Citation: Helena Walz, Barbara Bohn, Jessica Sander, Claudia Eberle, Monika Alisch, Bernhard Oswald, Anja Kroke. Access to Difficult-to-reach Population Subgroups: A Family Midwife Based Home Visiting Service for Implementing Nutrition-related Preventive Activities - A Mixed Methods Explorative Study[J]. AIMS Public Health, 2015, 2(3): 516-536. doi: 10.3934/publichealth.2015.3.516

| [1] | Dalstra J (2005) Socioeconomic differences in the prevalence of common chronic diseases: an overview of eight European countries. Int J Epidemiol 34(2):316-326. |
| [2] | Berkman LF (2009) Social Epidemiology: Social Determinants of Health in the United States: Are We Losing Ground? Annu Rev Publ Health 30(1):27-41. |
| [3] | Braveman PA, Cubbin C, Egerter S, et al. (2010) Socioeconomic Disparities in Health in the United States: What the Patterns Tell Us. Am J Publ Health 100(S1):S186. |
| [4] | Friel S, Marmot MG (2011) Action on the Social Determinants of Health and Health Inequities Goes Global. Annu Rev Publ Health 32(1):225-36. |
| [5] | Bleich SN, Jarlenski MP, Bell CN, et al. (2012) Health Inequalities: Trends, Progress, and Policy. Annu Rev Publ Health 33(1):7-40. |
| [6] | Lampert T, Kroll L, Lippe E, et al. (2013) Sozioökonomischer Status und Gesundheit: Ergebnisse der Studie zur Gesundheit Erwachsener in Deutschland (DEGS1). Bundesgesundheitsblatt-Gesundheitsforschung-Gesundheitsschutz 56(5-6):814-821. |
| [7] | Kröger H, Pakpahan E, Hoffmann R (2015) What causes health inequality? A systematic review on the relative importance of social causation and health selection. Europ J Publ Health. (in press) |
| [8] | Fernández-Alvira JM, Börnhorst C, Bammann K, et al. (2015) Prospective associations between socio-economic status and dietary patterns in European children: the Identification and Prevention of Dietary- and Lifestyle-induced Health Effects in Children and Infants (IDEFICS) Study. Brit J Nutr 113(3):517-525. |
| [9] | Giskes K, Kunst AE, Benach J, et al. (2005) Trends in smoking behaviour between 1985 and 2000 in nine European countries by education. J Epidemiol Commun Health 59(5):395-401. |
| [10] | Haustein K (2006) Smoking and poverty. European journal of cardiovascular prevention and rehabilitation official journal of the European Society of Cardiology, Working Groups on Epidemiology & Prevention and Cardiac Rehabilitation and Exercise Physiology 13(3):312-318. |
| [11] | Giovino GA, Mirza SA, Samet JM, et al. (2012) Tobacco use in 3 billion individuals from 16 countries: an analysis of nationally representative cross-sectional household surveys. Lancet 380(9842):668-679. |
| [12] | Lampert T, Lippe E, Müters S (2013) Verbreitung des Rauchens in der Erwachsenenbevölkerung in Deutschland. Bundesgesundheitsblatt-Gesundheitsforschung-Gesundheitsschutz 56(5-6):802-808. |
| [13] | Varo JJ, Martínez-González MA, Irala-Estévez J de, et al. (2003) Distribution and determinants of sedentary lifestyles in the European Union. Int J Epidemiol 32(1):138-146. |
| [14] | Gidlow C, Johnston LH, Crone D, et al. (2006) A systematic review of the relationship between socio-economic position and physical activity. Health Educ J 65(4):338-367. |
| [15] | Krug S, Jordan S, Mensink G, et al. (2013) Körperliche Aktivität. Bundesgesundheitsblatt-Gesundheitsforschung-Gesundheitsschutz 56(5-6):765-771. |
| [16] | Irala-Estévez JD, Groth M, Johansson L, et al. (2000) A systematic review of socio-economic differences in food habits in Europe: consumption of fruit and vegetables. Europ J Clin Nutr 54(9):706-714. |
| [17] | Hulshof KFAM, Brussaard JH, Kruizinga AG, et al. (2003) Socio-economic status, dietary intake and 10 y trends: the Dutch National Food Consumption Survey. Europ J Clin Nutr 57(1):128-137. |
| [18] | Shahar D, Shai I, Vardi H, et al. (2005) Diet and eating habits in high and low socioeconomic groups. Nutr 21(5):559-566. |
| [19] | Mackenbach JP, Cavelaars AE, Kunst AE, et al. (2000) Socioeconomic inequalities in cardiovascular disease mortality; an international study. Europ Heart J 21(14):1141-1151. |
| [20] | Gößwald A, Lange M, Kamtsiuris P, et al. (2012) DEGS: Studie zur Gesundheit Erwachsener in Deutschland. Bundesgesundheitsblatt-Gesundheitsforschung-Gesundheitsschutz 55(6-7):775-780. |
| [21] | Agardh E, Allebeck P, Hallqvist J, et al. (2011) Type 2 diabetes incidence and socio-economic position: a systematic review and meta-analysis. Int J Epidemiol 40(3):804-818. |
| [22] | World Cancer Research Fund (2007) Food, nutrition, physical activity, and the prevention of cancer: A global perspective. WCRF/AICR, Washington, DC. |
| [23] | Mackenbach JP, Stirbu I, Roskam AR, et al. (2008) Socioeconomic Inequalities in Health in 22 European Countries. New Engl J Med 358(23):2468-2481. |
| [24] | Lampert T, Kurth B (2007) Sozialer Status und Gesundheit von Kindern und Jugendlichen: Ergebnisse der Kinder- und Jugendgesundheitssurveys (KiGGS). Deutsches Ärzteblatt 104(43):A2944 - A 2949. |
| [25] | Currie C, Zanotti C, Morgan A, et al. (2012) Social determinants of health and well-being among young people. Health Behaviour in School-aged Children (HBSC) study: international report from the 2009/2010 survey. (Health Policy for Children and Adolescents, No. 6), Copenhagen. |
| [26] | Hölling H, Schlack R, Petermann F, et al. (2014) Psychische Auffälligkeiten und psychosoziale Beeinträchtigungen bei Kindern und Jugendlichen im Alter von 3 bis 17 Jahren in Deutschland - Prävalenz und zeitliche Trends zu 2 Erhebungszeitpunkten (2003-2006 und 2009-2012): Ergebnisse der KiGGS-Studie - Erste Folgebefragung (KiGGS Welle 1). Bundesgesundheitsblatt-Gesundheitsforschung-Gesundheitsschutz 57(7):807-819. |
| [27] | Birnie K, Cooper R, Martin RM, et al. (2011) Childhood Socioeconomic Position and Objectively Measured Physical Capability Levels in Adulthood: A Systematic Review and Meta-Analysis. PLoS ONE 6(1):e15564. |
| [28] | Ellert U, Brettschneider A, Ravens-Sieberer U (2014) Gesundheitsbezogene Lebensqualität bei Kindern und Jugendlichen in Deutschland: Ergebnisse der KiGGS-Studie - Erste Folgebefragung (KiGGS Welle 1). Bundesgesundheitsblatt-Gesundheitsforschung-Gesundheitsschutz 57(7):798-806. |
| [29] | Richter M, Hurrelmann K (eds) (2009) Gesundheitliche Ungleichheit: Grundlagen, Probleme, Perspektiven, 2nd edn. Verlag für Sozialwissenschaften, Wiesbaden. |
| [30] | Laaksonen M, Roos E, Rahkonen O, et al. (2005) Influence of material and behavioural factors on occupational class differences in health. J Epidemiol Commun Health 59(2):163-169. |
| [31] | van Oort FVA, van Lenthe FJ, Mackenbach JP (2005) Material, psychosocial, and behavioural factors in the explanation of educational inequalities in mortality in The Netherlands. J Epidemiol Commun Health 59(3):214-220. |
| [32] | Plagemann A (ed) (2011) Perinatal programming: The state of the art. De Gruyter, Berlin, Boston. |
| [33] | Bateson P, Barker DJP, Clutton-Brock T, et al. (2004) Developmental plasticity and human health. Nature 430(6998):419-421. |
| [34] | Blumfield ML, Hure AJ, Macdonald-Wicks L, et al. (2012) Systematic review and meta-analysis of energy and macronutrient intakes during pregnancy in developed countries. Nutr Rev70(6):322-336. |
| [35] | Blumfield ML, Hure AJ, Macdonald-Wicks L, et al. (2013) A systematic review and meta-analysis of micronutrient intakes during pregnancy in developed countries. Nutr Rev71(2):118-132. |
| [36] | Barker DJP (1995) Fetal origins of coronary heart disease. British Med J Clin res 311(6998):171-174. |
| [37] | Harder T, Rodekamp E, Schellong K, et al. (2007) Birth Weight and Subsequent Risk of Type 2 Diabetes: A Meta-Analysis. Am J Epidemiol 165(8):849-857. |
| [38] | Yajnik C, Deshmukh U (2011) Early life origins of diabetes and obesity: General aspects and the thin - a fat baby paradigm, In: Plagemann A (ed) Perinatal programming: The state of the art: De Gruyter. Berlin, Boston, pp 69-81. |
| [39] | Schellong K, Schulz S, Harder T, et al. (2012) Birth Weight and Long-Term Overweight Risk: Systematic Review and a Meta-Analysis Including 643,902 Persons from 66 Studies and 26 Countries Globally. PLoS ONE 7(10):1-12. |
| [40] | Horta BL, Bahl Rajiv, Martines JC, et al. (2007) Evidence on the long-term effects of breastfeeding: Systematic reviews and meta-analyses. World Health Organization, Geneva. |
| [41] | Ip S, Chung M, Raman G, et al. (2007) Breastfeeding and maternal and infant health outcomes in developed countries. Evidence report/technology assessment(153):1-186. |
| [42] | Plagemann A, Harder T, Schellong K, et al. (2012) Early postnatal life as a critical time window for determination of long-term metabolic health. Best practice & research. Clin endocrinol & metabol 26(5):641-653. |
| [43] | Günther ALB, Walz H, Kroke A, et al. (2013) Breastfeeding and Its Prospective Association with Components of the GH-IGF-Axis, Insulin Resistance and Body Adiposity Measures in Young Adulthood - Insights from Linear and Quantile Regression Analysis. PLoS ONE 8(11):e79436. |
| [44] | Muntaner C, Sridharan S, Solar O, et al. (2009) Against unjust global distribution of power and money: the report of the WHO commission on the social determinants of health: global inequality and the future of public health policy. J Publi Health Policy 30(2):163-175. |
| [45] |
Uphoff EP, Pickett KE, Cabieses B, et al. (2013) A systematic review of the relationships between social capital and socioeconomic inequalities in health: a contribution to understanding the psychosocial pathway of health inequalities. Int J Equity in Health 12:54. doi: 10.1186/1475-9276-12-54

|
| [46] | World Health Organization (2008) Closing the Gap in a Generation: Health Equity through Action on the Social Determinants of Health. World Health Organization, Geneva |
| [47] | Brown MJ, Sinclair M, Liddle D, et al. (2012) A systematic review investigating healthy lifestyle interventions incorporating goal setting strategies for preventing excess gestational weight gain. PLoS ONE 7(7):e39503. |
| [48] | Muktabhant B, Lawrie TA, Lumbiganon P, et al. (2015) Diet or exercise, or both, for preventing excessive weight gain in pregnancy. Cochrane Dat Syst Rev 6:CD007145. |
| [49] | Lumley J, Chamberlain C, Dowswell T, et al. (2009) Interventions for promoting smoking cessation during pregnancy. Cochrane Dat Syst Rev (3):CD001055. |
| [50] | Chamberlain C, O'Mara-Eves A, Oliver S, et al. (2013) Psychosocial interventions for supporting women to stop smoking in pregnancy. Cochrane Dat Syst Rev 10:CD001055. |
| [51] | Gresham E, Byles JE, Bisquera A, et al. (2014) Effects of dietary interventions on neonatal and infant outcomes: a systematic review and meta-analysis. Am J Clin Nutr 100(5):1298-1321. |
| [52] | Thomas M, Vieten C, Adler N, et al. (2014) Potential for a stress reduction intervention to promote healthy gestational weight gain: focus groups with low-income pregnant women. Women's health issues official publication of the Jacobs Institute of Women's Health 24(3):e305-11. |
| [53] | Renfrew MJ, McCormick FM, Wade A, et al. (2012) Support for healthy breastfeeding mothers with healthy term babies. Cochrane Dat Syst Rev 5:CD001141. |
| [54] | Cleminson J, Oddie S, Renfrew MJ, et al. (2015) Being baby friendly: evidence-based breastfeeding support. Archives of disease in childhood. Fetal and neonatal edition 100(2):F173-8. |
| [55] |
Knoll M, Soller L, Ben-Shoshan M, et al. (2012) The use of incentives in vulnerable populations for a telephone survey: a randomized controlled trial. BMC Res notes 5:572. doi: 10.1186/1756-0500-5-572
|
| [56] | Barlow J, Kirkpatrick S, Stewart-Brown S, et al. (2005) Hard-to-reach or out-of-reach? Reasons why women refuse to take part in early interventions. Children & Society 19(3):199-210. |
| [57] | Barnes J, MacPherson K, Senior R (2006) Factors influencing the acceptance of volunteer home-visiting support offered to families with new babies. Child Family Social Work 11(2):107-117. |
| [58] | Dryden R, Williams B, McCowan C, et al. (2012) What do we know about who does and does not attend general health checks? Findings from a narrative scoping review. BMC Publ Health 12:723. |
| [59] | Hoebel J, Richter M, Lampert T (2013) Social status and participation in health checks in men and women in Germany: results from the German Health Update (GEDA), 2009 and 2010. Deutsches Ärzteblatt Int 110(41):679-685. |
| [60] | Wen LM, Baur LA, Simpson JM, et al. (2012) Effectiveness of home based early intervention on children's BMI at age 2: randomised controlled trial. BMJ 344(jun26 3):e3732. |
| [61] | Gomby, Deanna S. (2005) Home visitation in 2005: Outcomes for children and parents. Invest in Kids Working Paper No. 7, Washington, DC. |
| [62] | Westin M, Westerling R (2007) Social capital and inequality in health between single and couple parents in Sweden. Scand J Publ Health 35(6):609-617. |
| [63] | Olds DL, Kitzman HJ, Cole RE, et al. (2010) Enduring effects of prenatal and infancy home visiting by nurses on maternal life course and government spending: follow-up of a randomized trial among children at age 12 years. Arch Pediatr Adol Med 164(5):419-424. |
| [64] | Kendrick D, Mulvaney CA, Ye L, et al. (2013) Parenting interventions for the prevention of unintentional injuries in childhood. Cochrane Dat Syst Rev 3:CD006020. |
| [65] | Yonemoto N, Dowswell T, Nagai S, et al. (2013) Schedules for home visits in the early postpartum period. Cochrane Dat Syst Rev 7:CD009326. |
| [66] | Filene JH, Kaminski JW, Valle LA, et al. (2013) Components associated with home visiting program outcomes: a meta-analysis. Pediatr 132 Suppl 2:S100-9. |
| [67] | Avellar SA, Supplee LH (2013) Effectiveness of home visiting in improving child health and reducing child maltreatment. Pediatr 132 Suppl 2:S90-9. |
| [68] | Shah MK, Austin KR (2014) Do home visiting services received during pregnancy improve birth outcomes? Findings from Virginia PRAMS 2007-2008. Publ Health Nurs 31(5):405-413. |
| [69] | Ayerle G, Luderer C, Behrens J (2010) Modellprojekt FrühStart - Evaluation der Familienhebammen in Sachsen-Anhalt. Bundesgesundheitsblatt-Gesundheitsforschung-Gesundheitsschutz 53(11):1158-1165. |
| [70] | Ayerle GM (2012) Frühstart: Familienhebammen im Netzwerk Frühe Hilfen, 1st edn., Köln |
| [71] | Lange U, Liebald C (2013) Der Einsatz von Familienhebammen in Netzwerken Früher Hilfen: Leitfaden für Kommunen. BZgA, Köln. |
| [72] | Elm E von, Altman DG, Egger M, et al. (2007) The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. PLoS Med 4(10):e296. |
| [73] | Vandenbroucke JP, Elm E von, Altman DG, et al. (2014) Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): explanation and elaboration. Int J Surg (London, England) 12(12):1500-1524. |
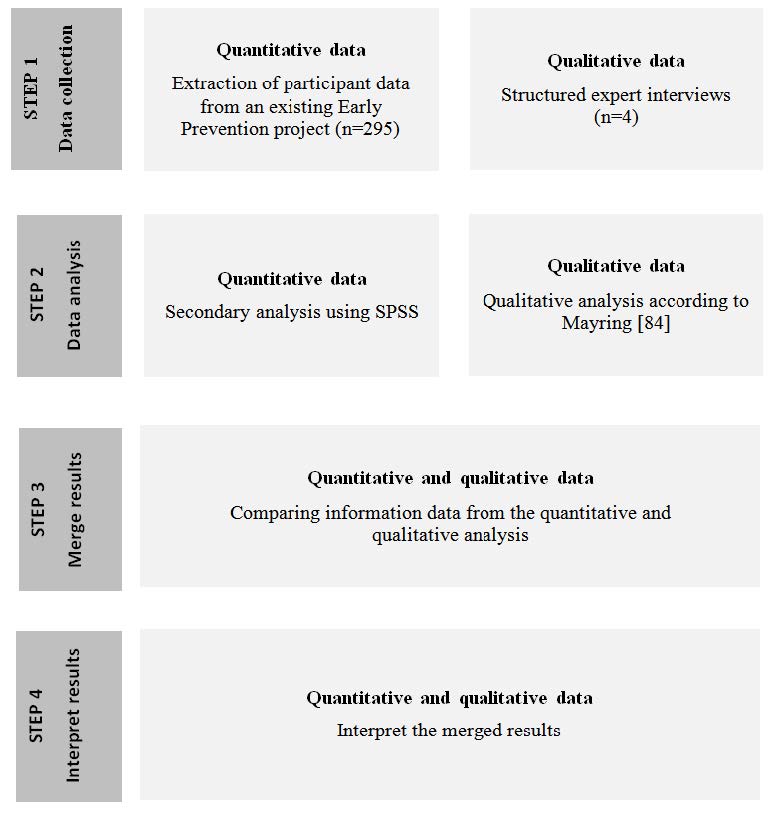
| [74] | Creswell JW, Plano Clark, Vicki L (2011) Designing and conducting mixed methods research, 2nd edn. Sage Publications, Los Angeles. |
| [75] | Bundesministerium für Familie, Senioren, Frauen und Jugend (2006) Frühe Hilfen für Eltern und Kinder und soziale Frühwarnsysteme: Aktionsprogramm des Bundesministeriums für Familie, Senioren, Frauen und Jugend zum Schutz von Kleinkindern, zur Früherkennung von Risiken und Gefährdungen und zur Implementierung effektiver Hilfesysteme. |
| [76] | Hahn M, Sander E (2012) Kompetenzprofil Familienhebammen, 1st edn., Germany, Köln |
| [77] | German Society for Social Medicine and Prevention, German Society for Epidemiology (2012) Good Practice Secondary Data Analysis. Available from: http://dgepi.de/fileadmin/pdf/leitlinien/GPS_fassung3.pdf. |
| [78] | Bogner A, Littig B, Menz W (2009) Interviewing Experts. Palgrave Macmillan, Basingstoke. |
| [79] | Littig B, Pochhacker F (2014) Socio-Translational Collaboration in Qualitative Inquiry: The Case of Expert Interviews. Qualitative Inquiry 20(9):1085-1095. |
| [80] | German Sociological Association (1992) Ethical Code of the German Sociological Association: revised in 2014. Available from: http://soziologie.univie.ac.at/fileadmin/user_upload/inst_soziologie/DGS_Ethik.pdf; http://www.soziologie.de/uploads/media/Ethik-Kodex_2014-06-14.pdf. |
| [81] | Helfferich C (2011) Die Qualität qualitativer Daten: Manual für die Durchführung qualitativer Interviews, 4th edn. Verlag für Sozialwissenschaften, Wiesbaden. |
| [82] | Kowal S, O'Connell Daniel (2009) Zur Transkription von Gesprächen, In: Flick U, Kardorff Ev, Steinke I (eds) Qualitative Forschung: Ein Handbuch, 7th edn.: Rowohlt Taschenbuch-Verlag. Reinbek bei Hamburg, pp 437-447. |
| [83] | Bortz J, Döring N (2006) Forschungsmethoden und Evaluation: Für Human- und Sozialwissenschaftler, 4th edn. Springer Medizin Verlag Heidelberg, Berlin, Heidelberg. |
| [84] | Mayring P (2010) Qualitative Inhaltsanalyse: Grundlagen und Techniken, 11th edn. Beltz, Weinheim. |
| [85] | Scharte M, Bolte G (2012) Kinder alleinerziehender Frauen in Deutschland: Gesundheitsrisiken und Umweltbelastungen. Das Gesundheitswesen 74(03):123-131. |
| [86] | Osborne C, McLanahan S (2007) Partnership Instability and Child Well-Being. J MarrFam 69(4):1065-1083. |
| [87] | Yanicki S (2005) Social support and family assets: the perceptions of low-income lone-mother families about support from home visitation. Can Journal Publ Health 96(1):46-49. |
| [88] | Crosier T, Butterworth P, Rodgers B (2007) Mental health problems among single and partnered mothers. Soc Psychi Epidemiol 42(1):6-13. |
| [89] | Bilszta JL, Tang M, Meyer D, et al. (2008) Single motherhood versus poor partner relationship: outcomes for antenatal mental health. Aust NZ J Psychiat 42(1):56-65. |
| [90] | Olds DL, Kitzman H, Hanks C, et al. (2007) Effects of nurse home visiting on maternal and child functioning: age-9 follow-up of a randomized trial. Pediatrics 120(4):e832-45. |
| [91] | Zierau J, Gonzáles-C I, Blume E, et al. (2005) Modellprojekt: Aufsuchende Familienhilfe für junge Mütter - Netzwerk Familienhebammen. Ergebn der Eval, Hannover. |
| [92] | Steinmann M (2008) Was wissen Hebammen über Ernährung? Eine empirische Analyse. Ernährungs Umschau 55(1):12-15. |
| [93] | Kitzman H, Olds DL, Henderson CR, et al. (1997) Effect of prenatal and infancy home visitation by nurses on pregnancy outcomes, childhood injuries, and repeated childbearing. A randomized controlled trial. JAMA 278(8):644-652. |
| [94] | Arenz S, Rückerl R, Koletzko B, et al. (2004) Breast-feeding and childhood obesity—a systematic review. Int J Obes 28(10):1247-1256. |
| [95] | Owen CG, Martin RM, Whincup PH, et al. (2005) Effect of infant feeding on the risk of obesity across the life course: a quantitative review of published evidence. Pediatr115(5):1367-1377. |
| [96] | Harder T, Bergmann R, Kallischnigg G, et al. (2005) Duration of breastfeeding and risk of overweight: a meta-analysis. Am J Epidemiol 162(5):397-403. |
| [97] | Weng SF, Redsell SA, Swift JA, et al. CP (2012) Systematic review and meta-analyses of risk factors for childhood overweight identifiable during infancy. Arch Dis Childhood 97(12):1019-1026. |
| [98] | Taylor JS, Kacmar JE, Nothnagle M, et al. (2005) A systematic review of the literature associating breastfeeding with type 2 diabetes and gestational diabetes. J Am Coll Nutr 24(5):320-326. |
| [99] | Gouveri E, Papanas N, Hatzitolios AI, et al. (2011) Breastfeeding and diabetes. Curr Diabet Rev7(2):135-142. |
| [100] | Manco M, Alterio A, Bugianesi E, et al. (2011) Insulin dynamics of breast- or formula-fed overweight and obese children. J Am Coll Nutr 30(1):29-38. |
| [101] | Martorell R, Zongrone A (2012) Intergenerational Influences on Child Growth and Undernutrition. Paediatr Perinat Ep 26:302-314. |
| [102] | Grebmer K von, Headey D, Olofinbiyi T, et al. (2013) Welthunger-Index: Herausforderung Hunger: Widerstandsfähigkeit sicher, Ernährung sichern, Bonn / Washington, DC / Dublin. |
| [103] | Uauy R, Kain J, Corvalan C (2011) How can the Developmental Origins of Health and Disease (DOHaD) hypothesis contribute to improving health in developing countries? Am J Clin Nutr 94(6_Suppl):1759S. |
| [104] | Sanchez-Villegas A, Martínez JA, Prättälä R, et al. (2003) A systematic review of socioeconomic differences in food habits in Europe: consumption of cheese and milk. Europ J Clin Nutr 57(8):917-929. |
| [105] | Mensink G, Truthmann J, Rabenberg M, et al. (2013) Obst- und Gemüsekonsum in Deutschland. Bundesgesundheitsblatt-Gesundheitsforschung-Gesundheitsschutz 56(5-6):779-785. |
| [106] | Simoes E, Kunz S, Bosing-Schwenkglenks M, et al. (2004) Untersuchung auf der Basis der Perinatalerhebung Baden-Württemberg - Psychosoziale Risikofaktoren in der Schwangerschaft. Psychoneuro 30(6):342-347. |
| [107] | Koller D, Lack N, Mielck A (2009) Soziale Unterschiede bei der Inanspruchnahme der Schwangerschafts-Vorsorgeuntersuchungen, beim Rauchen der Mutter während der Schwangerschaft und beim Geburtsgewicht des Neugeborenen. Empirische Analyse auf Basis der Bayerischen Perinatal-Studie. Das Gesundheitswesen 71(01):10-18. |
| [108] | Simoes E, Kunz SK (2011) Der leise Confounder Armut macht krank: Gesundheitliche Ungleichheit in der geburtshilflichen Versorgung. Arbeitsmedizin Sozialmedizin Umweltmedizin 46(11):629-635. |
| [109] | Kitzman HJ, Olds DL, Cole RE, et al. (2010) Enduring effects of prenatal and infancy home visiting by nurses on children: follow-up of a randomized trial among children at age 12 years. Arch Pediat Adol Med 164(5):412-418. |
| [110] | Sadler GR, Lee H, Lim RS, et al. (2010) Research Article: Recruitment of hard-to-reach population subgroups via adaptations of the snowball sampling strategy. Nurs Health Sci 12(3):369-374. |
| [111] | Ofstedal MB, Weir DR (2011) Recruitment and retention of minority participants in the health and retirement study. Gerontol 51 Suppl 1:S8-20. |
| [112] | Spears CR, Nolan BV, O'Neill JL, et al. (2011) Recruiting underserved populations to dermatologic research: a systematic review. Int J Dermatol 50(4):385-395. |
| [113] | Fracasso PM, Goodner SA, Creekmore AN, et al. (2013) Coaching intervention as a strategy for minority recruitment to cancer clinical trials. J Oncol Pract 9(6):294-299. |
Figures(2) / Tables(4)

Helena Walz, Barbara Bohn, Jessica Sander, Claudia Eberle, Monika Alisch, Bernhard Oswald, Anja Kroke. Access to Difficult-to-reach Population Subgroups: A Family Midwife Based Home Visiting Service for Implementing Nutrition-related Preventive Activities - A Mixed Methods Explorative Study[J]. AIMS Public Health, 2015, 2(3): 516-536. doi: 10.3934/publichealth.2015.3.516







 DownLoad:
DownLoad: