With the recent approval of booster vaccinations in the United States for adults who already received their primary vaccinations, millions of adults have been administered the Pfizer-BioNTech or Moderna booster vaccines. Adverse events related to these vaccines continue to be reported and are majority self-limited. In this case report, we present a young male who acquired chronic, migratory dermatographic urticaria two weeks after administration of the Moderna mRNA-1273 COVID-19 vaccine booster.
Citation: Richard A. Maiella, Kelly M. Staples, Ashokvardhan Veldanda. Migratory dermatographic urticaria following COVID-19 vaccine booster in young adult male[J]. AIMS Allergy and Immunology, 2022, 6(1): 14-18. doi: 10.3934/Allergy.2022003
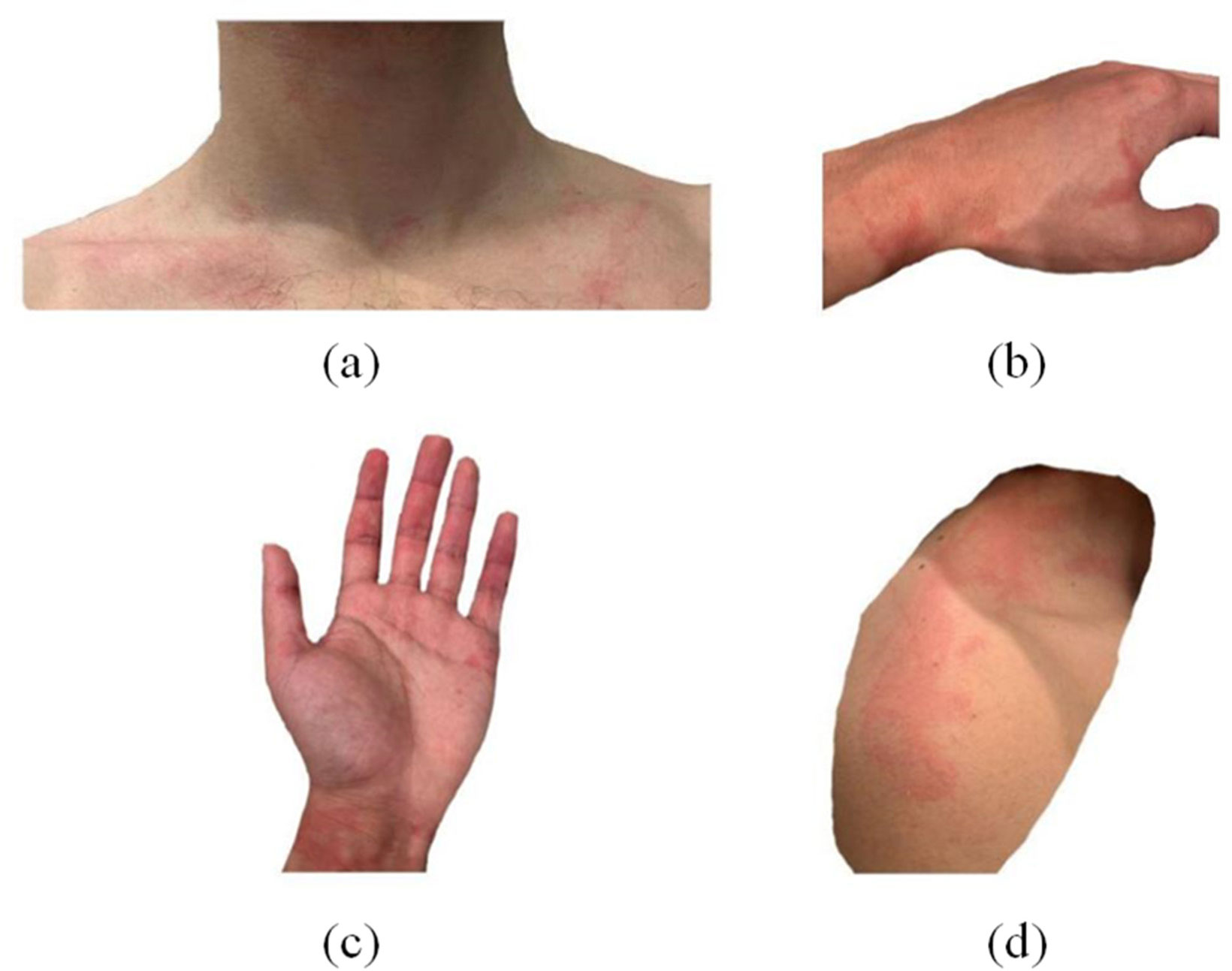
With the recent approval of booster vaccinations in the United States for adults who already received their primary vaccinations, millions of adults have been administered the Pfizer-BioNTech or Moderna booster vaccines. Adverse events related to these vaccines continue to be reported and are majority self-limited. In this case report, we present a young male who acquired chronic, migratory dermatographic urticaria two weeks after administration of the Moderna mRNA-1273 COVID-19 vaccine booster.

| [1] | (2021) U.S. Food and Drug Administration, Coronavirus (COVID-19) Update: FDA Expands Eligibility for COVID-19 Vaccine Boosters. FDA. Available from: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-expands-eligibility-covid-19-vaccine-boosters |
| [2] |
Mathieu E, Ritchie H, Ortiz-Ospina E, et al. (2021) A global database of COVID-19 vaccinations. Nat Hum Behav 5: 947-953. https://doi.org/10.1038/s41562-021-01122-8 
|
| [3] |
Baden LR, El Sahly HM, Essink B, et al. (2021) Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine. New Engl J Med 384: 403-416. https://doi.org/10.1056/NEJMoa2035389
|
| [4] |
McMahon DE, Amerson E, Rosenbach M, et al. (2021) Cutaneous reactions reported after Moderna and Pfizer COVID-19 vaccination: a registry-based study of 414 cases. J Am Acad Dermatol 85: 46-55. https://doi.org/10.1016/j.jaad.2021.03.092
|
| [5] |
Gronbeck C, Grant-Kels JM (2021) Attention all anti-vaccinators: The cutaneous adverse events from the mRNA COVID-19 vaccines are not an excuse to avoid them!. Clin Dermatol 39: 674-687. https://doi.org/10.1016/j.clindermatol.2021.05.027
|
| [6] | Thomas J, Thomas G, Chatim A, et al. (2021) Chronic spontaneous urticaria after COVID-19 vaccine. Cureus 13: e18102. https://doi.org/10.7759/cureus.18102 |
| [7] |
Johnston MS, Galan A, Watsky KL, et al. (2021) Delayed localized hypersensitivity reactions to the Moderna COVID-19 vaccine: a case series. JAMA Dermatol 157: 716-720. https://doi.org/10.1001/jamadermatol.2021.1214
|
Figures(1)

Richard A. Maiella, Kelly M. Staples, Ashokvardhan Veldanda. Migratory dermatographic urticaria following COVID-19 vaccine booster in young adult male[J]. AIMS Allergy and Immunology, 2022, 6(1): 14-18. doi: 10.3934/Allergy.2022003







 DownLoad:
DownLoad: