Assuming the care of a dependent family member can constitute a health risk factor that significantly reduces the productivity of family caregivers, compromising their future and quality of life.
Our purpose of this study was to investigate the productivity activities that are altered in the caregivers of a dependent family member and the impact this has on their satisfaction and quality of life.
An analytical observational study was conducted for 500 caregivers of dependent family members. Sociodemographic data were collected for caregivers and their dependent family members. Carers' occupational performance and satisfaction were assessed using the Canadian Occupational Performance Measure (COPM), and quality of life was assessed using the World Health Organization - Quality of Life (WHOQOL-Bref). Comparison between groups was performed using the Chi-square test for qualitative variables. Pearson's correlation coefficient was used to assess the strength and direction of linear associations between numerical variables.
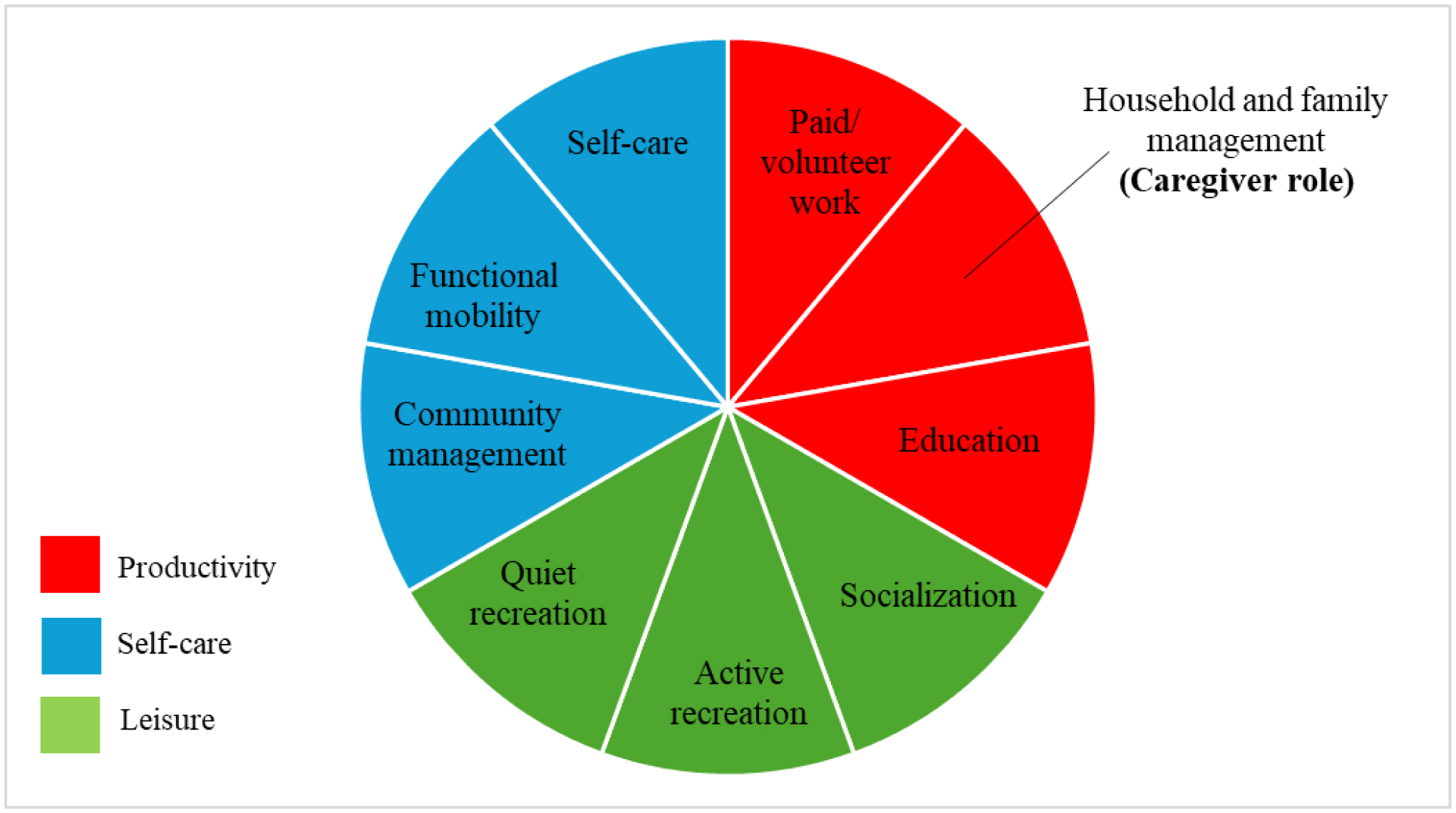
Most caregivers were women (72.3%, n = 364), with an average age of 60.3 ± 13.64 years. These individuals were providing care for a family member with severe dependency (69.7%, n = 348), classified as Grade III. Up to 38.2% (n = 191) of caregivers struggled with maintaining punctuality and consistency in their paid employment, and 25.6% (n = 128) of caregivers stopped or had difficulty working. In addition, 28.4% (n = 142) of caregivers had problems with household cleaning and tidying, 20.4% (n = 102) perceived that they neglected their other family members, and 18.6% (n = 93) of caregivers encountered problems attending courses and furthering their education. Women were more affected in terms of productivity. Moreover, performance and quality of life worsened as the number of productivity activities affected increased.
Caring for a dependent family member has a considerable impact on the caregiver's productive activities, affecting their work performance, household management, and professional development, with a particularly marked impact on women. This caregiving role is also associated with a decrease in quality of life, which highlights the need for interventions to support caregivers in these areas.
Citation: Laura Gonzalo-Ciria, Marta Pérez De Heredia-Torres, María Isabel Vidal-Sánchez, María José López-de-la-Fuente, Elisa Bullón-Benito, Ana Poveda-García, Mariana Ortiz-Piña, María Cristina Ruiz-Garrós, Ana Gascón-Catalán. Loss of productivity among caregivers of dependent family members[J]. AIMS Public Health, 2025, 12(2): 451-469. doi: 10.3934/publichealth.2025025
Assuming the care of a dependent family member can constitute a health risk factor that significantly reduces the productivity of family caregivers, compromising their future and quality of life.
Our purpose of this study was to investigate the productivity activities that are altered in the caregivers of a dependent family member and the impact this has on their satisfaction and quality of life.
An analytical observational study was conducted for 500 caregivers of dependent family members. Sociodemographic data were collected for caregivers and their dependent family members. Carers' occupational performance and satisfaction were assessed using the Canadian Occupational Performance Measure (COPM), and quality of life was assessed using the World Health Organization - Quality of Life (WHOQOL-Bref). Comparison between groups was performed using the Chi-square test for qualitative variables. Pearson's correlation coefficient was used to assess the strength and direction of linear associations between numerical variables.
Most caregivers were women (72.3%, n = 364), with an average age of 60.3 ± 13.64 years. These individuals were providing care for a family member with severe dependency (69.7%, n = 348), classified as Grade III. Up to 38.2% (n = 191) of caregivers struggled with maintaining punctuality and consistency in their paid employment, and 25.6% (n = 128) of caregivers stopped or had difficulty working. In addition, 28.4% (n = 142) of caregivers had problems with household cleaning and tidying, 20.4% (n = 102) perceived that they neglected their other family members, and 18.6% (n = 93) of caregivers encountered problems attending courses and furthering their education. Women were more affected in terms of productivity. Moreover, performance and quality of life worsened as the number of productivity activities affected increased.
Caring for a dependent family member has a considerable impact on the caregiver's productive activities, affecting their work performance, household management, and professional development, with a particularly marked impact on women. This caregiving role is also associated with a decrease in quality of life, which highlights the need for interventions to support caregivers in these areas.

| [1] |
Tejero-Aranguren J, García Del Moral R, Poyatos-Aguilera ME, et al. (2024) Family burden after critical illness: the forgotten caregivers. Med Intensiva (Engl Ed) 48: 69-76. https://doi.org/10.1016/j.medine.2023.08.002 
|
| [2] |
Sánchez Bárcenas RA, López Hernández D, Brito-Aranda L, et al. (2024) Factors associated with caregiver burden in primary caregivers of older adults with type2 diabetes. Aten Primaria 56: 102948. https://doi.org/10.1016/j.aprim.2024.102948
|
| [3] | OECDEvolving Family Models in Spain: A New National Framework for Improved Support and Protection for Families (2022).OECD Publishing. https://doi.org/10.1787/c27e63ab-en |
| [4] |
Boop C, Cahill SM, Davis C, et al. (2020) Occupational therapy practice framework: Domain and process fourth edition. Am J Occup Ther 74: 7412410010p1-7412410010p87. https://doi.org/10.5014/ajot.2020.74S2001
|
| [5] |
Saletti-Cuesta L, Tutton E, Langstaff D, et al. (2018) Understanding informal carers' experiences of caring for older people with a hip fracture: a systematic review of qualitative studies. Disabil Rehabil 40: 740-750. https://doi.org/10.1080/09638288.2016.1262467
|
| [6] | Roca Roger M, Úbeda Bonet I, García Viñets L, et al. (2012) Padres que cuidan a sus hijos con plurisdiscapacidad: estudio cualitativo sobre el cuidado y sus consecuencias. Siglo Cero: Revista Española sobre Discapacidad Intelectual 43: 49-61. https://dialnet.unirioja.es/servlet/extart?codigo=4128594 |
| [7] | Agulló Cantos JM, Paredes-Carbonell JJ, García-Alandete J (2019) Roles e intereses en familiares cuidadores de personas diagnosticadas con enfermedad de Alzheimer. Revista TOG 16: 9-19. |
| [8] |
Castellanos L (2022) La carga del cuidado: repercusiones en la salud de las cuidadoras de personas con discapacidad. MUSAS. Revista de Investigación en Mujer, Salud y Sociedad 7: 26-43. https://doi.org/10.1344/musas2022.vol7.num2.2
|
| [9] |
Fernández-Ávalos MI, Pérez-Marfil MN, Ferrer-Cascales R, et al. (2020) Quality of Life and Concerns in Parent Caregivers of Adult Children Diagnosed with Intellectual Disability: A Qualitative Study. Int J Environ Res Public Health 17: 8690. https://doi.org/10.3390/ijerph17228690
|
| [10] | Swartz K, Collins LG (2019) Caregiver Care. Am Fam Physician 99: 699-706. |
| [11] |
Hazzan AA, Follansbee P, Dauenhauer J, et al. (2020) Relationship between family caregiver quality of life and the care provided to people living with dementia: protocol for a mixed methods study. AIMS Public Health 7: 301-305. https://doi.org/10.3934/publichealth.2020025
|
| [12] |
Stragapede E, Petricone-Westwood D, Hales S, et al. (2023) Patient quality of life and caregiver experiences in ovarian cancer: How are they related?. Qual Life Res 32: 3521-3529. https://doi.org/10.1007/s11136-023-03481-3
|
| [13] |
Young K, Cashion C, Ekberg S, et al. (2023) Quality of life and family functioning soon after paediatric brain tumour diagnosis: A cross-sectional observational study. Eur J Oncol Nurs 67: 102463. https://doi.org/10.1016/j.ejon.2023.102463
|
| [14] |
Ortiz-Mallasén V, Claramonte-Gual E, Cervera-Gasch Á, et al. (2021) Evaluation of the effectiveness of an intervention program in family caregivers of dependent persons, in the primary health care system. Aten Primaria 53: 60-66. https://doi.org/10.1016/j.aprim.2020.06.011
|
| [15] |
Stathopoulou A, Fragkiadakis GF (2023) Assessment of psychological distress and quality of life of family caregivers caring for patients with chronic diseases at home. AIMS Public Health 10: 456-468. https://doi.org/10.3934/publichealth.2023032
|
| [16] |
Bagatell N, Lamarche E, Klinger L (2023) Roles of Caregivers of Autistic Adults: A Qualitative Study. Am J Occup Ther 77: 7702205030. https://doi.org/10.5014/ajot.2023.050117
|
| [17] |
Castilblanco AC (2023) Las políticas de cuidado en algunos países de América Latina. Una mirada feminista. Ánfora 30: 136-160. https://doi.org/10.30854/anf.v30.n54.2023.856
|
| [18] |
Letrondo PA, Ashley SA, Flinn A, et al. (2023) Systematic review of arts and culture-based interventions for people living with dementia and their caregivers. Ageing Res Rev 83: 101793. https://doi.org/10.1016/j.arr.2022.101793
|
| [19] |
Santana E, Mendes F, Bernardo J, et al. (2023) Difficulties in Caring for the Older Adults: Perspective of Brazilian and Portuguese Caregivers. Nurs Rep 13: 284-296. https://doi.org/10.3390/nursrep13010027
|
| [20] | Gómez ÁM, Navarro JR (2019) Tendencias demográficas a escala mundial y sus repercusiones en la provisión de cuidado a las personas mayores dependientes. Actas de coordinación sociosanitaria 25: 31-58. |
| [21] |
Davy G, Barbaro J, Unwin K, et al. (2024) Leisure, community, workforce participation and quality of life in primary and secondary caregivers of autistic children. Autism Res 17: 799-811. https://doi.org/10.1002/aur.3113
|
| [22] |
Huang Y, Hu J, Xie T, et al. (2023) Effects of home-based chronic wound care training for patients and caregivers: A systematic review. Int Wound J 20: 3802-3820. https://doi.org/10.1111/iwj.14219
|
| [23] |
Guato-Torres P, Mendoza-Parra S (2022) Autocuidado del cuidador informal de personas mayores en algunos países de Latinoamérica: Revisión descriptiva. Enfermería: Cuidados Humanizados 11: e2917. https://doi.org/10.22235/ech.v11i2.2917
|
| [24] | McColl MA, Law MC, Debra S (2015) Theoretical Basis of Occupational Therapy (3rd ed.). Routledge: . https://doi.org/10.4324/9781003526742 |
| [25] | Curtin M, Egan M, Adams J (2016) Occupational Therapy for People Experiencing Illness, Injury or Impairment E-Book (previously entitled Occupational Therapy and Physical Dysfunction): Occupational Therapy for People Experiencing Illness, Injury or Impairment E-Book (previously entitled Occupational Therapy and Physical Dysfunction). Elsevier Health Sciences 186. |
| [26] |
Keita Fakeye MB, Samuel LJ, Drabo EF, et al. (2023) Caregiving-Related Work Productivity Loss Among Employed Family and Other Unpaid Caregivers of Older Adults. Value Health 26: 712-720. https://doi.org/10.1016/j.jval.2022.06.014
|
| [27] | Ganapathy V, Graham GD, DiBonaventura MD, et al. (2015) Caregiver burden, productivity loss, and indirect costs associated with caring for patients with poststroke spasticity. Clin Interv Aging 10: 1793-1802. https://doi.org/10.2147/CIA.S91123 |
| [28] |
Sruamsiri R, Mori Y, Mahlich J (2018) Productivity loss of caregivers of schizophrenia patients: a cross-sectional survey in Japan. J Ment Health 27: 583-587. https://doi.org/10.1080/09638237.2018.1466048
|
| [29] | (2008) Aragon GovernmentSistema Aragonés de Atención a la Dependencia: guía informativa [Internet]. Zaragoza: Gobierno de Aragón. Departamento de Servicios Sociales y Familia, Dirección General de Atención a la Dependencia. [cited 2024 November 23]. Available from: https://www.aragon.es/-/dependencia.-informacion-general#:~:text=La%20clasificaci%C3%B3n%20de%20la%20situaci%C3%B3n%20de%20dependencia%3A%20grados,de%20la%20vida%20diaria%2C%20una%20vez%20al%20d%C3%ADa. |
| [30] | Capdevila E, Portell M, Penelo E, et al. (2024) Propiedades de medición del COPM español en pacientes hospitalizados en rehabilitación de adultos mayores. Revista escandinava de terapia ocupacional 31: 2377175. https://doi.org/10.1080/11038128.2024.2377175 |
| [31] |
Gatta FD, Fabrizi E, Giubilei F, et al. (2022) Caregivers' Profiles Based on the Canadian Occupational Performance Measure for the Adoption of Assistive Technologies. Sensors (Basel) 22: 7500. https://doi.org/10.3390/s22197500
|
| [32] |
Mulcahey MJ, Gerhardt N, Alpajora B, et al. (2022) Coaching-in-Context With Informal Maternal Care Partners of Children With Spinal Cord Injury. Top Spinal Cord Inj Rehabil 28: 99-113. https://doi.org/10.46292/sci21-00045
|
| [33] |
Verkerk GJ, Wolf MJ, Louwers AM, et al. (2006) The reproducibility and validity of the Canadian Occupational Performance Measure in parents of children with disabilities. Clin Rehabil 20: 980-988. https://doi.org/10.1177/0269215506070703
|
| [34] |
de Wit J, Schröder CD, El Mecky J, et al. (2019) Support needs of caregivers of patients with amyotrophic lateral sclerosis: A qualitative study. Palliat Support Care 17: 195-201. https://doi.org/10.1017/S1478951517001213
|
| [35] |
Lucas-Carrasco R (2012) The WHO quality of life (WHOQOL) questionnaire: Spanish development and validation studies. Qual Life Res 21: 161-165. https://doi.org/10.1007/s11136-011-9926-3
|
| [36] |
Benitez-Borrego S, Guàrdia-Olmos J, Urzúa-Morales A (2014) Factorial structural analysis of the Spanish version of WHOQOL-BREF: an exploratory structural equation model study. Qual Life Res 23: 2205-2212. https://doi.org/10.1007/s11136-014-0663-2
|
| [37] |
Shefeek SK, Joy TM, Olickal JJ, et al. (2024) Caregiver burden and quality of life in palliative care: cross-sectional study. BMJ Support Palliat Care 12: spcare–2024–005220. https://doi.org/10.1136/spcare-2024-005220
|
| [38] |
Salinas-Rodríguez A, Manrique-Espinoza BS, Montañez-Hernández JC (2022) Mediator effect of caregiver burden on the association between disability and quality of life among older adults. Salud Publica Mex 64: 507-514. https://doi.org/10.21149/13491
|
| [39] | World Health OrganizationWHOQOL: Measuring quality of life (2012). Available from: https://www.who.int/tools/whoqol |
| [40] |
Zarzycki M, Vilchinsky N, Bei E, et al. (2024) Cross-country variations in the caregiver role: evidence from the ENTWINE-iCohort study. BMC Public Health 24: 898. https://doi.org/10.1186/s12889-024-18302-6
|
| [41] |
Martsolf GR, Kandrack R, Rodakowski J, et al. (2020) Work Performance Among Informal Caregivers: A Review of the Literature. J Aging Health 32: 1017-1028. https://doi.org/10.1177/0898264319895374
|
| [42] | Kielhofner G (2002) A model of human occupation: Theory and application. Lippincott Williams & Wilkins. |
| [43] |
Bernabéu-Álvarez C, Lima-Rodríguez JS, Lima-Serrano M (2022) Effect of support groups on caregiver's quality of life. Fam Process 61: 643-658. https://doi.org/10.1111/famp.12684
|
| [44] |
García NAH, Campos AO, Bolaņos C, et al. (2018) Occupational Performance and Satisfaction of the Informal Primary Caregivers of Patients with Activity Limitations. RICS Revista Iberoamericana de las Ciencias de la Salud 7: 1-32.
|
| [45] |
Picatoste X, Mesquita A, González-Laxe F (2023) Gender wage gap, quality of earnings and gender digital divide in the European context. Empirica (Dordr) 50: 301-321. https://doi.org/10.1007/s10663-022-09555-8
|
| [46] |
Rubinich G, Lopes Campos B, Souza Ramos LC, et al. (2021) ¿Promoviendo la igualdad de género? Los avances del G20 y el Women20 para erradicar la brecha economica. Revista SAAP 15: 160-182. https://dx.doi.org/10.46468/rsaap.15.1.n1
|
| [47] |
Ozawa S, Monma T, Tsuchida M, et al. (2024) Health Problems Related to Presenteeism Among Japanese Employees. J Occup Environ Med 66: e1-e7. https://doi.org/10.1097/JOM.0000000000002985
|
| [48] | World Health OrganizationRegional Office for Europe (1986) Ottawa Charter for Health Promotion, 1986. Available from: https://iris.who.int/handle/10665/349652 |
| [49] | Wilcock A, Hocking C An occupational perspective of health, Routledge (2024). |
| [50] |
Lee K, Yefimova M, Puga F, et al. (2021) Gender Differences in Caregiver Burden Among Family Caregivers of Persons With Dementia. J Gerontol Nurs 47: 33-42. https://doi.org/10.3928/00989134-20210610-03
|
| [51] |
Leyva-López A, Rivera-Rivera L, Márquez-Caraveo ME, et al. (2022) Estudio de la calidad de vida en cuidadores familiares de personas con discapacidad intelectual. Salud Publica Mex 64: 397-405. https://doi.org/10.21149/13325
|
| [52] |
Hazzan AA, Dauenhauer J, Follansbee P, et al. (2022) Family caregiver quality of life and the care provided to older people living with dementia: qualitative analyses of caregiver interviews. BMC Geriatr 22: 86. https://doi.org/10.1186/s12877-022-02787-0
|
| [53] |
Farré M, Kostov B, Haro JM, et al. (2018) Costs and Burden Associated With Loss of Labor Productivity in Informal Caregivers of People With Dementia: Results From Spain. J Occup Environ Med 60: 449-456. https://doi.org/10.1097/JOM.0000000000001229
|
| [54] |
Jacobs JC, Van Houtven CH, Tanielian T, et al. (2019) Economic Spillover Effects of Intensive Unpaid Caregiving. Pharmacoeconomics 37: 553-562. https://doi.org/10.1007/s40273-019-00784-7
|
Figures(1) / Tables(5)

Laura Gonzalo-Ciria, Marta Pérez De Heredia-Torres, María Isabel Vidal-Sánchez, María José López-de-la-Fuente, Elisa Bullón-Benito, Ana Poveda-García, Mariana Ortiz-Piña, María Cristina Ruiz-Garrós, Ana Gascón-Catalán. Loss of productivity among caregivers of dependent family members[J]. AIMS Public Health, 2025, 12(2): 451-469. doi: 10.3934/publichealth.2025025







 DownLoad:
DownLoad: