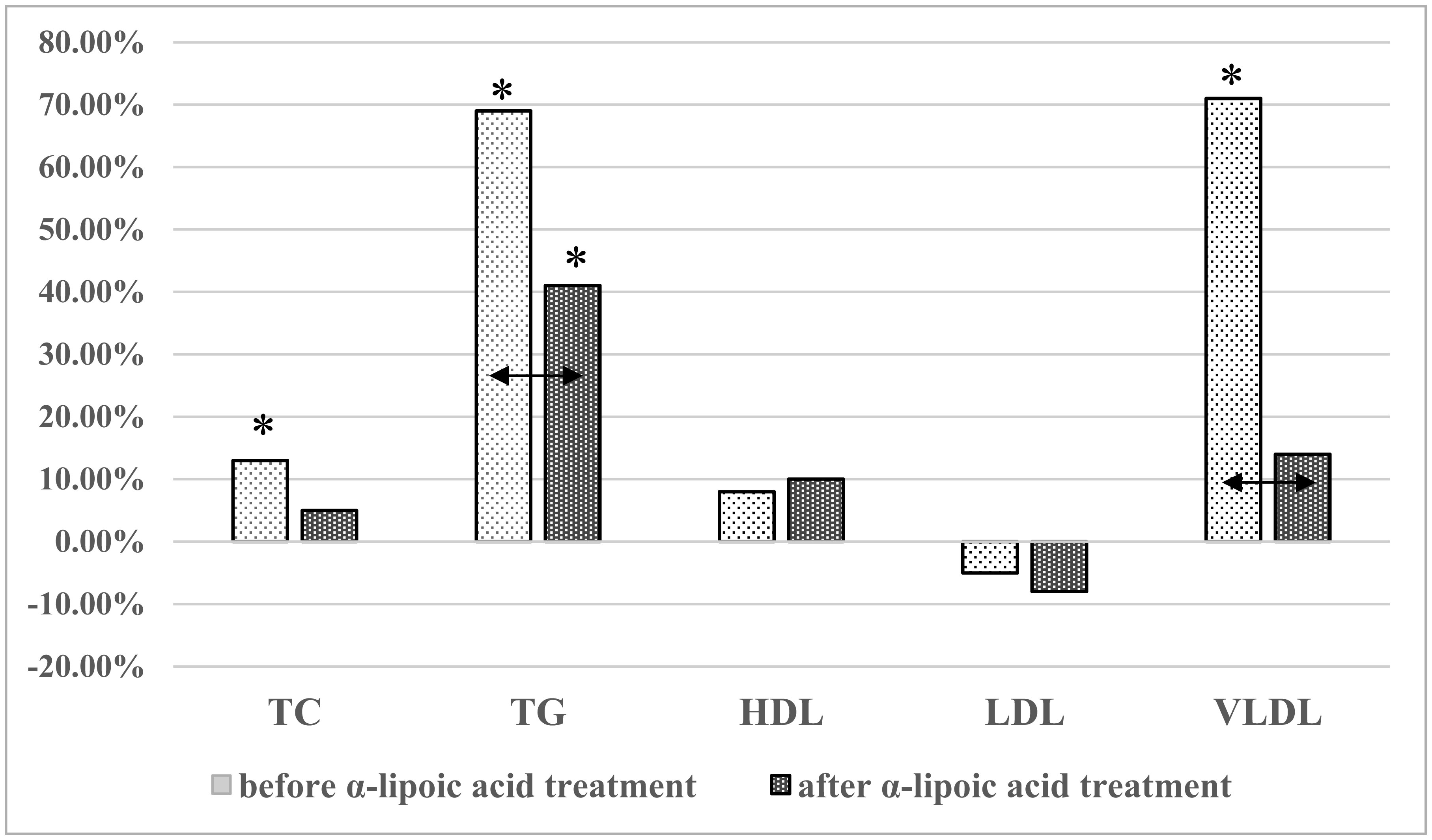
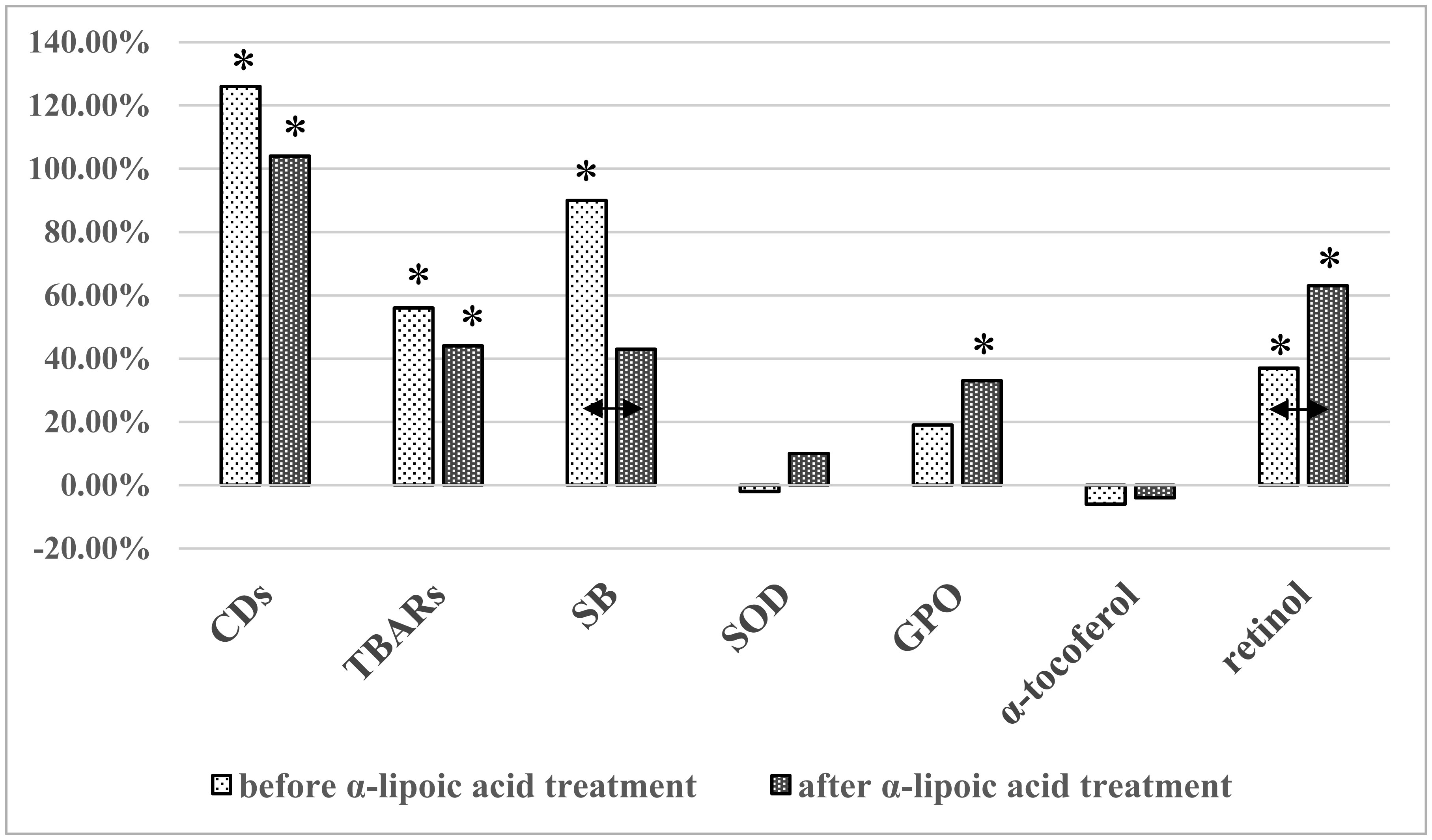
In various pathological conditions such as diabetes mellitus, the cellular redox balance can be disturbed and these alterations may persist even after blood glucose levels have returned to normal. Antioxidant therapies, including α-lipoic acid, are widely used to treat various systemic diseases including diabetes mellitus. The aim of this study was to measure the lipid metabolism parameters, as well as the activity of lipid peroxidation and antioxidant defense reactions, in men with type 1 diabetes mellitus (T1DM) during treatment with α-lipoic acid. Twenty-four reproductive-age T1DM males with an unsatisfactory glycemic profile were examined. Twenty-eight practically healthy men of similar age were used as the control group. Spectrophotometric, fluorometric, and enzyme-linked immunoassay methods were used. T1DM was characterized by increased values of lipid metabolism components, including total cholesterol, triacylglycerides (TG), and very-low-density lipoproteins (VLDL). In the lipid peroxidation system, increased levels of the primary products (conjugated dienes), secondary products (thiobarbituric acid reactants), and final products (Schiff bases) were observed in T1DM patients compared to the control group. Retinol values were also increased. After treatment, there was a decrease in TG, VLDL, and Schiff bases levels and an increase in the retinol level compared to before treatment. These results expand our understanding of the pathogenetic mechanisms of T1DM and suggest that α-LA treatment may be beneficial for type 1 diabetics.
Citation: Marina A. Darenskaya, Elena V. Chugunova, Sergey I. Kolesnikov, Natalja V. Semenova, Olga A. Nikitina, Lyubov I. Kolesnikova. Lipid peroxidation processes in men with type 1 diabetes mellitus following α-lipoic acid treatment[J]. AIMS Medical Science, 2021, 8(4): 291-300. doi: 10.3934/medsci.2021024
In various pathological conditions such as diabetes mellitus, the cellular redox balance can be disturbed and these alterations may persist even after blood glucose levels have returned to normal. Antioxidant therapies, including α-lipoic acid, are widely used to treat various systemic diseases including diabetes mellitus. The aim of this study was to measure the lipid metabolism parameters, as well as the activity of lipid peroxidation and antioxidant defense reactions, in men with type 1 diabetes mellitus (T1DM) during treatment with α-lipoic acid. Twenty-four reproductive-age T1DM males with an unsatisfactory glycemic profile were examined. Twenty-eight practically healthy men of similar age were used as the control group. Spectrophotometric, fluorometric, and enzyme-linked immunoassay methods were used. T1DM was characterized by increased values of lipid metabolism components, including total cholesterol, triacylglycerides (TG), and very-low-density lipoproteins (VLDL). In the lipid peroxidation system, increased levels of the primary products (conjugated dienes), secondary products (thiobarbituric acid reactants), and final products (Schiff bases) were observed in T1DM patients compared to the control group. Retinol values were also increased. After treatment, there was a decrease in TG, VLDL, and Schiff bases levels and an increase in the retinol level compared to before treatment. These results expand our understanding of the pathogenetic mechanisms of T1DM and suggest that α-LA treatment may be beneficial for type 1 diabetics.
Antioxidant defense
Body mass index
Conjugated dienes
Diabetes mellitus
Deoxyribonucleic acid
Glycosylated hemoglobin
High-density lipoproteins
Glutathione peroxidase
Low-density lipoproteins
Lipid peroxidation
Oxidative stress
Reactive oxygen species
Superoxide dismutase
Type 1 diabetes mellitus
Thiobarbituric acid reactants
Total cholesterol
Riacylglycerides
Schiff bases
Very-low-density lipoproteins
World health organization
α-lipoic acid

| [1] |
Harding JL, Pavkov ME, Magliano DJ, et al. (2019) Global trends in diabetes complications: a review of current evidence. Diabetologia 62: 3-16. doi: 10.1007/s00125-018-4711-2

|
| [2] |
Cho N, Shaw JE, Karuranga S, et al. (2018) IDF diabetes Atlas: global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res Clin Pract 138: 271-281. doi: 10.1016/j.diabres.2018.02.023
|
| [3] |
Dedov II, Shestakova MV, Vikulova OK, et al. (2018) Diabetes mellitus in the Russian Federation: prevalence, morbidity, mortality, parameters of carbohydrate metabolism and the structure of hypoglycemic therapy according to the Federal Register of Diabetes Mellitus, status 2017. Diabetes Mellit 21: 144-159. doi: 10.14341/DM9686
|
| [4] |
Shestakova MV, Mokrysheva NG, Dedov II (2020) Course and treatment of diabetes mellitus in the context of COVID-19. Diabetes Mellit 23: 132-139. doi: 10.14341/DM12418
|
| [5] | Sies H (2020) Oxidative eustress and oxidative distress: Introductory remarks Academic Press. |
| [6] |
Forrester SJ, Kikuchi DS, Hernandes MS, et al. (2018) Reactive oxygen species in metabolic and inflammatory signaling. Circ Res 122: 877-902. doi: 10.1161/CIRCRESAHA.117.311401
|
| [7] |
Sies H (2020) Oxidative stress: concept and some practical aspects. Antioxidants 9: 852. doi: 10.3390/antiox9090852
|
| [8] |
Sifuentes-Franco S, Pacheco-Moisés FP, Rodríguez-Carrizalez AD, et al. (2017) The role of oxidative stress, mitochondrial function, and autophagy in diabetic polyneuropathy. J Diabetes Res 2017. doi: 10.1155/2017/1673081
|
| [9] |
Lavender N, Hein DW, Brock G, et al. (2015) Evaluation of oxidative stress response related genetic variants, pro-oxidants, antioxidants and prostate cancer. AIMS Med Sci 2: 271. doi: 10.3934/medsci.2015.4.271
|
| [10] | Chandra K, Singh P, Dwivedi S, et al. (2019) Diabetes mellitus and oxidative stress: a co-relative and therapeutic approach. J Clin Diagnostic Res 13. |
| [11] |
Darenskaya MA, Kolesnikova LI, Kolesnikov SI (2021) Oxidative stress: pathogenetic role in the development of diabetes mellitus and its complications, therapeutic approaches to correction. Bull Exp Biol Med 171: 179-189. doi: 10.1007/s10517-021-05191-7
|
| [12] |
Hirakawa Y, Tanaka T, Nangaku M (2017) Mechanisms of metabolic memory and renal hypoxia as a therapeutic target in diabetic kidney disease. J Diabetes Investig 8: 261-271. doi: 10.1111/jdi.12624
|
| [13] |
Ceriello A, Testa R, Genovese S (2016) Clinical implications of oxidative stress and potential role of natural antioxidants in diabetic vascular complications. Nutr Metab Cardiovasc Dis 26: 285-292. doi: 10.1016/j.numecd.2016.01.006
|
| [14] | Mendoza-Núñez VM, García-Martínez BI, Rosado-Pérez J, et al. (2019) The effect of 600 mg alpha-lipoic acid supplementation on oxidative stress, inflammation, and RAGE in older adults with type 2 diabetes mellitus. Oxid Med Cell Longev 2019. |
| [15] |
Corongiu FP, Banni S (1994) Detection of conjugated dienes by second derivative ultraviolet spectrophotometry. Methods Enzymol 233: 303-310. doi: 10.1016/S0076-6879(94)33033-6
|
| [16] |
Asakawa T, Matsushita S (1980) Coloring conditions of thiobarbituric acid test for detecting lipid hydroperoxides. Lipids 15: 137-140. doi: 10.1007/BF02540959
|
| [17] |
Shimasaki H, Hirai N, Ueta N (1988) Comparison of fluorescence characteristics of products of peroxidation of membrane phospholipids with those of products derived from reaction of malonaldehyde with glycine as a model of lipofuscin fluorescent substances. J Biochem 104: 761-766. doi: 10.1093/oxfordjournals.jbchem.a122546
|
| [18] | Chernyauskene RCh, Varshkyavichene ZZ, Gribauskas S (1984) Simultaneous determination of the concentrations of vitamins E and A in the serum. Laboratornoe Delo 6: 362-365. (Article in Russian). |
| [19] |
Chowdary RP, Praveen D, Aanandhi VM (2017) A prospective study on incidence of dyslipidemia in diabetes mellitus. Res J Pharm Technol 10: 431-433. doi: 10.5958/0974-360X.2017.00086.5
|
| [20] |
Kolesnikova LI, Darenskaya MA, Grebenkina LA, et al. (2019) Ethnic aspects of lipid peroxidation process flow in patients with type 1 diabetes mellitus. Diabetes Technol The 21: 133. doi: 10.1089/dia.2018.0347
|
| [21] |
Kolesnikova LI, Kolesnikov SI, Darenskaya MA, et al. (2015) Lipid status and predisposing genes in patients with diabetes mellitus type 1 from various ethnic groups. Bull Exp Biol Med 160: 278-280. doi: 10.1007/s10517-015-3149-5
|
| [22] |
Maahs DM, Ogden LG, Dabelea D, et al. (2010) Association of glycaemia with lipids in adults with type 1 diabetes: modification by dyslipidaemia medication. Diabetologia 53: 2518-2525. doi: 10.1007/s00125-010-1886-6
|
| [23] |
Mach F, Baigent C, Catapano AL, et al. (2019) 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Atherosclerosis 290: 140-205. doi: 10.1016/j.atherosclerosis.2019.08.014
|
| [24] | Darenskaya MA, Grebenkina LA, Semenova NV, et al. (2018) The use of integral indicator of oxidative stress in women with diabetes mellitus. Diabetes Technol The 20: 143-144. |
| [25] |
Darenskaya MA, Shemyakina NA, Namokonov EV, et al. (2020) Glyoxal, metilglyoxal and malonic dialdehyde levels in patients with diabetes mellitus and microangiopathy of the lower extremities in the course of recommended therapy with added N-acetylcysteine. Diabetes Technol The 22: 760. doi: 10.1089/dia.2019.0509
|
| [26] |
Asadipooya K, Uy EM (2019) Advanced glycation end products (AGEs), receptor for AGEs, diabetes, and bone: review of the literature. J Endocr Soc 3: 1799-1818. doi: 10.1210/js.2019-00160
|
| [27] |
Sies H, Jones DP (2020) Reactive oxygen species (ROS) as pleiotropic physiological signalling agents. Nat Rev Mol Cell Biol 21: 363-383. doi: 10.1038/s41580-020-0230-3
|
| [28] | Lankin VZ, Tikhaze AK, Konovalova GG, et al. (2018) Oxidative and carbonyl stress as a factors of the modification of proteins and DNA destruction in diabetes. Ter Arkh 90: 46-50. |
| [29] | Kolesnikova LI, Shemyakina NA, Namokonov EV, et al. (2019) Some parameters of carbonyl and oxidative stress in patients with type 2 diabetes mellitus and macroangiopathy of the lower extremities. Diabetes Technol The 21: 46. |
| [30] |
Kolesnikova LI, Darenskaya MA, Semenova NV, et al. (2015) Lipid peroxidation and antioxidant protection in girls with type 1 diabetes mellitus during reproductive system development. Medicina 51: 107-111. doi: 10.1016/j.medici.2015.01.009
|
| [31] |
Kolesnikova LI, Vlasov BY, Kolesnikov SI, et al. (2016) Intensity of oxidative stress in Mongoloid and Caucasian patients with type 1 diabetes mellitus. Bull Exp Biol Med 161: 767-769. doi: 10.1007/s10517-016-3505-0
|
| [32] |
Wentholt IME, Kulik W, Michels RPJ, et al. (2008) Glucose fluctuations and activation of oxidative stress in patients with type 1 diabetes. Diabetologia 51: 183-190. doi: 10.1007/s00125-007-0842-6
|
| [33] |
Ito F, Sono Y, Ito T (2019) Measurement and clinical significance of lipid peroxidation as a biomarker of oxidative stress: oxidative stress in diabetes, atherosclerosis, and chronic inflammation. Antioxidants 8: 72. doi: 10.3390/antiox8030072
|
| [34] | Teichert J, Kern J, Tritschler HJ, et al. (1998) Investigations on the pharmacokinetics of alpha-lipoic acid in healthy volunteers. Int J Clin Pharmacol Ther 36: 625-628. |
| [35] | Carlson DA, Smith AR, Fischer SJ, et al. (2007) The plasma pharmacokinetics of R-(+)-lipoic acid administered as sodium R-(+)-lipoate to healthy human subjects. Altern Med Rev 12: 343-351. |
| [36] |
Khan A, Iqbal Z, Watson DG, et al. (2011) Simultaneous determination of lipoic acid (LA) and dihydrolipoic acid (DHLA) in human plasma using high–performance liquid chromatography coupled with electrochemical detection. J Chromatogr B Analyt Technol Biomed Life Sci 879: 1725-1731. doi: 10.1016/j.jchromb.2011.04.017
|
| [37] |
Scaramuzza A, Giani E, Redaelli F, et al. (2015) Alpha–lipoic acid and antioxidant diet help to improve endothelial dysfunction in adolescents with type 1 diabetes: a pilot trial. J Diabetes Res 2015. doi: 10.1155/2015/474561
|
| [38] |
Derosa G, D'Angelo A, Romano D, et al. (2016) A clinical trial about a food supplement containing α–lipoic acid on oxidative stress markers in type 2 diabetic patients. Int J Mol Sci 17: 1802. doi: 10.3390/ijms17111802
|
Figures(2) / Tables(1)

Marina A. Darenskaya, Elena V. Chugunova, Sergey I. Kolesnikov, Natalja V. Semenova, Olga A. Nikitina, Lyubov I. Kolesnikova. Lipid peroxidation processes in men with type 1 diabetes mellitus following α-lipoic acid treatment[J]. AIMS Medical Science, 2021, 8(4): 291-300. doi: 10.3934/medsci.2021024







 DownLoad:
DownLoad: