Knee medial compartment osteoarthritis is effectively treated by a medial open-wedge high tibial osteotomy (MOWHTO). The feasibility and safety of MOWHTO for mild lateral meniscal tears are unknown. This study examined the feasibility and safety of knee joint weight-bearing line ratio (WBLr) adjustment during MOWHTO with lateral meniscal injuries. We used a healthy adult male's lower extremities computed tomography scans and knee joint magnetic resonance imaging images to create a normal fine element (FE) model. Based on this model, we generated nine FE models for the MOWHTO operation (WBLr: 40–80%) and 15 models for various lateral meniscal injuries. A compressive load of 650N was applied to all cases to calculate the von Mises stress (VMS), and the intact lateral meniscus' maximal VMS at 77.5% WBLr was accepted as the corrective upper limit stress. Our experimental results show that mild lateral meniscal tears can withstand MOWHTO, while severe tears cannot. Our findings expand the use of MOWHTO and provide a theoretical direction for practical decisions in patients with lateral meniscal injuries.
Citation: Lin Chen, Mingjun Wang, Zhanyu Wu, Jinbo Sun, Jianglong Li, Chun Chen, Chuan Ye. Advancements in health informatics: finite element insights into medial open-wedge high tibial osteotomy and lateral meniscal tears[J]. Mathematical Biosciences and Engineering, 2024, 21(4): 5394-5410. doi: 10.3934/mbe.2024237
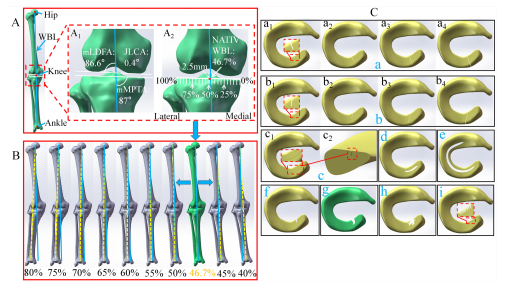
Knee medial compartment osteoarthritis is effectively treated by a medial open-wedge high tibial osteotomy (MOWHTO). The feasibility and safety of MOWHTO for mild lateral meniscal tears are unknown. This study examined the feasibility and safety of knee joint weight-bearing line ratio (WBLr) adjustment during MOWHTO with lateral meniscal injuries. We used a healthy adult male's lower extremities computed tomography scans and knee joint magnetic resonance imaging images to create a normal fine element (FE) model. Based on this model, we generated nine FE models for the MOWHTO operation (WBLr: 40–80%) and 15 models for various lateral meniscal injuries. A compressive load of 650N was applied to all cases to calculate the von Mises stress (VMS), and the intact lateral meniscus' maximal VMS at 77.5% WBLr was accepted as the corrective upper limit stress. Our experimental results show that mild lateral meniscal tears can withstand MOWHTO, while severe tears cannot. Our findings expand the use of MOWHTO and provide a theoretical direction for practical decisions in patients with lateral meniscal injuries.

| [1] |
L. N. Reynard, M. J. Barter, Osteoarthritis year in review 2019: Genetics, genomics and epigenetics, Osteoarthritis Cartilage, 28 (2020), 275–284. http://doi.org/10.1016/j.joca.2019.11.010 doi: 10.1016/j.joca.2019.11.010

|
| [2] |
D. J. Hunter, S. Bierma-Zeinstra, Osteoarthritis, Lancet, 393 (2019), 1745–1759. http://doi.org/10.1016/S0140-6736(19)30417-9 doi: 10.1016/S0140-6736(19)30417-9
|
| [3] |
J. W. Bijlsma, F. Berenbaum, F. P. Lafeber, Osteoarthritis: an update with relevance for clinical practice, Lancet, 377 (2011), 2115–2126. http://doi.org/10.1016/S0140-6736(11)60243-2 doi: 10.1016/S0140-6736(11)60243-2
|
| [4] |
Q. Liu, S. Wang, J. Lin, Y. Zhang, The burden for knee osteoarthritis among Chinese elderly: estimates from a nationally representative study, Osteoarthritis Cartilage, 26 (2018), 1636–1642. http://doi.org/10.1016/j.joca.2018.07.019 doi: 10.1016/j.joca.2018.07.019
|
| [5] |
S. Safiri, A. Kolahi, E. Smith, C. Hill, D. Bettampadi, M. A. Mansournia, et al., Global, regional and national burden of osteoarthritis 1990–2017: A systematic analysis of the Global Burden of Disease Study 2017, Ann. Rheum. Dis., 79 (2020), 819–828. http://doi.org/10.1136/annrheumdis-2019-216515 doi: 10.1136/annrheumdis-2019-216515
|
| [6] |
J. C. Stoddart, O. Dandridge, A. Garner, J. Cobb, R. J. van Arkel, The compartmental distribution of knee osteoarthritis-a systematic review and meta-analysis, Osteoarthritis Cartilage, 29 (2021), 445–455. http://doi.org/10.1016/j.joca.2020.10.011 doi: 10.1016/j.joca.2020.10.011
|
| [7] |
C. Jacquet, F. Gulagaci, A. Schmidt, A. Pendse, S. Parratte, J. Argenson, et al., Opening wedge high tibial osteotomy allows better outcomes than unicompartmental knee arthroplasty in patients expecting to return to impact sports, Knee Surg. Sports Traumatol. Arthroscopy, 28 (2020), 3849–3857. http://doi.org/10.1007/s00167-020-05857-1 doi: 10.1007/s00167-020-05857-1
|
| [8] |
A. Agarwalla, D. R. Christian, J. N. Liu, G. H. Garcia, M. L. Redondo, A. B. Yanke, et al., Return to work following isolated opening wedge high tibial osteotomy, Cartilage, 12 (2021), 468–474. http://doi.org/10.1177/1947603519852417 doi: 10.1177/1947603519852417
|
| [9] |
M. Loia, S. Vanni, F. Rosso, D. Bonasia, M. Bruzzone, F. Dettoni, et al., High tibial osteotomy in varus knees: Indications and limits, Joints, 4 (2016), 98–110. http://doi.org/10.11138/jts/2016.4.2.098 doi: 10.11138/jts/2016.4.2.098
|
| [10] |
B. Zampogna, S. Vasta, R. Papalia, Patient evaluation and indications for osteotomy around the knee, Clin. Sports Med., 38 (2019), 305–315. http://doi.org/10.1016/j.csm.2019.02.011 doi: 10.1016/j.csm.2019.02.011
|
| [11] |
D. H. Kim, S. C. Kim, J. S. Yoon, Y. S. Lee, Are there harmful effects of preoperative mild lateral or patellofemoral degeneration on the outcomes of open wedge high tibial osteotomy for medial compartmental osteoarthritis?, Orthop. J. Sports Med., 8 (2020). http://doi.org/10.1177/2325967120927481 doi: 10.1177/2325967120927481
|
| [12] |
C. Jin, E. Song, A. Santoso, P. S. Ingale, I. Choi, J. Seon, Survival and risk factor analysis of medial open wedge high tibial osteotomy for unicompartment knee osteoarthritis, J. Arthroscopic Relat. Surg., 36 (2020), 535–543. http://doi.org/10.1016/j.arthro.2019.08.040 doi: 10.1016/j.arthro.2019.08.040
|
| [13] |
R. S. Khakha, H. R. B. A. Razak, K. Kley, R. van Heerwaarden, A. J. Wilson, Role of high tibial osteotomy in medial compartment osteoarthritis of the knee: Indications, surgical technique and outcomes, J. Clin. Orthop. Trauma, 23 (2021), 101618. http://doi.org/10.1016/j.jcot.2021.101618 doi: 10.1016/j.jcot.2021.101618
|
| [14] |
J. L. Martay, A. J. Palmer, N. K. Bangerter, S. Clare, A. P. Monk, C. P. Brown, et al., A preliminary modeling investigation into the safe correction zone for high tibial osteotomy, Knee, 25 (2018), 286–295. http://doi.org/10.1016/j.knee.2017.12.006 doi: 10.1016/j.knee.2017.12.006
|
| [15] | Z. Trad, A. Barkaoui, M. Chafra, J. M. R. Tavares, Finite element analysis of the effect of high tibial osteotomy correction angle on articular cartilage loading, in Proceedings of the Institution of Mechanical Engineers, Part H: Journal of Engineering in Medicine, 232 (2018), 553–564. http://doi.org/10.1177/0954411918770706 |
| [16] |
Y. Dong, G. Hu, Y. Dong, Y. Hu, Q. Xu, The effect of meniscal tears and resultant partial meniscectomies on the knee contact stresses: a finite element analysis, Comput. Methods Biomech. Biomed. Eng., 17 (2013), 1452–1463. http://doi.org/10.1080/10255842.2012.753063 doi: 10.1080/10255842.2012.753063
|
| [17] |
L. Li, L. Yang, K. Zhang, L. Zhu, X. Wang, Q. Jiang, Three-dimensional finite-element analysis of aggravating medial meniscus tears on knee osteoarthritis, J. Orthop. Transl., 20 (2020), 47–55. http://doi.org/10.1016/j.jot.2019.06.007 doi: 10.1016/j.jot.2019.06.007
|
| [18] |
P. Jiang, J. Cui, Z. Chen, Z. Dai, Y. Zhang, G. Yi, Biomechanical study of medial meniscus after posterior horn injury: a finite element analysis, Comput. Methods Biomech. Biomed. Eng., 23 (2020), 127–137. http://doi.org/10.1080/10255842.2019.1702167 doi: 10.1080/10255842.2019.1702167
|
| [19] |
B. P. Nguyen, C. Chui, S. Ong, S. Chang, An efficient compression scheme for 4-D medical images using hierarchical vector quantization and motion compensation, Comput. Biol. Med., 41 (2011), 843–856. http://doi.org/10.1016/j.compbiomed.2011.07.003 doi: 10.1016/j.compbiomed.2011.07.003
|
| [20] |
Q. H. Nguyen, B. P. Nguyen, M. T. Nguyen, M. C. H. Chua, T. T. T. Do, N. Nghiem, Bone age assessment and sex determination using transfer learning, Expert Syst. Appl., 200 (2022), 116926. http://doi.org/10.1016/j.eswa.2022.116926 doi: 10.1016/j.eswa.2022.116926
|
| [21] |
X. Chen, B. P. Nguyen, C. Chui, S. Ong, An automatic framework for multi-label brain tumor segmentation based on kernel sparse representation, Acta Polytech. Hung., 14 (2017). http://doi.org/10.12700/aph.14.1.2017.1.3 doi: 10.12700/aph.14.1.2017.1.3
|
| [22] |
S. Lu, B. Yang, Y. Xiao, S. Liu, M. Liu, L. Yin, et al., Iterative reconstruction of low-dose CT based on differential sparse, Biomed. Signal Process. Control, 79 (2023), 104204. http://doi.org/10.1016/j.bspc.2022.104204 doi: 10.1016/j.bspc.2022.104204
|
| [23] |
L. Cai, W. Tay, B. P. Nguyen, C. Chui, S. Ong, Automatic transfer function design for medical visualization using visibility distributions and projective color mapping, Comput. Med. Imaging Graphics, 37 (2013), 450–458. http://doi.org/10.1016/j.compmedimag.2013.08.008 doi: 10.1016/j.compmedimag.2013.08.008
|
| [24] |
Y. Xu, F. Zhang, W. Zhai, S. Cheng, J. Li, Y. Wang, Unraveling of advances in 3D-printed polymer-based bone scaffolds, Polymers, 14 (2022), 566. http://doi.org/10.3390/polym14030566 doi: 10.3390/polym14030566
|
| [25] |
S. Su, J. He, C. Wang, F. Gao, D. Zhong, P. Lei, A new dressing system reduces the number of dressing changes in the primary total knee arthroplasty: A randomized controlled trial, Front. Surg., 9 (2022). http://doi.org/10.3389/fsurg.2022.800850 doi: 10.3389/fsurg.2022.800850
|
| [26] |
Y. Miao, X. Wang, S. Wang, R. Li, Adaptive switching control based on dynamic zero-moment point for versatile hip exoskeleton under hybrid locomotion, IEEE Trans. Ind. Electron., 70 (2023), 11443–11452. http://doi.org/10.1109/TIE.2022.3229343 doi: 10.1109/TIE.2022.3229343
|
| [27] |
Y. Chen, J. Xiang, Z. Wang, Y. Xiao, D. Zhang, X. Chen, et al., Associations of bone mineral density with lean mass, fat mass, and dietary patterns in postmenopausal chinese women: A 2-year prospective study, PLOS ONE, 10 (2015), 0137097. http://doi.org/10.1371/journal.pone.0137097 doi: 10.1371/journal.pone.0137097
|
| [28] |
N. M. Luís, R. Varatojo, Radiological assessment of lower limb alignment, Efort Open Rev., 6 (2021), 487–494. http://doi.org/10.1302/2058-5241.6.210015 doi: 10.1302/2058-5241.6.210015
|
| [29] |
D. M. Allen, L. Li, M. D. Crema, M. D. Marra, A. Guermazi, B. T. Wyman, et al., The relationship between meniscal tears and meniscal position, Ther. Adv. Musculoskeletal Dis., 2 (2010), 315–323. http://doi.org/10.1177/1759720X10383198 doi: 10.1177/1759720X10383198
|
| [30] |
M. E. Wells, J. P. Scanaliato, J. C. Dunn, E. J. Garcia, Meniscal injuries: Mechanism, classification, Sports Med. Arthroscopy Rev., 29 (2021), 154–157. http://doi.org/10.1097/JSA.0000000000000311 doi: 10.1097/JSA.0000000000000311
|
| [31] |
P. Beaufils, R. Becker, S. Kopf, O. Matthieu, N. Pujol, The knee meniscus: management of traumatic tears and degenerative lesions, Efort Open Rev., 2 (2017), 195–203. http://doi.org/10.1302/2058-5241.2.160056 doi: 10.1302/2058-5241.2.160056
|
| [32] |
K. Ding, W. Yang, H. Wang, S. Zhan, P. Hu, J. Bai, et al., Finite element analysis of biomechanical effects of residual varus/valgus malunion after femoral fracture on knee joint, Int. Orthop., 45 (2021), 1827–1835. http://doi.org/10.1007/s00264-021-05039-9 doi: 10.1007/s00264-021-05039-9
|
| [33] |
H. R. C. Bao, D. Zhu, G. S. Gu, H. Gong, The effect of complete radial lateral meniscus posterior root tear on the knee contact mechanics: a finite element analysis, J. Orthop. Sci., 18 (2013), 256–263. http://doi.org/10.1007/s00776-012-0334-5 doi: 10.1007/s00776-012-0334-5
|
| [34] |
T. Kozaki, D. Fukui, E. Yamamoto, D. Nishiyama, M. Yamanaka, A. Murata, et al., Medial meniscus extrusion and varus tilt of joint line convergence angle increase stress in the medial compartment of the knee joint in the knee extension position-finite element analysis-, J. Exp. Orthop., 9 (2022). http://doi.org/10.1186/s40634-022-00490-y doi: 10.1186/s40634-022-00490-y
|
| [35] |
C. Pan, X. Wang, L. Ding, X. Zhu, W. Xu, L. Huang, The best position of bone grafts in the medial open-wedge high tibial osteotomy: A finite element analysis, Comput. Methods Programs Biomed., 228 (2023), 107253. http://doi.org/10.1016/j.cmpb.2022.107253 doi: 10.1016/j.cmpb.2022.107253
|
| [36] |
A. E. Kedgley, T. Saw, N. A. Segal, U. N. Hansen, A. M. J. Bull, S. D. Masouros, Predicting meniscal tear stability across knee-joint flexion using finite-element analysis, Knee Surg. Sports Traumatol. Arthroscopy, 27 (2019), 206–214. http://doi.org/10.1007/s00167-018-5090-4 doi: 10.1007/s00167-018-5090-4
|
| [37] |
Y. Wu, X. Jin, X. Zhao, Y. Wang, H. Bai, B. Lu, et al., Computer-aided design of distal femoral osteotomy for the valgus knee and effect of correction angle on joint loading by finite element analysis, Orthop. Surg., 14 (2022), 2904–2913. http://doi.org/10.1111/os.13440 doi: 10.1111/os.13440
|
| [38] |
B. Ollivier, P. Berger, C. Depuydt, H. Vandenneucker, Good long-term survival and patient-reported outcomes after high tibial osteotomy for medial compartment osteoarthritis, Knee Surg. Sports Traumatol. Arthroscopy, 29 (2020), 3569–3584. http://doi.org/10.1007/s00167-020-06262-4 doi: 10.1007/s00167-020-06262-4
|
| [39] |
M. Englund, A. Guermazi, S. L. Lohmander, The role of the meniscus in knee osteoarthritis: A cause or consequence?, Radiol. Clin., 47 (2009), 703–712. http://doi.org/10.1016/j.rcl.2009.03.003 doi: 10.1016/j.rcl.2009.03.003
|
| [40] |
J. B. Guimaraes, M. C. Nevitt, C. E. McCulloch, B. J. Schwaiger, A. S. Gersing, L. Facchetti, et al., Association of weight change with progression of meniscal intrasubstance degeneration over 48 months: Data from the Osteoarthritis Initiative, Eur. Radiol., 28 (2017), 953–962. http://doi.org/10.1007/s00330-017-5054-y doi: 10.1007/s00330-017-5054-y
|
| [41] |
M. A. Wesdorp, S. M. Eijgenraam, D. E. Meuffels, S. M. A. Bierma-Zeinstra, G. Kleinrensink, Y. M. Bastiaansen-Jenniskens, et al., Traumatic meniscal tears are associated with meniscal degeneration, Am. J. Sports Med., 48 (2020), 2345–2352. http://doi.org/10.1177/0363546520934766 doi: 10.1177/0363546520934766
|
| [42] |
R. J. Ward, J. B. Driban, J. W. MacKay, T. E. McAlindon, B. Lu, C. B. Eaton, et al., Meniscal degeneration is prognostic of destabilzing meniscal tear and accelerated knee osteoarthritis: Data from the osteoarthritis initiative, J. Orthop. Res., 41 (2023), 2418–2423. http://doi.org/10.1002/jor.25575 doi: 10.1002/jor.25575
|
| [43] |
J. Moore, L. Mychaltchouk, F. Lavoie, Applicability of a modified angular correction measurement method for open-wedge high tibial osteotomy, Knee Surg. Sports Traumatol. Arthroscopy, 25 (2016), 846–852. http://doi.org/10.1007/s00167-015-3954-4 doi: 10.1007/s00167-015-3954-4
|
| [44] |
K. Briem, D. K. Ramsey, W. Newcomb, K. S. Rudolph, L. Snyder-Mackler, Effects of the amount of valgus correction for medial compartment knee osteoarthritis on clinical outcome, knee kinetics and muscle co‐contraction after opening wedge high tibial osteotomy, J. Orthop. Res., 25 (2007), 311–318. http://doi.org/10.1002/jor.20326 doi: 10.1002/jor.20326
|
| [45] |
Y. Yin, S. Li, R. Zhang, J. Guo, Z. Hou, Y. Zhang, What is the relationship between the "fujisawa point" and postoperative knee valgus angle? A theoretical, computer-based study, Knee, 27 (2020), 183–191. http://doi.org/10.1016/j.knee.2019.10.018 doi: 10.1016/j.knee.2019.10.018
|
| [46] |
X. Liu, Z. Chen, Y. Gao, J. zhang, Z. Jin, High tibial osteotomy: Review of techniques and biomechanics, J. Healthcare Eng., 2019 (2019), 8363128. http://doi.org/10.1155/2019/8363128 doi: 10.1155/2019/8363128
|







Figures(8)

Lin Chen, Mingjun Wang, Zhanyu Wu, Jinbo Sun, Jianglong Li, Chun Chen, Chuan Ye. Advancements in health informatics: finite element insights into medial open-wedge high tibial osteotomy and lateral meniscal tears[J]. Mathematical Biosciences and Engineering, 2024, 21(4): 5394-5410. doi: 10.3934/mbe.2024237







 DownLoad:
DownLoad: