Hypoxia is a crucial factor in the development of esophageal cancer. The relationship between hypoxia and immune status in the esophageal cancer microenvironment is becoming increasingly important in clinical practice. This study aims to clarify and investigate the possible connection between immunotherapy and hypoxia in esophageal cancer.
The Cancer Genome Atlas databases are used to find two types of esophageal cancer cases. Cox regressions analyses are used to screen genes for hypoxia-related traits. After that, the genetic signature is validated by survival analysis and the construction of ROC curves. GSEA is used to compare differences in enrichment in the two groups and is followed by the CIBERSORT tool to investigate a potentially relevant correlation between immune cells and gene signatures.
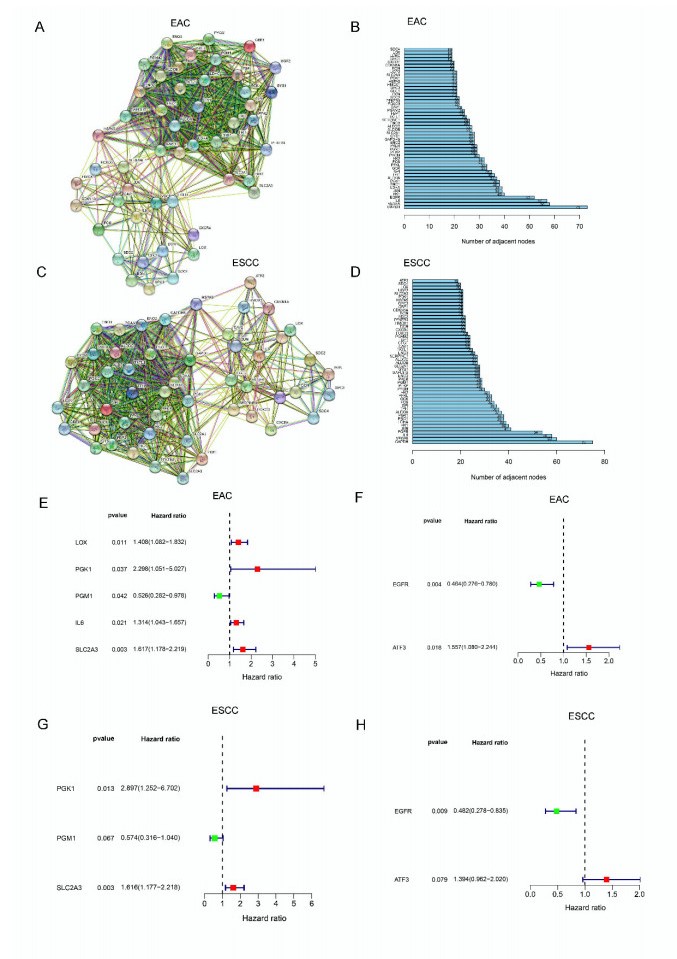
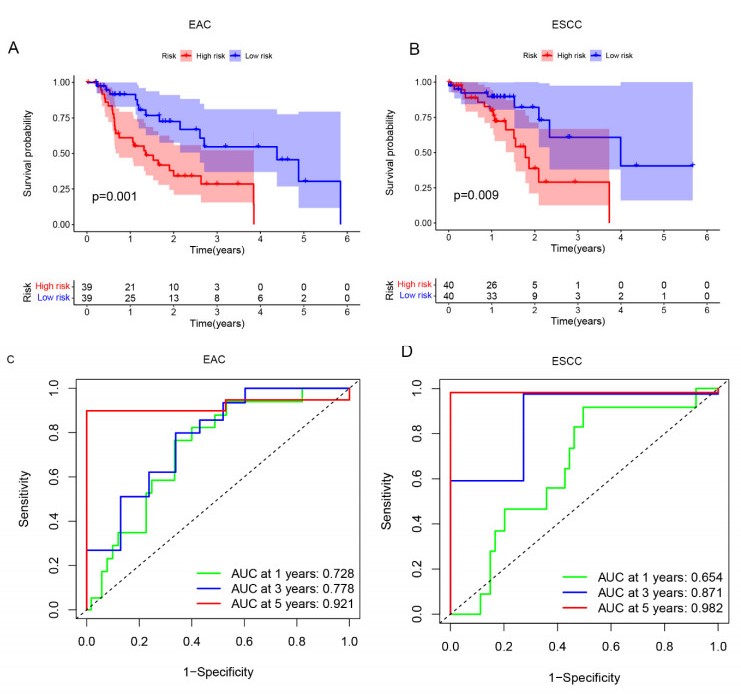
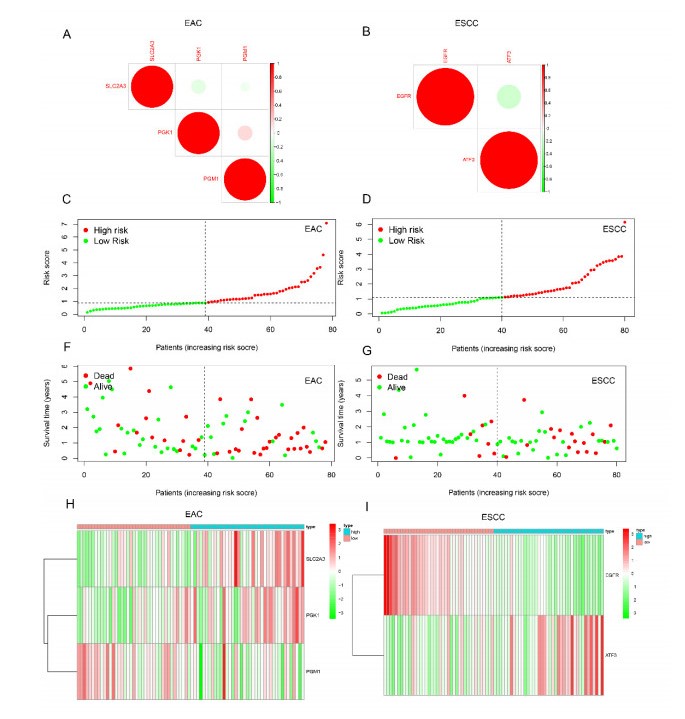
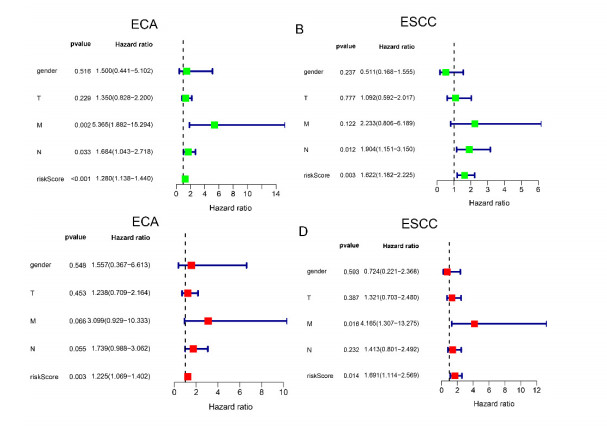
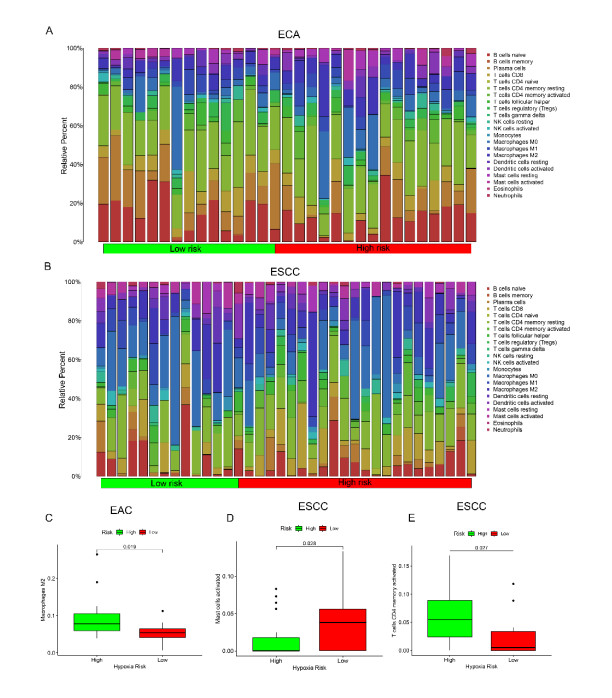
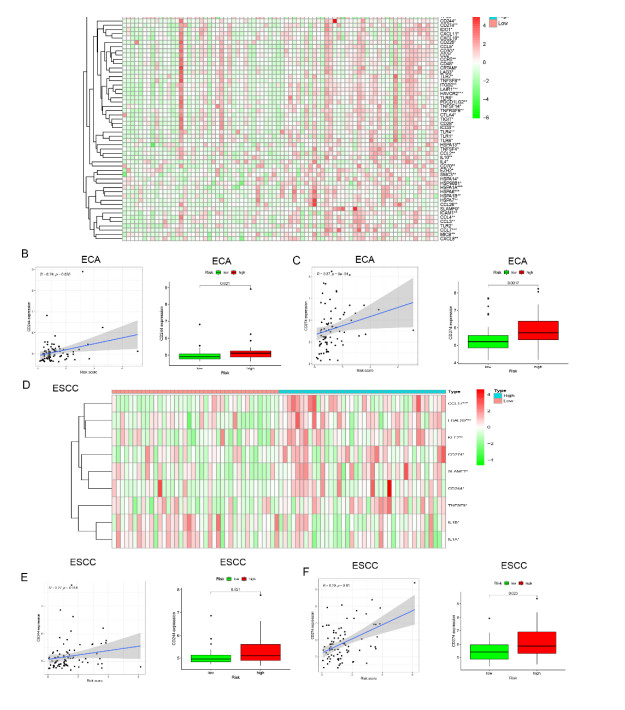
We found that the esophageal adenocarcinoma hypoxia model contains 3 genes (PGK1, PGM1, SLC2A3), and the esophageal squamous cell carcinoma hypoxia model contains 2 genes (EGFR, ATF3). The findings demonstrated that the survival rate of patients in the high-risk group is lower than in the lower-risk group. Furthermore, we find that three kinds of immune cells (memory activated CD4+ T cells, activated mast cells, and M2 macrophages) have a marked infiltration in the tissues of patients in the high-risk group. Moreover, we find that PD-L1 and CD244 are highly expressed in high-risk groups.
Our data demonstrate that oxygen deprivation is correlated with prognosis and the incidence of immune cell infiltration in patients with both types of esophageal cancer, which provides an immunological perspective for the development of personalized therapy.
Citation: Linlin Tan, Dingzhuo Cheng, Jianbo Wen, Kefeng Huang, Qin Zhang. Identification of prognostic hypoxia-related genes signature on the tumor microenvironment in esophageal cancer[J]. Mathematical Biosciences and Engineering, 2021, 18(6): 7743-7758. doi: 10.3934/mbe.2021384
Hypoxia is a crucial factor in the development of esophageal cancer. The relationship between hypoxia and immune status in the esophageal cancer microenvironment is becoming increasingly important in clinical practice. This study aims to clarify and investigate the possible connection between immunotherapy and hypoxia in esophageal cancer.
The Cancer Genome Atlas databases are used to find two types of esophageal cancer cases. Cox regressions analyses are used to screen genes for hypoxia-related traits. After that, the genetic signature is validated by survival analysis and the construction of ROC curves. GSEA is used to compare differences in enrichment in the two groups and is followed by the CIBERSORT tool to investigate a potentially relevant correlation between immune cells and gene signatures.
We found that the esophageal adenocarcinoma hypoxia model contains 3 genes (PGK1, PGM1, SLC2A3), and the esophageal squamous cell carcinoma hypoxia model contains 2 genes (EGFR, ATF3). The findings demonstrated that the survival rate of patients in the high-risk group is lower than in the lower-risk group. Furthermore, we find that three kinds of immune cells (memory activated CD4+ T cells, activated mast cells, and M2 macrophages) have a marked infiltration in the tissues of patients in the high-risk group. Moreover, we find that PD-L1 and CD244 are highly expressed in high-risk groups.
Our data demonstrate that oxygen deprivation is correlated with prognosis and the incidence of immune cell infiltration in patients with both types of esophageal cancer, which provides an immunological perspective for the development of personalized therapy.

| [1] |
J. Ferlay, I. Soerjomataram, R. Dikshit, S. Eser, C. Mathers, M. Rebelo, et al., Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012, Int. J. Cancer, 136 (2015), E359-386. doi: 10.1002/ijc.29210

|
| [2] | M. W. Short, K. G. Burgers, V. T. Fry, Esophageal cancer, Am. Fam. Phys., 95 (2017), 22-28. |
| [3] |
X. Jing, F. Yang, C. Shao, K. Wei, M. Xie, H. Shen, et al., Role of hypoxia in cancer therapy by regulating the tumor microenvironment, Mol. Cancer, 18 (2019), 157. doi: 10.1186/s12943-019-1089-9
|
| [4] |
E. B. Rankin, A. J. Giaccia, Hypoxic control of metastasis, Science (New York, NY), 352 (2016), 175-180. doi: 10.1126/science.aaf4405
|
| [5] |
B. Zhang, B. Tang, J. Gao, J. Li, L. Kong, L. Qin, A hypoxia-related signature for clinically predicting diagnosis, prognosis and immune microenvironment of hepatocellular carcinoma patients, J. Trans. Med., 18 (2020), 342. doi: 10.1186/s12967-020-02492-9
|
| [6] |
V. L. Dengler, M. Galbraith, J. M. Espinosa, Transcriptional regulation by hypoxia inducible factors, Crit. Rev. Biochem. Mol. Biol., 49 (2014), 1-15. doi: 10.3109/10409238.2013.838205
|
| [7] |
X. Lu, Y. Kang, Hypoxia and hypoxia-inducible factors: master regulators of metastasis, Clin. Cancer Res., 16 (2010), 5928-5935. doi: 10.1158/1078-0432.CCR-10-1360
|
| [8] | S. K. Daniel, K. M. Sullivan, K. P. Labadie, V. G. Pillarisetty, Hypoxia as a barrier to immunotherapy in pancreatic adenocarcinoma, Clin. Trans. Med., 8 (2019), 10. |
| [9] |
L. You, W. Wu, X. Wang, L. Fang, V. Adam, E. Nepovimova, et al., The role of hypoxia-inducible factor 1 in tumor immune evasion, Med. Res. Rev., 41 (2021), 1622-1643. doi: 10.1002/med.21771
|
| [10] |
D. Mennerich, K. Kubaichuk, T. Kietzmann, DUBs, hypoxia and cancer, Trends Cancer, 5 (2019), 632-653. doi: 10.1016/j.trecan.2019.08.005
|
| [11] |
V. W. Yuen, C. C. Wong, Hypoxia-inducible factors and innate immunity in liver cancer, J. Clin. Invest., 130 (2020), 5052-5062. doi: 10.1172/JCI137553
|
| [12] |
T. F. Gajewski, H. Schreiber, Y. X. Fu, Innate and adaptive immune cells in the tumor microenvironment, Nat. Immunol., 14 (2013), 1014-1022. doi: 10.1038/ni.2703
|
| [13] |
J. Peerlings, L. V. D. Voorde, C. Mitea, R. Larue, A. Yaromina, S. Sandeleanu, et al., Hypoxia and hypoxia response-associated molecular markers in esophageal cancer: A systematic review, Methods (San Diego, Calif), 130 (2017), 51-62. doi: 10.1016/j.ymeth.2017.07.002
|
| [14] |
A. Palazón, J. Aragonés, A. Morales-Kastresana, M. O. de Landázuri, I. Melero, Molecular pathways: hypoxia response in immune cells fighting or promoting cancer, Clin. Cancer Res., 18 (2012), 1207-1213. doi: 10.1158/1078-0432.CCR-11-1591
|
| [15] |
P. Naeli, M. H. Pourhanifeh, M. R. Karimzadeh, Z. Shabaninejad, A. Movahedpour, H. Tarrahimofrad, et al., Circular RNAs and gastrointestinal cancers: Epigenetic regulators with a prognostic and therapeutic role, Crit. Rev. Oncol. Hematol., 145 (2020), 102854. doi: 10.1016/j.critrevonc.2019.102854
|
| [16] |
M. H. Pourhanifeh, M. Vosough, M. Mahjoubin-Tehran, M. Hashemipour, M. Nejati, M. Abbasi-Kolli, et al., Autophagy-related microRNAs: Possible regulatory roles and therapeutic potential in and gastrointestinal cancers, Pharmacol. Res., 161 (2020), 105133. doi: 10.1016/j.phrs.2020.105133
|
| [17] |
A. Hesari, M. Azizian, A. Sheikhi, A. Nesaei, S. Sanaei, N. Mahinparvar, et al., Chemopreventive and therapeutic potential of curcumin in esophageal cancer: Current and future status, Int. J. Cancer, 144 (2019), 1215-1226. doi: 10.1002/ijc.31947
|
| [18] |
M. Sarvizadeh, O. Hasanpour, Z. N. Ghale-Noie, S. Mollazadeh, M. Rezaei, H. Pourghadamyari, et al., Allicin and digestive system cancers: from chemical structure to its therapeutic opportunities, Front. Oncol., 11 (2021), 650256. doi: 10.3389/fonc.2021.650256
|
| [19] |
F. L. Huang, S. J. Yu, Esophageal cancer: Risk factors, genetic association, and treatment, Asian J. Surg., 41 (2018), 210-215. doi: 10.1016/j.asjsur.2016.10.005
|
| [20] |
F. Chen, L. Chu, J. Li, Y. Shi, B. Xu, J. Gu, et al., Hypoxia induced changes in miRNAs and their target mRNAs in extracellular vesicles of esophageal squamous cancer cells, Thorac. Cancer, 11 (2020), 570-580. doi: 10.1111/1759-7714.13295
|
| [21] | C. M. Silva, V. M. Gonçalves, R. Henrique, C. Jerónimo, I. Bravo, The critical role of hypoxic microenvironment and epigenetic deregulation in esophageal cancer radioresistance, Genes, 10 (2019). |
| [22] | N. Sethi, O. Kikuchi, J. McFarland, Y. Zhang, M. Chung, N. Kafker, et al., Mutant p53 induces a hypoxia transcriptional program in gastric and esophageal adenocarcinoma, JCI Insight, 4 (2019). |
| [23] |
Q. Zhang, J. Zhang, Z. Fu, L. Dong, Y. Tang, C. Xu, et al., Hypoxia-induced microRNA-10b-3p promotes esophageal squamous cell carcinoma growth and metastasis by targeting TSGA10, Aging, 11 (2019), 10374-10384. doi: 10.18632/aging.102462
|
| [24] |
E. P. Cummins, C. T. Taylor, Hypoxia-responsive transcription factors, Pflugers Arch., 450 (2005), 363-371. doi: 10.1007/s00424-005-1413-7
|
| [25] |
Q. Ke, M. Costa, Hypoxia-inducible factor-1 (HIF-1), Mol. Pharmacol., 70 (2006), 1469-1480. doi: 10.1124/mol.106.027029
|
| [26] |
A. Loboda, A. Jozkowicz, J. Dulak, HIF-1 and HIF-2 transcription factors-similar but not identical, Mol. Cells, 29 (2010), 435-442. doi: 10.1007/s10059-010-0067-2
|
| [27] | G. L. Semenza, Hypoxia-inducible factor 1 (HIF-1) pathway, Sci. STKE, 2007 (2007), 8. |
| [28] |
D. Zhou, C. Huang, Z. Lin, S. Zhan, L. Kong, C. Fang, et al., Macrophage polarization and function with emphasis on the evolving roles of coordinated regulation of cellular signaling pathways, Cell Signal, 26 (2014), 192-197. doi: 10.1016/j.cellsig.2013.11.004
|
| [29] |
A. Mantovani, S. Sozzani, M. Locati, P. Allavena, A. Sica, Macrophage polarization: tumor-associated macrophages as a paradigm for polarized M2 mononuclear phagocytes, Trends Immunol., 23 (2002), 549-555. doi: 10.1016/S1471-4906(02)02302-5
|
| [30] | N. B. Hao, M. H. Lü, Y. H. Fan, Y. L. Cao, Z. R. Zhang, S. M. Yang, Macrophages in tumor microenvironments and the progression of tumors, Clin. Dev. Immunol., 2012 (2012), 948098. |
| [31] |
J. W. Pollard, Tumour-educated macrophages promote tumour progression and metastasis, Nat. Rev. Cancer, 4 (2004), 71-78. doi: 10.1038/nrc1256
|
| [32] |
C. Yunna, H. Mengru, W. Lei, C. Weidong, Macrophage M1/M2 polarization, Eur. J. Pharmacol., 877 (2020), 173090. doi: 10.1016/j.ejphar.2020.173090
|
| [33] | L. Agresta, M. Lehn, K. Lampe, R. Cantrell, C. Hennies, S. Szabo, et al., CD244 represents a new therapeutic target in head and neck squamous cell carcinoma, J. Immunother. Cancer, 8 (2020). |
| [34] |
M. G. Mofrad, D. T. Maleki, E. Faghihloo, The roles of programmed death ligand 1 in virus-associated cancers, Infect. Genet Evol., 84 (2020), 104368. doi: 10.1016/j.meegid.2020.104368
|
| [35] |
X. Zhu, J. Lang, Soluble PD-1 and PD-L1: predictive and prognostic significance in cancer, Oncotarget, 8 (2017), 97671-97682. doi: 10.18632/oncotarget.18311
|
| [36] |
C.Y. Mu, J. A. Huang, Y. Chen, C. Chen, X.G. Zhang, High expression of PD-L1 in lung cancer may contribute to poor prognosis and tumor cells immune escape through suppressing tumor infiltrating dendritic cells maturation, Med. Oncol., 28 (2011), 682-688. doi: 10.1007/s12032-010-9515-2
|
| [37] |
K. Azuma, K. Ota, A. Kawahara, S. Hattori, E. Iwama, T. Harada, et al., Association of PD-L1 overexpression with activating EGFR mutations in surgically resected nonsmall-cell lung cancer, Ann. Oncol., 25 (2014), 1935-1940. doi: 10.1093/annonc/mdu242
|
| [38] |
J. Hou, Z. Yu, R. Xiang, C. Li, L. Wang, S. Chen, et al., Correlation between infiltration of FOXP3+ regulatory T cells and expression of B7-H1 in the tumor tissues of gastric cancer, Exp. Mol. Pathol., 96 (2014), 284-291. doi: 10.1016/j.yexmp.2014.03.005
|
| [39] |
R. A. Droeser, C. Hirt, C. T. Viehl, D. M. Frey, C. Nebiker, X. Huber, et al., Clinical impact of programmed cell death ligand 1 expression in colorectal cancer, Eur. J. Cancer, 49 (2013), 2233-2242. doi: 10.1016/j.ejca.2013.02.015
|
| [40] |
Y. Ohigashi, M. Sho, Y. Yamada, Y. Tsurui, K. Hamada, N. Ikeda, et al., Clinical significance of programmed death-1 ligand-1 and programmed death-1 ligand-2 expression in human esophageal cancer, Clin. Cancer Res., 11 (2005), 2947-2953. doi: 10.1158/1078-0432.CCR-04-1469
|
| [41] | L. Chen, H. Deng, M. Lu, B. Xu, Q. Wang, J. Jiang, et al., B7-H1 expression associates with tumor invasion and predicts patient's survival in human esophageal cancer, Int. J. Clin. Exp. Pathol., 7 (2014), 6015-6023. |
| [42] |
H. Dong, S. E. Strome, D. R. Salomao, H. Tamura, F. Hirano, D. B. Flies, et al., Tumor-associated B7-H1 promotes T-cell apoptosis: a potential mechanism of immune evasion, Nat. Med., 8 (2002), 793-800. doi: 10.1038/nm730
|
| [43] |
P. Dong, Y. Xiong, J. Yue, S. J. B. Hanley, H. Watari, Tumor-intrinsic PD-L1 signaling in cancer initiation, development and treatment: beyond immune evasion, Front. Oncol., 8 (2018), 386. doi: 10.3389/fonc.2018.00386
|
| [44] |
J. Cai, D. Wang, G. Zhang, X. Guo, The role of PD-1/PD-L1 axis in treg development and function: implications for cancer immunotherapy, Oncol. Targets Ther., 12 (2019), 8437-8445. doi: 10.2147/OTT.S221340
|
| [45] |
T. V. Larsen, D. Hussmann, A. L. Nielsen, PD-L1 and PD-L2 expression correlated genes in non-small-cell lung cancer, Cancer Commun. (Lond), 39 (2019), 30. doi: 10.1186/s40880-019-0376-6
|
| [46] |
R. Erber, A. Hartmann, Understanding PD-L1 testing in breast cancer: A practical approach, Breast Care (Basel), 15 (2020), 481-490. doi: 10.1159/000510812
|
| [47] |
F. Wei, T. Zhang, S. C. Deng, J. C. Wei, P. Yang, Q. Wang, et al., PD-L1 promotes colorectal cancer stem cell expansion by activating HMGA1-dependent signaling pathways, Cancer Lett., 450 (2019), 1-13. doi: 10.1016/j.canlet.2019.02.022
|
| [48] |
K. Junker, M. Eckstein, M. Fiorentino, R. Montironi, PD1/PD-L1 Axis in Uro-oncology, Curr. Drug Targets, 21 (2020), 1293-1300. doi: 10.2174/1389450121666200326123700
|
| [49] |
R. J. Kelly, Immunotherapy for esophageal and gastric cancer, Am. Soc. Clin. Oncol. Educ. Book, 37 (2017), 292-300. doi: 10.1200/EDBK_175231
|
| [50] |
X. Wang, F. Teng, L. Kong, J. Yu, PD-L1 expression in human cancers and its association with clinical outcomes, Oncol. Targets Ther., 9 (2016), 5023-5039. doi: 10.2147/OTT.S105862
|
 mbe-18-06-384-Supplemental Tables 1-4.pdf mbe-18-06-384-Supplemental Tables 1-4.pdf |
 |
Figures(6)

Linlin Tan, Dingzhuo Cheng, Jianbo Wen, Kefeng Huang, Qin Zhang. Identification of prognostic hypoxia-related genes signature on the tumor microenvironment in esophageal cancer[J]. Mathematical Biosciences and Engineering, 2021, 18(6): 7743-7758. doi: 10.3934/mbe.2021384







 DownLoad:
DownLoad: