.3390/diagnostics8040074
|
| [62] |
Heikkinen AM, Nwhator SO, Rathnayake N, et al. (2015) Pilot study on oral health status as assessed by an active matrix metalloproteinase-8 chairside mouthrinse test in adolescents. J Periodontol 87: 36-40. doi: 10.1902/jop.2015.150377
|
| [63] | Raivisto T, Sorsa T, Räisänen I, et al. (2020) Active matrix metalloproteinase-8 chair side mouth rinse test, health behaviour and oral Health in finnish adolescent cohort. J Clin Diagnostic Res 35-39. |
| [64] |
Rautava J, Gursoy U, Kullstrom A, et al. (2020) An oral rinse active matrix metalloproteinase-8 point-of-care immunotest may be less accurate in patients with crohn's disease. Biomolecules 10: 395. doi: 10.3390/biom10030395
|
| [65] | Pajnigara NG, Kolte AP, Kolte RA, et al. (2016) Chair side diagnostic kits in periodontics. IDJSR 4: 25-31. |
| [66] | Hamodat HF, Taha MYM (2020) Estimation of salivary MMP-8, MMP-9, MMP-13 and TIMP-1 in chronic periodontitis in Mosul. IJDSR 8: 22-26. |
| [67] |
Özcan E, Işıl Saygun N, Serdar MA, et al. (2016) Non-surgical periodontal therapy reduces saliva adipokine and matrix metalloproteinase levels in periodontitis. J Periodontol 87: 934-943. doi: 10.1902/jop.2016.160046
|
| [68] | Keles Yucel ZP, Afacan B, Emingil G, et al. (2020) Local and systemic levels of aMMP-8 in gingivitis and stage 3 grade C periodontitis. J Periodontal Res 1-8. |
| [69] |
Sorsa T, Hernández M, Leppilahti J, et al. (2010) Detection of gingival crevicular fluid MMP-8 levels with different laboratory and chair-side methods. Oral Dis 16: 39-45. doi: 10.1111/j.1601-0825.2009.01603.x
|
| [70] |
Gonçalves PF, Huang H, McAninley S, et al. (2013) Periodontal treatment reduces matrix metalloproteinase levels in localized aggressive periodontitis. J Periodontol 84: 1801-1808. doi: 10.1902/jop.2013.130002
|
| [71] |
Leppilahti JM, Kallio MA, Tervahartiala T, et al. (2014) Gingival crevicular fluid matrix metalloproteinase-8 levels predict treatment outcome among smokers with chronic periodontitis. J Periodontol 85: 250-260. doi: 10.1902/jop.2013.130156
|
Figures(3) / Tables(4)

Fazle Khuda, Nur Najmi Mohamad Anuar, Badiah Baharin, Nurrul Shaqinah Nasruddin. A mini review on the associations of matrix metalloproteinases (MMPs) -1, -8, -13 with periodontal disease[J]. AIMS Molecular Science, 2021, 8(1): 13-31. doi: 10.3934/molsci.2021002







 DownLoad:
DownLoad: