Eosinophilic esophagitis (EoE) is a chronic allergen/immune-mediated disease known by eosinophil infiltration into the esophagus. Topical steroids are used for its treatment. We investigated the efficacy, side effects, and symptom relapse after discontinuation of two budesonide forms in EoE patients.
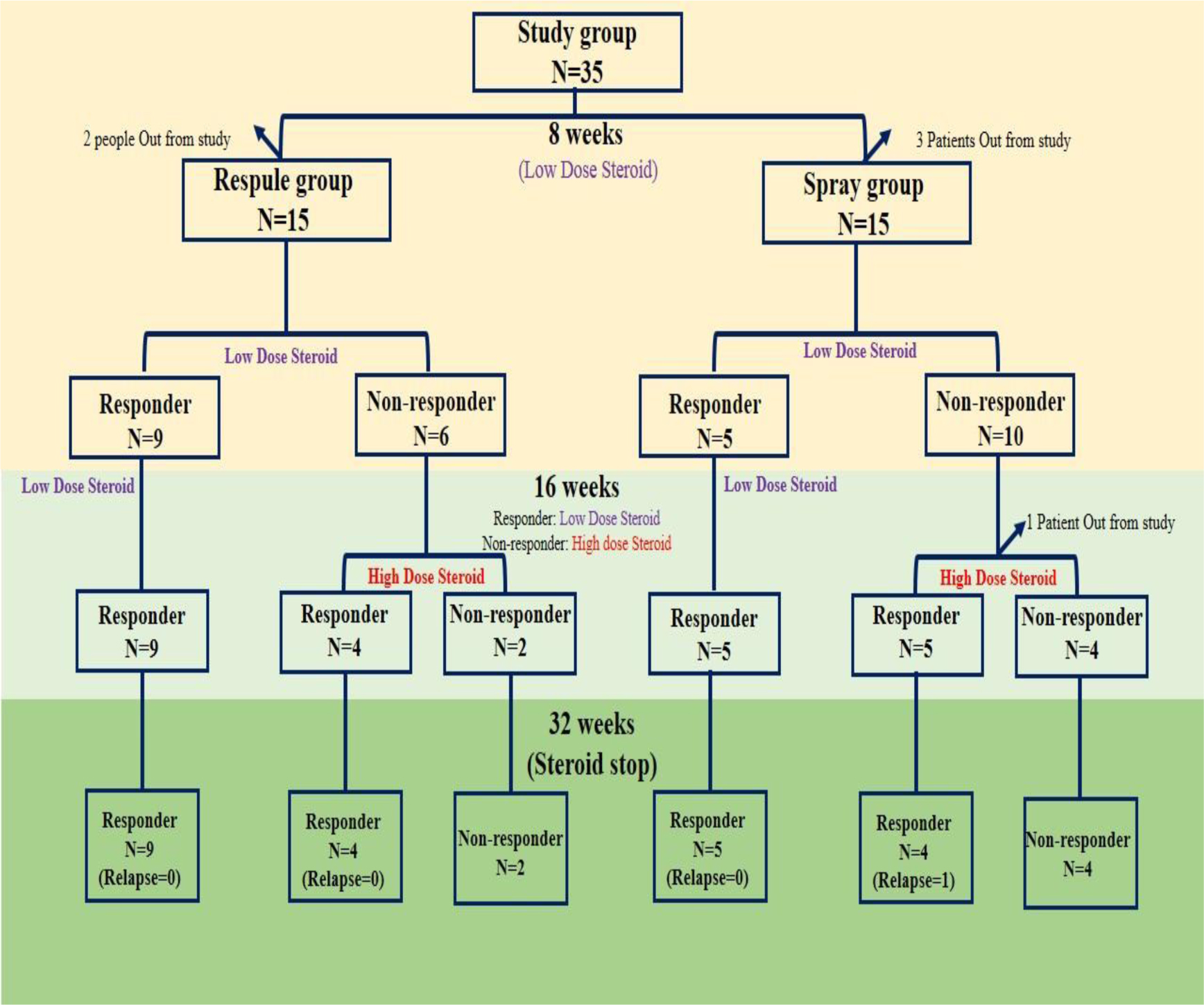
In this prospective, dose-ranging, randomized trial, 35 EoE patients under 18 years who received two budesonide forms were assigned to low-dose oral respule (17 patients) and swallowed metered-dose inhaler (MDI) (18 patients) groups. Both groups received low-dose budesonide for eight weeks. Doses were doubled after the first eight weeks if symptom remission was not achieved, but the previous dose was continued for the next eight weeks for the subjects with symptom relief. At the end of week 16, budesonide was discontinued in all patients. The following outcomes were assessed: The primary outcome was symptom relief, assessed by Pediatric EoE Symptom Scores (PEESS®v2.0). Secondary outcomes included safety, side effects, and histological changes, based on repeated endoscopy at weeks 0, 8, 16, and 32.
Non-response to low-dose treatment in the first eight weeks was observed in 2 cases (13.3%, 95% CI: 2.6%–35.2%) in the respule group and 7 cases (50.0%, 95% CI: 22.7%–77.3%) in the MDI group, indicating a significant difference between the groups (p = 0.033). In the 16th week, the treatment failure rate was 13.3% and 26.6% in the oral respule and swallowed MDI groups, respectively (p = 0.048). The therapeutic response during the 8th week was significantly higher in oral respule group than swallowed MDI group (OR = 8.418, p = 0.046).
This study indicates that the oral respule formulation of budesonide is more effective than the swallowed MDI in alleviating symptoms of eosinophilic esophagitis (EoE) in children. The oral respule not only resulted in a higher rate of symptom relief but also exhibited a better safety profile, with fewer incidents of oral thrush and adrenal suppression.
Citation: Farhad Seif, Nastaran Amiri, Majid Khoshmirsafa, Saba Arshi, Mohammad Nabavi, Mohammad Hassan Bemanian, Sima Shokri, Azizollah Yousefi, Banafshe Rajabian, Fatemeh Mahjoob, Nikoo Emtiazi, Morteza Fallahpour. Respule or metered-dose inhaler for eosinophilic esophagitis treatment? A dose-ranging, randomized clinical trial study on efficacy, safety, and relapse rate[J]. AIMS Allergy and Immunology, 2024, 8(3): 193-203. doi: 10.3934/Allergy.2024010
Eosinophilic esophagitis (EoE) is a chronic allergen/immune-mediated disease known by eosinophil infiltration into the esophagus. Topical steroids are used for its treatment. We investigated the efficacy, side effects, and symptom relapse after discontinuation of two budesonide forms in EoE patients.
In this prospective, dose-ranging, randomized trial, 35 EoE patients under 18 years who received two budesonide forms were assigned to low-dose oral respule (17 patients) and swallowed metered-dose inhaler (MDI) (18 patients) groups. Both groups received low-dose budesonide for eight weeks. Doses were doubled after the first eight weeks if symptom remission was not achieved, but the previous dose was continued for the next eight weeks for the subjects with symptom relief. At the end of week 16, budesonide was discontinued in all patients. The following outcomes were assessed: The primary outcome was symptom relief, assessed by Pediatric EoE Symptom Scores (PEESS®v2.0). Secondary outcomes included safety, side effects, and histological changes, based on repeated endoscopy at weeks 0, 8, 16, and 32.
Non-response to low-dose treatment in the first eight weeks was observed in 2 cases (13.3%, 95% CI: 2.6%–35.2%) in the respule group and 7 cases (50.0%, 95% CI: 22.7%–77.3%) in the MDI group, indicating a significant difference between the groups (p = 0.033). In the 16th week, the treatment failure rate was 13.3% and 26.6% in the oral respule and swallowed MDI groups, respectively (p = 0.048). The therapeutic response during the 8th week was significantly higher in oral respule group than swallowed MDI group (OR = 8.418, p = 0.046).
This study indicates that the oral respule formulation of budesonide is more effective than the swallowed MDI in alleviating symptoms of eosinophilic esophagitis (EoE) in children. The oral respule not only resulted in a higher rate of symptom relief but also exhibited a better safety profile, with fewer incidents of oral thrush and adrenal suppression.

| [1] |
Prasad GA, Alexander JA, Schleck CD, et al. (2009) Epidemiology of eosinophilic esophagitis over three decades in Olmsted County, Minnesota. Clini Gastroenterol Hepatol 7: 1055-1061. https://doi.org/10.1016/j.cgh.2009.06.023 
|
| [2] |
Robson J, O'Gorman M, McClain A, et al. (2019) Incidence and prevalence of pediatric eosinophilic esophagitis in Utah based on a 5-year population-based study. Clini Gastroenterol Hepatol 17: 107-114.e1. https://doi.org/10.1016/j.cgh.2018.06.028
|
| [3] |
Furuta GT, Liacouras CA, Collins MH, et al. (2007) Eosinophilic esophagitis in children and adults: A systematic review and consensus recommendations for diagnosis and treatment: Sponsored by the American Gastroenterological Association (AGA) Institute and North American Society of Pediatric Gastroenterology, Hepatology, and Nutrition. Gastroenterology 133: 1342-1363. https://doi.org/10.1053/j.gastro.2007.08.017
|
| [4] |
Chehade M, Kamboj AP, Atkins D, et al. (2021) Diagnostic delay in patients with eosinophilic gastritis and/or duodenitis: A population-based study. J Allergy Clini Immunol: In Practice 9: 2050-2059.e20. https://doi.org/10.1016/j.jaip.2020.12.054
|
| [5] |
Liacouras CA, Furuta GT, Hirano I, et al. (2011) Eosinophilic esophagitis: Updated consensus recommendations for children and adults. J Allergy Clin Immunol 128: 3-20.e6.
|
| [6] |
Moawad FJ (2018) Eosinophilic esophagitis: Incidence and prevalence. Gastrointest Endosc Clin 28: 15-25. https://doi.org/10.1016/j.giec.2017.07.001
|
| [7] |
Hirano I, Moy N, Heckman MG, et al. (2013) Endoscopic assessment of the oesophageal features of eosinophilic oesophagitis: Validation of a novel classification and grading system. Gut 62: 489-495. https://doi.org/10.1136/gutjnl-2011-301817
|
| [8] |
Chehade M, Sampson HA, Morotti RA, et al. (2007) Esophageal subepithelial fibrosis in children with eosinophilic esophagitis. J Pediatr Gastroenterol Nutr 45: 319-328. https://doi.org/10.1097/MPG.0b013e31806ab384
|
| [9] |
Dellon ES, Kim HP, Sperry SL, et al. (2014) A phenotypic analysis shows that eosinophilic esophagitis is a progressive fibrostenotic disease. Gastrointest Endosc 79: 577-585.e4. https://doi.org/10.1016/j.gie.2013.10.027
|
| [10] |
Liacouras CA, Spergel J, Gober LM (2014) Eosinophilic esophagitis: clinical presentation in children. Gastroenterol Clin 43: 219-229. https://doi.org/10.1016/j.gtc.2014.02.012
|
| [11] |
Nennstiel S, Schlag C (2020) Treatment of eosinophlic esophagitis with swallowed topical corticosteroids. World J Gastroenterol 26: 5395. https://doi.org/10.3748/wjg.v26.i36.5395
|
| [12] |
Noel RJ, Rothenberg ME (2005) Eosinophilic esophagitis. Curr Opin Pediatr 17: 690-694. https://doi.org/10.1097/01.mop.0000184291.34654.be
|
| [13] |
Sperge JM, Andrews IT, Brown-Whitehorn TF, et al. (2005) Treatment of eosinophilic esophagitis with specific food elimination diet directed by a combination of skin prick and patch tests. Ann Allergy Asthma Immunol 95: 336-343. https://doi.org/10.1016/S1081-1206(10)61151-9
|
| [14] |
Liacouras CA, Spergel JM, Ruchelli E, et al. (2005) Eosinophilic esophagitis: A 10-year experience in 381 children. Clini Gastroenterol Hepatol 3: 1198-1206. https://doi.org/10.1016/S1542-3565(05)00885-2
|
| [15] |
Albert D, Heifert TA, Min SB, et al. (2016) Comparisons of fluticasone to budesonide in the treatment of eosinophilic esophagitis. Dig Dis Sci 61: 1996-2001. https://doi.org/10.1007/s10620-016-4110-9
|
| [16] |
Gómez-Aldana A, Jaramillo-Santos M, Delgado A, et al. (2019) Eosinophilic esophagitis: Current concepts in diagnosis and treatment. World J Gastroenterol 25: 4598. https://doi.org/10.3748/wjg.v25.i32.4598
|
| [17] |
Mendes ES, Rebolledo P, Campos M, et al. (2014) Immediate antiinflammatory effects of inhaled budesonide in patients with asthma. Ann Am Thorac Soc 11: 706-711. https://doi.org/10.1513/AnnalsATS.201307-220OC
|
| [18] |
Dellon ES, Liacouras CA, Molina-Infante J, et al. (2018) Updated international consensus diagnostic criteria for eosinophilic esophagitis: Proceedings of the AGREE conference. Gastroenterology 155: 1022-1033.e10. https://doi.org/10.1053/j.gastro.2018.07.009
|
| [19] | Aceves SS (2016) Allergy testing in patients with eosinophilic esophagitis. Gastroenterol Hepatol 12: 516-518. |
| [20] | Anyane-Yeboa A, Wang W, Kavitt RT (2018) The role of allergy testing in eosinophilic esophagitis. Gastroenterol Hepatol 14: 463. |
| [21] |
Pitsios C, Vassilopoulou E, Pantavou K, et al. (2022) Allergy-test-based elimination diets for the treatment of eosinophilic esophagitis: A systematic review of their efficacy. J Clin Med 11: 5631. https://doi.org/10.3390/jcm11195631
|
| [22] |
Yousefi A, Nasehi S, Arshi S, et al. (2021) Assessment of IgE-and cell-mediated immunity in pediatric patients with eosinophilic esophagitis. Eur ann allergy clin 53: 86-90. https://doi.org/10.23822/EurAnnACI.1764-1489.154
|
| [23] |
Schoepfer AM, Straumann A, Safroneeva E (2018) Pharmacologic treatment of eosinophilic esophagitis: An update. Gastrointest Endosc Clin North Am 28: 77-88. https://doi.org/10.1016/j.giec.2017.07.007
|
| [24] | Zur E (2012) Eosinophilic esophagitis: Treatment with oral viscous budesonide. Int J Pharm Comp 16: 288-293. |
| [25] |
Gupta SK, Vitanza JM, Collins MH (2015) Efficacy and safety of oral budesonide suspension in pediatric patients with eosinophilic esophagitis. Clin Gastroenterol Hepatol 13: 66-76.e3. https://doi.org/10.1016/j.cgh.2014.05.021
|
| [26] |
Vaghi A, Berg E, Liljedahl S, et al. (2005) In vitro comparison of nebulised budesonide (Pulmicort Respules®) and beclomethasone dipropionate (Clenil® per Aerosol). Pulm Pharmacol Ther 18: 151-153. https://doi.org/10.1016/j.pupt.2004.10.004
|
| [27] |
Neubauer PD, Schwam ZG, Manes RP (2016) Comparison of intranasal fluticasone spray, budesonide atomizer, and budesonide respules in patients with chronic rhinosinusitis with polyposis after endoscopic sinus surgery. Int Forum Allergy Rhinol 2016: 233-237. https://doi.org/10.1002/alr.21688
|
| [28] |
Fable JM, Fernandez M, Goodine S, et al. (2018) Retrospective comparison of fluticasone propionate and oral viscous budesonide in children with eosinophilic esophagitis. J Pediatr Gastroenterol Nutr 66: 26-32. https://doi.org/10.1097/MPG.0000000000001626
|
| [29] |
Dellon ES, Woosley JT, Arrington A, et al. (2019) Efficacy of budesonide vs fluticasone for initial treatment of eosinophilic esophagitis in a randomized controlled trial. Gastroenterology 157: 65-73.e5. https://doi.org/10.1053/j.gastro.2019.03.014
|
| [30] |
D'Alessandro A, Esposito D, Pesce M, et al. (2015) Eosinophilic esophagitis: From pathophysiology to treatment. World J Gastrointest Pathophysiol 6: 150. https://doi.org/10.4291/wjgp.v6.i4.150
|
Figures(1) / Tables(3)

Farhad Seif, Nastaran Amiri, Majid Khoshmirsafa, Saba Arshi, Mohammad Nabavi, Mohammad Hassan Bemanian, Sima Shokri, Azizollah Yousefi, Banafshe Rajabian, Fatemeh Mahjoob, Nikoo Emtiazi, Morteza Fallahpour. Respule or metered-dose inhaler for eosinophilic esophagitis treatment? A dose-ranging, randomized clinical trial study on efficacy, safety, and relapse rate[J]. AIMS Allergy and Immunology, 2024, 8(3): 193-203. doi: 10.3934/Allergy.2024010







 DownLoad:
DownLoad: