A significant percentage of the population must be vaccinated to achieve herd immunity. Therefore the success of a vaccination program relies on the level of acceptance. This present study seeks to understand COVID-19 vaccine acceptance and hesitancy in Nigeria by assessing the public's willingness to get vaccinated.
This is a population-based cross-sectional study. Data were derived through a structured online survey.
A cross-sectional study was conducted among adult residents in Nigeria in March 2021 using a structured online questionnaire. The questionnaire surveyed participants' demographic characteristics and perception of COVID-19 and the COVID-19 vaccine. Descriptive statistics and inferential statistics using Chi-square, as well as univariable logistic regression to determine the factors associated with acceptance of COVID-19 vaccine was conducted.
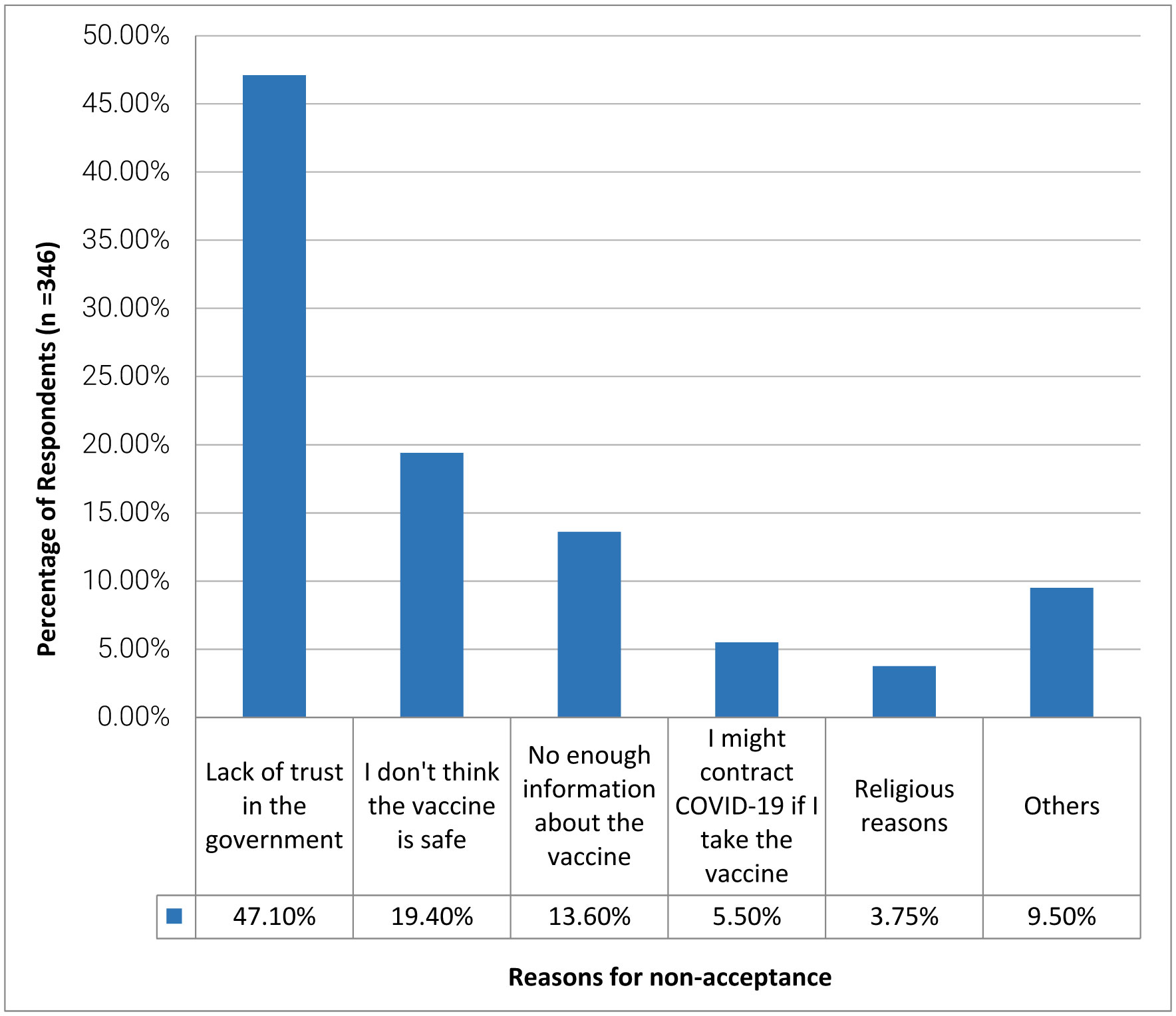
Of the 618 respondents, 272 (44%) reported being willing to get vaccinated. Interestingly, of the 346 (56%) respondents that would not take the COVID-19 vaccine, the highest marginal reasons for non-acceptance were lack of trust in the government 163 (47.1%), followed by the belief that the vaccine is not safe 67 (19.4%), and no enough information about the vaccine 49 (13.6%). In addition, male respondents and those with a university degree or above were statistically significantly more likely to accept a COVID-19 vaccine.
A considerable proportion of the study population is unwilling to receive a COVID-19 vaccine. This observation highlights the need for the government, public health officials, and advocacy groups to implement immediate awareness-raising measures to sway the public towards COVID-19 vaccine acceptance.
Citation: Osmond C. Ekwebelem, Helen Onyeaka, Ismaeel Yunusa, Taghi Miri, Yahwedalu M. Onwuneme, Ayeni T. Eunice, Amara Anyogu, Bright Obi, Ngwogu Ada Carol. Do we trust the government? Attributes of COVID-19 vaccine hesitancy and acceptance in Nigeria[J]. AIMS Medical Science, 2022, 9(2): 268-282. doi: 10.3934/medsci.2022010
A significant percentage of the population must be vaccinated to achieve herd immunity. Therefore the success of a vaccination program relies on the level of acceptance. This present study seeks to understand COVID-19 vaccine acceptance and hesitancy in Nigeria by assessing the public's willingness to get vaccinated.
This is a population-based cross-sectional study. Data were derived through a structured online survey.
A cross-sectional study was conducted among adult residents in Nigeria in March 2021 using a structured online questionnaire. The questionnaire surveyed participants' demographic characteristics and perception of COVID-19 and the COVID-19 vaccine. Descriptive statistics and inferential statistics using Chi-square, as well as univariable logistic regression to determine the factors associated with acceptance of COVID-19 vaccine was conducted.
Of the 618 respondents, 272 (44%) reported being willing to get vaccinated. Interestingly, of the 346 (56%) respondents that would not take the COVID-19 vaccine, the highest marginal reasons for non-acceptance were lack of trust in the government 163 (47.1%), followed by the belief that the vaccine is not safe 67 (19.4%), and no enough information about the vaccine 49 (13.6%). In addition, male respondents and those with a university degree or above were statistically significantly more likely to accept a COVID-19 vaccine.
A considerable proportion of the study population is unwilling to receive a COVID-19 vaccine. This observation highlights the need for the government, public health officials, and advocacy groups to implement immediate awareness-raising measures to sway the public towards COVID-19 vaccine acceptance.

| [1] | World Health Organization (WHO)COVID-19 vaccine tracker and landscape (2020). Available from: https://www.who.int/publications/m/item/draft-landscape-of-covid-19-candidate-vaccines |
| [2] |
Apolone G, Montomoli E, Manenti A, et al. (2021) Unexpected detection of SARS-CoV-2 antibodies in the prepandemic period in Italy. Tumori J 107: 446-451. https://doi.org/10.1177/0300891620974755 
|
| [3] |
La Rosa G, Mancini P, Ferraro GB, et al. (2021) SARS-CoV-2 has been circulating in northern Italy since December 2019: evidence from environmental monitoring. Sci Total Environ 750: 141711. https://doi.org/10.1016/j.scitotenv.2020.141711
|
| [4] | Al-Sharify ZT, Nussrat HH, Al-Najjar SZ, et al. (2021) The emergence of COVID-19 and its pandemic potentialas a global health security threat and its effect on future life strategy. System Rev Pharm 12: 259-269. |
| [5] |
Ekwebelem OC, Ofielu ES, Nnorom-Dike OV, et al. (2021) Threats of COVID-19 to achieving united nations sustainable development goals in Africa. Am J Trop Med Hyg 104: 457-460. https://doi.org/10.4269/ajtmh.20-1489
|
| [6] |
Lazarus JV, Ratzan SC, Palayew A, et al. (2021) A global survey of potential acceptance of a COVID-19 vaccine. Nat Med 27: 225-228. https://doi.org/10.1038/s41591-020-1124-9
|
| [7] |
Yunusa I, Iloanusi S, Mgbere O, et al. (2021) Public opinion regarding government response to COVID-19: case study of a large commercial city in Nigeria. Pan Afr Med J 38: 282. https://doi.org/10.11604/pamj.2021.38.282.26361
|
| [8] |
Ekwebelem OC, Yunusa I, Onyeaka H, et al. (2021) COVID-19 vaccine rollout: will it affect the rates of vaccine hesitancy in Africa?. Public Health 197: e18-e19. https://doi.org/10.1016/j.puhe.2021.01.010
|
| [9] |
Adepoju P (2020) Nigeria responds to COVID-19; first case detected in sub-Saharan Africa. Nat Med 26: 444-448. https://doi.org/10.1038/d41591-020-00004-2
|
| [10] |
Kalu B (2020) COVID-19 in Nigeria: a disease of hunger. Lancet Respir Med 8: 556-557. https://doi.org/10.1016/S2213-2600(20)30220-4
|
| [11] | Nigeria Center for Disease Control (NCDC)COVID-19 outbreak in Nigeria situation report (2020). Available from: https://ncdc.gov.ng/themes/common/files/%20annualreports/18803aba62a09ada4ad84c8db76c22ea.pdf |
| [12] | Africa CDCCoronavirus Disease 2019 (COVID-19) latest updates on the COVID-19 crisis from Africa CDC (2021). Available from: https://africacdc.org/covid-19/ |
| [13] | World Health Organization (WHO)Strategic Advisory Group of Experts on Immunisation. Report of the SAGE working group on vaccine hesitancy. [cited 14th March 2022] (2021). Available from: https://www.medbox.org/document/report-of-the-sage-working-group-on-vaccine-hesitancy#GO |
| [14] |
Lozano R, Naghavi M, Foreman K, et al. (2012) Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 380: 2095-2128. https://doi.org/10.1016/S0140-6736(12)61728-0
|
| [15] | Aborode AT, Fajemisin EA, Ekwebelem OC, et al. (2021) Vaccine hesitancy in Africa: causes and strategies to the rescue. Ther Adv Vaccines Immunother 9: 25151355211047514. https://doi.org/10.1177/25151355211047514 |
| [16] |
Onyeaka H, Al-Sharify ZT, Ghadhban MY, et al. (2021) A review on the advancements in the development of vaccines to combat coronavirus disease 2019. Clin Exp Vaccine Res 10: 6-12. https://doi.org/10.7774/cevr.2021.10.1.6
|
| [17] |
Adebisi YA, Prisno DEL, Nuga BB (2020) Last fight of wild polio in Africa: Nigeria's battle. Public Health Pract 1: 100043. https://doi.org/10.1016/j.puhip.2020.100043
|
| [18] |
Ekwebelem OC, Nnorom-Dike OV, Aborode AT, et al. (2021) Eradication of wild poliovirus in Nigeria: lessons learnt. Public Health Pract 2: 100144. https://doi.org/10.1016/j.puhip.2021.100144
|
| [19] |
Malik AA, McFadden SM, Elharake J, et al. (2020) Determinants of COVID-19 vaccine acceptance in the US. EClinicalMedicine 26: 100495. https://doi.org/10.1016/j.eclinm.2020.100495
|
| [20] |
Adebisi YA, Alaran AJ, Bolarinwa OA, et al. (2021) When it is available, will we take it? Social media users' perception of hypothetical COVID-19 vaccine in Nigeria. Pan Afr Med J 38: 230. https://doi.org/10.11604/pamj.2021.38.230.27325
|
| [21] |
Larson HJ, Clarke RM, Jarrett C, et al. (2018) Measuring trust in vaccination: A systematic review. Hum Vaccin Immunother 14: 1599-1609. https://doi.org/10.1080/21645515.2018.1459252
|
| [22] |
Flaxman S, Mishra S, Gandy A, et al. (2020) Estimating the effects of non-pharmaceutical interventions on COVID-19 in Europe. Nature 584: 257-261. https://doi.org/10.1038/s41586-020-2405-7
|
| [23] |
Sanche S, Lin YT, Xu C, et al. (2020) High contagiousness and rapid spread of severe acute respiratory syndrome coronavirus 2. Emerg Infect Dis 26: 1470-1477. https://doi.org/10.3201/eid2607.200282
|
| [24] | IPSOSThree in four adults globally say they would get a vaccine for COVID-19. [14th March 2022] (2020). Available from: https://www.ipsos.com/en/three-four-adults-globally-say-theyd-get-vaccine-covid-19 |
| [25] |
Neumann-Böhme S, Varghese NE, Sabat I, et al. (2020) Once we have it, will we use it? A European survey on willingness to be vaccinated against COVID-19. Eur J Health Econ 21: 977-982. https://doi.org/10.1007/s10198-020-01208-6
|
| [26] |
Harapan H, Wagner AL, Yufika A, et al. (2020) Acceptance of a COVID-19 vaccine in Southeast Asia: A cross-sectional study in Indonesia. Front Public Health 8: 381. https://doi.org/10.3389/fpubh.2020.00381
|
| [27] |
Wong LP, Alias H, Wong PF, et al. (2020) The use of the health belief model to assess predictors of intent to receive the COVID-19 vaccine and willingness to pay. Hum Vaccin Immunother 16: 2204-2214. https://doi.org/10.1080/21645515.2020.1790279
|
| [28] |
Nzaji MK, Ngombe LK, Mwamba GN, et al. (2020) Acceptability of vaccination against COVID-19 among healthcare workers in the Democratic Republic of the Congo. Pragmat Obs Res 11: 103-109. https://doi.org/10.2147/POR.S271096
|
| [29] | Thorneloe R, Wilcockson H, Lamb M, et al. (2020) Willingness to receive a COVID-19 vaccine among adults at high-risk of COVID-19: a UK-wide survey. PsyArXiv Preprints . https://doi.org/10.31234/osf.io/fs9wk |
| [30] |
Dodd RH, Cvejic E, Bonner C, et al. (2021) Willingness to vaccinate against COVID-19 in Australia. Lancet Infect Dis 21: 318-319. https://doi.org/10.1016/S1473-3099(20)30559-4
|
| [31] |
Kourlaba G, Kourkouni E, Maistreli S, et al. (2021) Willingness of Greek general population to get a COVID-19 vaccine. Glob Health Res Policy 6: 1-10. https://doi.org/10.1186/s41256-021-00188-1
|
| [32] | European Centre for Disease Prevention and Control (ECDC)Catalogue of interventions addressing vaccine hesitancy (2017). Available from: https://www.ecdc.europa.eu/sites/default/files/documents/Catalogue-interventions-vaccine-hesitancy.pdf |
| [33] |
Thomson A, Vallee-Tourangeau G, Suggs LS (2018) Strategies to increase vaccine acceptance and uptake: From behavioral insights to context-specific, culturally-appropriate, evidence-based communications and interventions. Vaccine 36: 6457-6458. https://doi.org/10.1016/j.vaccine.2018.08.031
|
| [34] |
Betsch C, Schmid P, Heinemeier D, et al. (2018) Beyond confidence: development of a measure assessing the 5C psychological antecedents of vaccination. PloS One 13: e0208601. https://doi.org/10.1371/journal.pone.0208601
|
| [35] |
Siegrist M, Zingg A (2014) The role of public trust during pandemics: implications for crisis communication. Eur Psychol 19: 23-32. https://doi.org/10.1027/1016-9040/a000169
|
| [36] |
Eysenbach G (2004) Improving the quality of web surveys: the checklist for reporting results of internet e-surveys (CHERRIES). J Med Internet Res 6: e34. https://doi.org/10.2196/jmir.6.3.e34
|
| [37] |
Wyatt J (2000) When to use web-based surveys. J Am Med Inform Assoc 7: 426-429. https://doi.org/10.1136/jamia.2000.0070426
|
Figures(2) / Tables(2)

Osmond C. Ekwebelem, Helen Onyeaka, Ismaeel Yunusa, Taghi Miri, Yahwedalu M. Onwuneme, Ayeni T. Eunice, Amara Anyogu, Bright Obi, Ngwogu Ada Carol. Do we trust the government? Attributes of COVID-19 vaccine hesitancy and acceptance in Nigeria[J]. AIMS Medical Science, 2022, 9(2): 268-282. doi: 10.3934/medsci.2022010







 DownLoad:
DownLoad: