Non-invasive fetal ECG (NI-FECG) provides a non-invasive method to monitor the health of the fetus. However, the NI-FECG is easily interfered by noise, which makes the signal quality decline, leading to the fetal heart rate (FHR) monitoring becoming a challenging task.
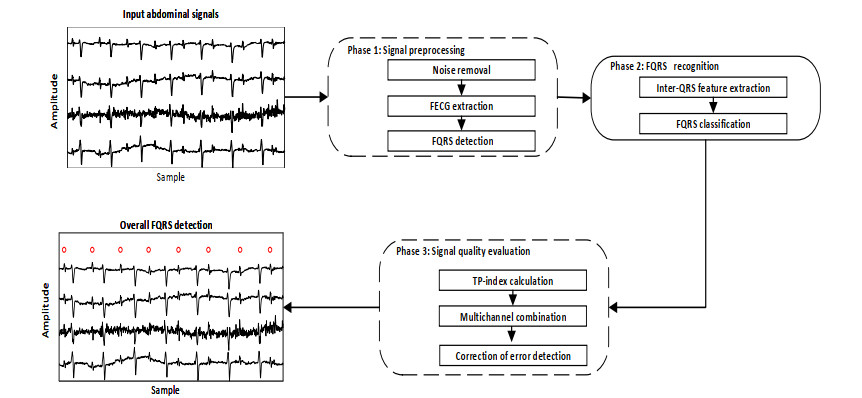
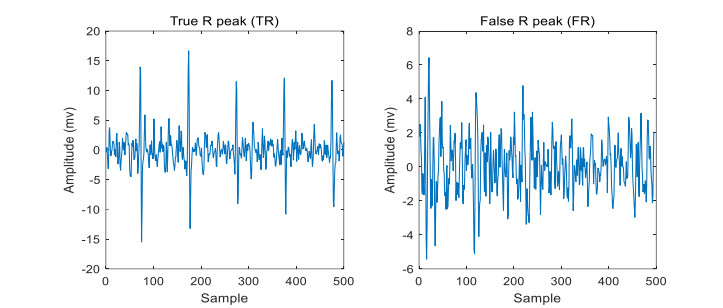
In this work, an algorithm for dynamic evaluation of signal quality is proposed to improve the multi-channel FHR monitoring. The innovation of the method is to assess the signal quality in the process of multi-channel fetal QRS (FQRS) complexes detection. Specifically, the detected FQRS is used as quality unit. Each quality unit can be a true R peak (TR) or a false R peak (FR). It is the basic quality information in this work. The signal quality of each channel is estimated by estimating the correctness of the detection results. Further, the TRs of all channels can be fused to obtain more reliable fetal heart rate monitoring.
Analysis results demonstrate that the proposed algorithm is capable of selecting the good quality signal for FQRS detection achieving 97.40% $ PPV $, 98.33% $ SE $ and 97.86% $ F_1 $.
This work sheds light on the quality assessment of fetal monitoring signal.
Citation: Wei Zhong, Li Mao, Wei Du. A signal quality assessment method for fetal QRS complexes detection[J]. Mathematical Biosciences and Engineering, 2023, 20(5): 7943-7956. doi: 10.3934/mbe.2023344
Non-invasive fetal ECG (NI-FECG) provides a non-invasive method to monitor the health of the fetus. However, the NI-FECG is easily interfered by noise, which makes the signal quality decline, leading to the fetal heart rate (FHR) monitoring becoming a challenging task.
In this work, an algorithm for dynamic evaluation of signal quality is proposed to improve the multi-channel FHR monitoring. The innovation of the method is to assess the signal quality in the process of multi-channel fetal QRS (FQRS) complexes detection. Specifically, the detected FQRS is used as quality unit. Each quality unit can be a true R peak (TR) or a false R peak (FR). It is the basic quality information in this work. The signal quality of each channel is estimated by estimating the correctness of the detection results. Further, the TRs of all channels can be fused to obtain more reliable fetal heart rate monitoring.
Analysis results demonstrate that the proposed algorithm is capable of selecting the good quality signal for FQRS detection achieving 97.40% $ PPV $, 98.33% $ SE $ and 97.86% $ F_1 $.
This work sheds light on the quality assessment of fetal monitoring signal.

| [1] |
P. Mannella, L. Billeci, A. Giannini, A. Canu, F. Pancetti, T. Simoncini, et al., A feasibility study on non-invasive fetal ECG to evaluate prenatal autonomic nervous system activity, Eur. J. Obstet. Gyn. R. B., 246 (2020), 60–66. https://doi.org/10.1016/j.ejogrb.2020.01.015 doi: 10.1016/j.ejogrb.2020.01.015

|
| [2] |
E. Castillo, D. P. Morales, A. García, L. Parrilla, V. U. Ruiz, J. A. Álvarez Bermejo, A clustering-based method for single-channel fetal heart rate monitoring, PLoS One, 13 (2018), 1–22. https://doi.org/10.1371/journal.pone.0199308 doi: 10.1371/journal.pone.0199308
|
| [3] |
T. L. Yassin, A. R. Esam, Fetal ECG extraction using input-mode and output-mode adaptive filters with blind source separation, IEEE Can. J. Electr. Comput. Eng., 43 (2020), 295–304. https://doi.org/10.1109/CJECE.2020.2984602 doi: 10.1109/CJECE.2020.2984602
|
| [4] |
B. Al-Sheikh, M. S. Salman, A. Eleyan, S. Alboon, Non-invasive fetal ECG extraction using discrete wavelet transform recursive inverse adaptive algorithm, Technol. Health Care, 28 (2020), 507–520. https://doi.org/10.3233/THC-191948 doi: 10.3233/THC-191948
|
| [5] |
D. A. Ramli, Y. H. Shiong, N. Hassan, Blind source separation (bss) of mixed maternal and fetal electrocardiogram (ECG) signal: A comparative study, Procedia Comput. Sci., 176 (2020), 582–591. https://doi.org/10.1016/j.procs.2020.08.060 doi: 10.1016/j.procs.2020.08.060
|
| [6] | S. Mirza, K. Bhole, P. Singh, Fetal ECG extraction and QRS detection using independent component analysis, in 2020 16th IEEE International Colloquium on Signal Processing & Its Applications (CSPA), (2020), 157–161. https://doi.org/10.1109/CSPA48992.2020.9068696 |
| [7] |
N. Zhang, J. Zhang, H. Li, O. Mumini, O. Samuel, K. Ivanov, et al., A novel technique for fetal ECG extraction using single-channel abdominal recording, Sensors, 17 (2017), 457. https://doi.org/10.3390/s17030457 doi: 10.3390/s17030457
|
| [8] |
F. Andreotti, J. Behar, S. Zaunseder, J. Oster, G. D. Clifford, An open-source framework for stress-testing non-invasive foetal ECG extraction algorithms, Physiol. Meas., 37 (2016), 627. https://doi.org/10.1088/0967-3334/37/5/627 doi: 10.1088/0967-3334/37/5/627
|
| [9] |
C. H. N. V. S. Praneeth, J. D. K. Abel, D. Samiappan, R. Kumar, S. P. Kumar, P. V. Nitin, A comparison on variants of lms used in fir adaptive noise cancellers for fetal ECG extraction, Biomed. Eng. Appl. Basis Commun., 32 (2020), 2050026. https://doi.org/10.4015/s101623722050026x doi: 10.4015/s101623722050026x
|
| [10] |
Y. Zhang, A. Gu, Z. Xiao, Y. Xing, C. Yang, J. Li, et al., Wearable fetal ECG monitoring system from abdominal electrocardiography recording, Biosensors, 12 (2022), 475. https://doi.org/10.3390/bios12070475 doi: 10.3390/bios12070475
|
| [11] |
R. Jaros, R. Martinek, R. Kahankova, Non-adaptive methods for fetal ECG signal processing: A review and appraisal, Sensors, 18 (2018), 3648. https://doi.org/10.3390/s18113648 doi: 10.3390/s18113648
|
| [12] |
M. Jallouli, S. Arfaoui, A. B. Mabrouk, C. Cattani, Clifford wavelet entropy for fetal ECG extraction, Entropy, 23 (2021), 844. https://doi.org/10.3390/e23070844 doi: 10.3390/e23070844
|
| [13] |
G. D. Clifford, J. Behar, Q. Li, I. Rezek, Signal quality indices and data fusion for determining clinical acceptability of electrocardiograms, Physiol. Meas., 33 (2012), 1419–1433. https://doi.org/10.1088/0967-3334/33/9/1419 doi: 10.1088/0967-3334/33/9/1419
|
| [14] |
Q. Li, G. D. Clifford, Signal quality and data fusion for false alarm reduction in the intensive care unit, J. Electrocardiol., 45 (2012), 596–603. https://doi.org/10.1016/j.jelectrocard.2012.07.015 doi: 10.1016/j.jelectrocard.2012.07.015
|
| [15] |
S. Rahman, C. Karmakar, M. Palaniswami, Robustness of electrocardiogram signal quality indices, J. R. Soc. Interface, 19 (2022), 1–15. https://doi.org/10.1098/rsif.2022.0012 doi: 10.1098/rsif.2022.0012
|
| [16] |
J. Behar, J. Oster, Q. Li, G. D. Clifford, ECG signal quality during arrhythmia and its application to false alarm reduction, IEEE Trans. Biomed. Eng., 60 (2013), 1660–1666. https://doi.org/10.1109/TBME.2013.2240452 doi: 10.1109/TBME.2013.2240452
|
| [17] |
C. Orphanidou, T. Bonnici, P. Charlton, D. Clifton, D. Vallance, L. Tarassenko, Signal-quality indices for the electrocardiogram and photoplethysmogram: Derivation and applications to wireless monitoring, IEEE J. Biomed. Health Inf., 19 (2015), 832–838. https://doi.org/10.1088/0967-3334/37/4/610 doi: 10.1088/0967-3334/37/4/610
|
| [18] |
J. Behar, F. Andreotti, S. Zaunseder, Q. Li, J. Oster, G. D. Clifford, An ECG simulator for generating maternal-foetal activity mixtures on abdominal ECG recordings, Physiol. Meas., 35 (2014), 1537. https://doi.org/10.1088/0967-3334/35/8/1537 doi: 10.1088/0967-3334/35/8/1537
|
| [19] |
F. Andreotti, M. Riedl, T. Himmelsbach, D. Wedekind, N. Wessel, H. Stepan, et al., Robust fetal ECG extraction and detection from abdominal leads, Physiol. Meas., 35 (2014), 1551–1567. https://doi.org/10.1088/0967-3334/35/8/1551 doi: 10.1088/0967-3334/35/8/1551
|
| [20] |
F. Liu, C. Liu, L. Zhao, X. Jiang, Z. Zhang, J. Li, et al., Dynamic ECG signal quality evaluation based on the generalized bsqi index, IEEE Access, 6 (2018), 41892–41902. https://doi.org/10.1109/ACCESS.2018.2860056 doi: 10.1109/ACCESS.2018.2860056
|
| [21] |
M. Varanini, G. Tartarisco, L. Billeci, A. Macerata, G. Pioggia, R. Balocchi, An efficient unsupervised fetal QRS complex detection from abdominal maternal ECG, Physiol. Meas., 35 (2014), 1607–1619. https://doi.org/10.1088/0967-3334/35/8/1607 doi: 10.1088/0967-3334/35/8/1607
|
| [22] |
J. Behar, J. Oster, G. D. Clifford, Combining and benchmarking methods of foetal ECG extraction without maternal or scalp electrode data, Physiol. Meas., 35 (2014), 1569–1589. https://doi.org/10.1088/0967-3334/35/8/1569 doi: 10.1088/0967-3334/35/8/1569
|
| [23] |
F. Andreotti, F. Gräßer, H. Malberg, S. Zaunseder, Non-invasive fetal ECG signal quality assessment for multichannel heart rate estimation, IEEE Trans. Biomed. Eng., 64 (2017), 2793–2802. https://doi.org/10.1109/TBME.2017.2675543 doi: 10.1109/TBME.2017.2675543
|
| [24] |
M. J. Mollakazemi, F. Asadi, Fetal QRS detection in noninvasive abdominal electrocardiograms using principal component analysis and discrete wavelet transforms with signal quality estimation, J. Biomed. Phys. Eng., 11 (2021), 197–204. https://doi.org/10.31661/jbpe.v0i0.397 doi: 10.31661/jbpe.v0i0.397
|
| [25] |
J. Hao, Y. Yang, Z. Zhou, S. Wu, Fetal electrocardiogram signal extraction based on fast independent component analysis and singular value decomposition, Sensors, 22 (2022), 3705. https://doi.org/10.3390/s22103705 doi: 10.3390/s22103705
|
| [26] |
I. Silva, J. Behar, R. Sameni, T. Zhu, J. Oster, G. D. Clifford, et al., Noninvasive fetal ECG: the physionet/computing in cardiology challenge 2013, Comput. Cardiol., 40 (2013), 149–152. https://doi.org/10.1088/0967-3334/35/8/1521 doi: 10.1088/0967-3334/35/8/1521
|
| [27] |
J. Behar, F. Andreotti, S. Zaunseder, J. Oster, G. D. Clifford, A practical guide to non-invasive foetal electrocardiogram extraction and analysis, Physiol. Meas., 37 (2016), 1–35. https://doi.org/10.1088/0967-3334/37/5/r1 doi: 10.1088/0967-3334/37/5/r1
|
| [28] |
W. Zhong, W. Zhao, Fetal ECG extraction using short time fourier transform and generative adversarial networks, Physiol. Meas., 42 (2021), 105011. https://doi.org/10.1088/1361-6579/ac2c5b doi: 10.1088/1361-6579/ac2c5b
|
| [29] |
J. Behar, A. Johnson, G. D. Clifford, J. Oster, A comparison of single channel fetal ECG extraction methods, Ann. Biomed. Eng., 42 (2014), 1340–1353. https://doi.org/10.1007/s10439-014-0993-9 doi: 10.1007/s10439-014-0993-9
|
| [30] |
J. Pan, W. J. Tompkins, A real-time QRS detection algorithm, IEEE Trans. Biomed. Eng., 32 (1985), 230–236. https://doi.org/10.1109/tbme.1985.325532 doi: 10.1109/tbme.1985.325532
|
| [31] |
A. Esteva, B. Kuprel, R. Novoa, J. Ko, S. M. Swetter, H. M. Blau, et al., Dermatologist-level classification of skin cancer with deep neural networks, Nature, 542 (2017), 115–118. https://doi.org/10.1038/nature21056 doi: 10.1038/nature21056
|
| [32] |
W. Zhong, L. Liao, X. Guo, G. Wang, A deep learning approach for fetal QRS complex detection, Physiol. Meas., 39 (2018), 045004. https://doi.org/10.1088/1361-6579/aab297 doi: 10.1088/1361-6579/aab297
|
| [33] |
S. P. von Steinburg, A. L. Boulesteix, C. Lederer, S. Grunow, S. Schiermeier, W. Hatzmann, et al., What is the "normal" fetal heart rate, PeerJ, 1 (2013), e82. https://doi.org/10.7717/peerj.82 doi: 10.7717/peerj.82
|


Figures(9) / Tables(2)

Wei Zhong, Li Mao, Wei Du. A signal quality assessment method for fetal QRS complexes detection[J]. Mathematical Biosciences and Engineering, 2023, 20(5): 7943-7956. doi: 10.3934/mbe.2023344







 DownLoad:
DownLoad: