Substance use among adolescents is a public health problem, and the simultaneous use of multiple substances aggravates this problem. Although the facilitators of specific substance use in adolescents have been widely investigated, polydrug use is a less common topic. Likewise, the role that the origin of the information available to adolescents regarding substance use plays in relation to polydrug use is practically unexplored.
This work analyzed the relevance of the origin of the information sources available to adolescents regarding substance use, among which we distinguished those that were monitored (or supervised) by public agencies from those that were unmonitored (or unsupervised) in the consumption of more than one substance. As control variables, we considered three individual factors and four environmental factors. The relevance of these sources was analysed from a dual perspective: on the one hand, their statistical relevance was measured, and on the other hand, how they combined with the control variables was analysed to identify risk and risk-free profiles in substance poly-drug use.
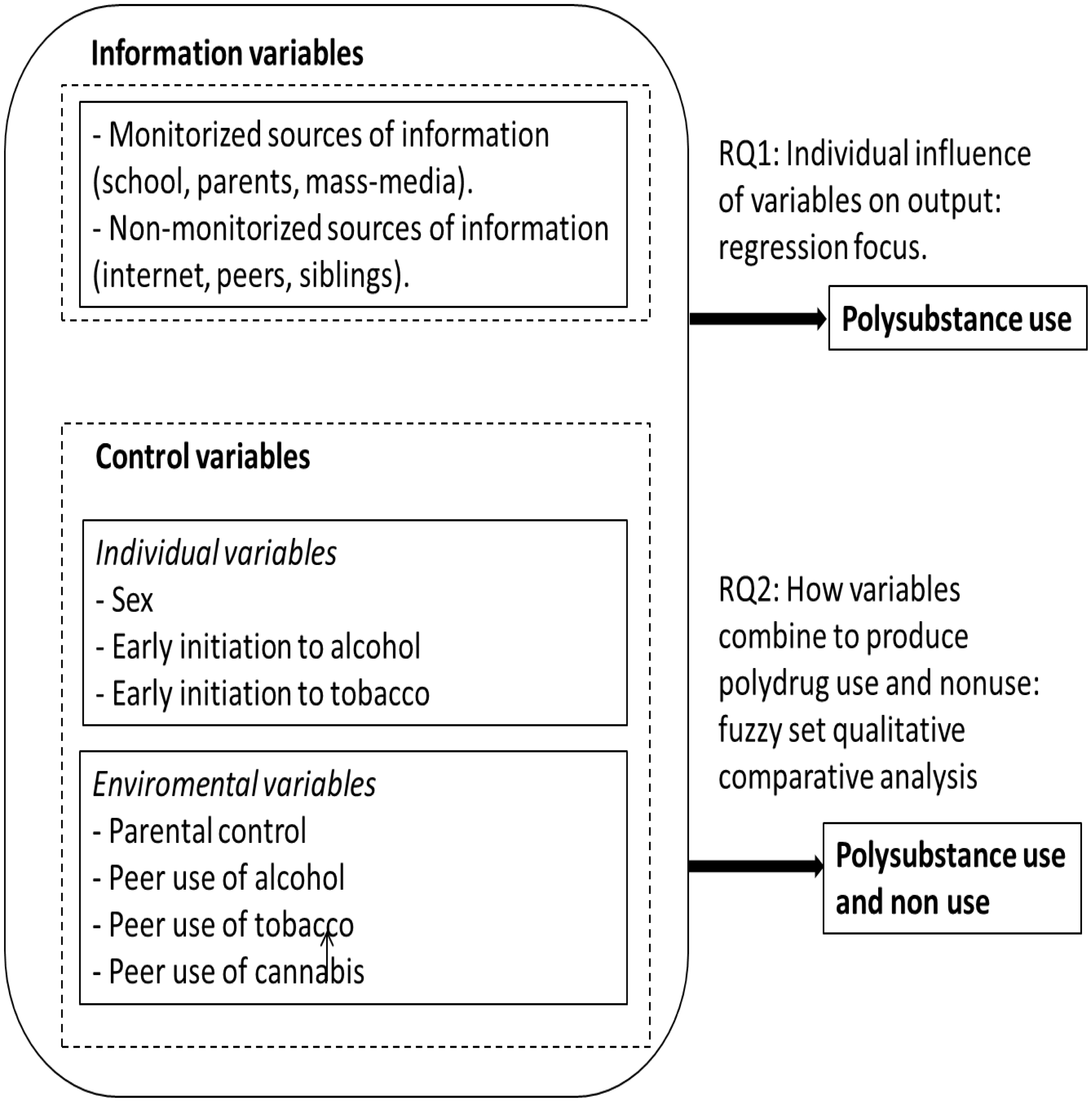
This paper utilized a sample of N = 573 adolescents aged ≥17 years. This sample was collected from a survey administered in the spring of 2023. We examined the impact of unmonitored information sources (peers, siblings, and the Internet) and supervised sources (school, parents, and media) on the combined consumption of alcohol, tobacco, and cannabis. Additionally, we took three individual factors (gender, early onset of alcohol, and tobacco use) and four environmental factors (parental control, alcohol, tobacco, and cannabis use among peers) into account as control variables. Initially, we conducted a regression analysis to adjust for the impact of these factors on polydrug use. Subsequently, we employed a fuzzy set qualitative analysis (fsQCA) to investigate how predictor factors combined with the formation of adolescent profiles associated with polydrug consumption and nonconsumption.
Unmonitored information sources were associated with a greater incidence of poly consumption, with ORs of 1.703 and p values of 0.004. However, the protective effects of regulated information sources remained ambiguous. Among the variables positively linked with of polydrug use, are female sex (OR = 1.329, p = 0.0076), early alcohol consumption (OR = 4.680, p < 0.0001), and early tobacco consumption (OR = 3.242, p < 0.001) were the most important. Peer drinking (OR = 1.556, p = 0.0187) and peer cannabis use (OR = 1.351, p = 0.0226) were also significantly correlated. The use of the fsQCA made it possible to identify the profiles of adolescents associated to polysubstance use and non-use. The conditions of the configurations that explained use were characterized by an early onset of the joint consumption of tobacco and alcohol. The profile of non-consuming adolescents is that of adolescents whose peers do not use tobacco or cannabis and who have parental control and monitored sources.
Citation: Jorge de Andrés-Sánchez, Francesc Valls-Fonayet, Anna Sánchez-Aragón, Inma Pastor-Gosálbez, Angel Belzunegui-Eraso. Explanatory factors of polydrug use in mid-late teens and the relevance of information sources: Correlational and configurational assessment in Tarragona (Spain)[J]. AIMS Public Health, 2024, 11(3): 773-802. doi: 10.3934/publichealth.2024039
Substance use among adolescents is a public health problem, and the simultaneous use of multiple substances aggravates this problem. Although the facilitators of specific substance use in adolescents have been widely investigated, polydrug use is a less common topic. Likewise, the role that the origin of the information available to adolescents regarding substance use plays in relation to polydrug use is practically unexplored.
This work analyzed the relevance of the origin of the information sources available to adolescents regarding substance use, among which we distinguished those that were monitored (or supervised) by public agencies from those that were unmonitored (or unsupervised) in the consumption of more than one substance. As control variables, we considered three individual factors and four environmental factors. The relevance of these sources was analysed from a dual perspective: on the one hand, their statistical relevance was measured, and on the other hand, how they combined with the control variables was analysed to identify risk and risk-free profiles in substance poly-drug use.
This paper utilized a sample of N = 573 adolescents aged ≥17 years. This sample was collected from a survey administered in the spring of 2023. We examined the impact of unmonitored information sources (peers, siblings, and the Internet) and supervised sources (school, parents, and media) on the combined consumption of alcohol, tobacco, and cannabis. Additionally, we took three individual factors (gender, early onset of alcohol, and tobacco use) and four environmental factors (parental control, alcohol, tobacco, and cannabis use among peers) into account as control variables. Initially, we conducted a regression analysis to adjust for the impact of these factors on polydrug use. Subsequently, we employed a fuzzy set qualitative analysis (fsQCA) to investigate how predictor factors combined with the formation of adolescent profiles associated with polydrug consumption and nonconsumption.
Unmonitored information sources were associated with a greater incidence of poly consumption, with ORs of 1.703 and p values of 0.004. However, the protective effects of regulated information sources remained ambiguous. Among the variables positively linked with of polydrug use, are female sex (OR = 1.329, p = 0.0076), early alcohol consumption (OR = 4.680, p < 0.0001), and early tobacco consumption (OR = 3.242, p < 0.001) were the most important. Peer drinking (OR = 1.556, p = 0.0187) and peer cannabis use (OR = 1.351, p = 0.0226) were also significantly correlated. The use of the fsQCA made it possible to identify the profiles of adolescents associated to polysubstance use and non-use. The conditions of the configurations that explained use were characterized by an early onset of the joint consumption of tobacco and alcohol. The profile of non-consuming adolescents is that of adolescents whose peers do not use tobacco or cannabis and who have parental control and monitored sources.

| [1] |
Ren M, Lotfipour S (2019) Nicotine gateway effects on adolescent substance use. West J Emerg Med 20: 696-709. https://doi.org/10.5811/westjem.2019.7.41661 
|
| [2] |
Soriano-Sánchez J, Jiménez-Vázquez D (2022) Predictores del consumo de alcohol en adolescentes: una revisión sistemática de estudios transversales. Revista Estudios Psicológicos 2: 73-86. https://doi.org/10.35622/j.rep.2022.04.006
|
| [3] | Spanish Observatory on Drugs and Addictions (OEDA)Survey on drug use in secondary education in Spain (ESTUDES), 1994–2021 (2022). Available from: https://pnsd.sanidad.gob.es/profesionales/sistemasInformacion/sistemaInformacion/pdf/ESTUDES_2021_Informe_de_Resultados.pdf |
| [4] | Codinach-Danés E, Obradors-Rial N, González-Casals H, et al. (2022) Polydrug use of tobacco and cannabis: Relationship with self-perceived health and mood state in adolescents in Central Catalonia-DESKcohort Project. Adicciones 36: 1716-1716. https://doi.org/10.20882/adicciones.1716 |
| [5] |
Gray KM, Squeglia LM (2018) Research review: What have we learned about adolescent substance use?. J Child Psychol Psychiatry 59: 618-627. https://doi.org/10.1111/jcpp.12783
|
| [6] | Clemans-Cope L, Lynch V, Winiski E, et al. Substance use and age of substance use initiation during adolescence: Self-reported patterns by race and ethnicity in the United States, 2015–19 (2021). Available from: https://www.urban.org/sites/default/files/publication/105389/substance-use-and-age-of-substance-use-initiation-during-adolescence_0.pdf |
| [7] |
Jongenelis M, Pettigrew S, Lawrence D, et al. (2019) Factors associated with poly drug use in adolescents. Prev Sci 20: 695-704. https://doi.org/10.1007/s11121-019-00993-8
|
| [8] |
Steinhoff A, Bechtiger L, Ribeaud D, et al. (2022) Polysubstance use in early adulthood: Patterns and developmental precursors in an urban cohort. Front Behav Neurosci 15: 797473. https://doi.org/10.3389/fnbeh.2021.797473
|
| [9] |
Magallon-Neri E, Diaz R, Forns M, et al. (2015) Personality psychopathology, drug use and psychological symptoms in adolescents with substance use disorders and community controls. PeerJ 3: e992. https://doi.org/10.7717/peerj.992
|
| [10] |
Hamidullah S, Thorpe HH, Frie JA, et al. (2020) Adolescent substance use and the brain: Behavioral, cognitive and neuroimaging correlates. Front Hum Neurosci 14: 298. https://doi.org/10.3389/fnhum.2020.00298
|
| [11] |
García-Pérez Á, Alonso-Diego G, Weidberg S, et al. (2023) Testing the cannabis gateway hypothesis in a national sample of Spanish adolescents. Addict Behav 144: 107751. https://doi.org/10.1016/j.addbeh.2023.107751
|
| [12] |
Codinach-Danés E, Obradors-Rial N, González-Casals H, et al. (2022) Polydrug use of tobacco and cannabis in a cohort of young people from central Catalonia (2012–2020). Adolescents 2: 350-357. https://doi.org/10.3390/adolescents2030027
|
| [13] |
Francis JM, Myers B, Nkosi S, et al. (2019) The prevalence of religiosity and association between religiosity and alcohol use, other drug use, and risky sexual behaviours among grade 8–10 learners in Western Cape, South Africa. PloS One 14: e0211322. https://doi.org/10.1371/journal.pone.0211322
|
| [14] |
Lawn W, Mokrysz C, Petrilli K, et al. (2020) Teenagers, compared to adults, are more vulnerable to the psychotic-like and addiction-forming risks associated with chronic cannabis use. Biol Psychiat 87: S227. http://doi.org/10.1016/j.biopsych.2020.02.589
|
| [15] |
Brière FN, Fallu JS, Descheneaux A, et al. (2011) Predictors and consequences of simultaneous alcohol and cannabis use in adolescents. Addict Behav 36: 785-788. https://doi.org/10.1016/j.addbeh.2011.02.012
|
| [16] |
Sutherland I, Shepherd JP (2001) Social dimensions of adolescent substance use. Addict 96: 445-458. http://dx.doi.org/10.1046/j.1360-0443.2001.9634458.x
|
| [17] |
Trucco EM (2020) A review of psychosocial factors linked to adolescent substance use. Pharmacol Biochem Behav 196: 172969. https://doi.org/10.1016/j.pbb.2020.172969
|
| [18] |
Nawi AM, Ismail R, Ibrahim F, et al. (2021) Risk and protective factors of drug abuse among adolescents: a systematic review. BMC Public Health 21: 2088. https://doi.org/10.1186/s12889-021-11906-2
|
| [19] |
Jayasinghe UW, Harris MF, Parker SM, et al. (2016) The impact of health literacy and life style risk factors on health-related quality of life of Australian patients. Health Qual Life Outcomes 14: 68. https://doi.org/10.1186/s12955-016-0471-1
|
| [20] |
Bröder J, Okan O, Bauer U, et al. (2017) Health literacy in childhood and youth: A systematic review of definitions and models. BMC Public Health 17: 361. https://doi.org/10.1186/s12889-017-4267-y
|
| [21] |
Belzunegui-Eraso A, Pastor-Gosálbez I, Raigal-Aran L, et al. (2020) Substance use among Spanish adolescents: The information paradox. Int J Environ Res Public Health 17: 627. https://doi.org/10.3390/ijerph17020627
|
| [22] |
Fleary SA, Joseph P, Pappagianopoulos JE (2018) Adolescent health literacy and health behaviors: A systematic review. J Adolesc 62: 116-127. https://doi.org/10.1016/j.adolescence.2017.11.010
|
| [23] |
Sadeghi R, Saeed S, Mahmoodabad M, et al. (2019) The association between health literacy and smoking (Hookah and Cigarette) among the young men in Sirjan, Iran. J Subst Use 24: 546-549. https://doi.org/10.1080/14659891.2019.1620886
|
| [24] |
Rolova G, Gavurova B, Petruzelka B (2021) Health literacy, self-perceived health, and substance use behavior among young people with alcohol and substance use disorders. Int J Environ Res Public Health 18: 4337. https://doi.org/10.3390/ijerph18084337
|
| [25] |
Mélard N, Grard A, Robert PO, et al. (2020) School tobacco policies and adolescent smoking in six European cities in 2013 and 2016: A school-level longitudinal study. Prev Med 138: 106142. https://doi.org/10.1016/j.ypmed.2020.106142
|
| [26] |
Dermota P, Wang J, Dey M, et al. (2013) Health literacy and substance use in young Swiss men. Int J Public Health 58: 939-948. https://doi.org/10.1007/s00038-013-0487-9
|
| [27] |
Chen X, Hay JL, Waters EA, et al. (2018) Health literacy and use and trust in health information. J Health Commun 23: 724-734. https://doi.org/10.1080/10810730.2018.1511658
|
| [28] |
Buawangpong N, Sirikul W, Anukhro C, et al. (2022) Health information sources influencing health literacy in different social contexts across age groups in northern Thailand citizens. Int J Environ Res Public Healt 19: 6051. https://doi.org/10.3390/ijerph19106051
|
| [29] |
Manganello JA (2008) Health literacy and adolescents: A framework and agenda for future research. Health Educ Res 23: 840-847. https://doi.org/10.1093/her/cym069
|
| [30] |
Bujnowska-Fedak MM (2015) Trends in the use of the internet for health purposes in Poland. BMC Public Health 15: 194. https://doi.org/10.1186/s12889-015-1473-3
|
| [31] |
Alduraywish SA, Altamimi LA, Aldhuwayhi RA, et al. (2020) Sources of health information and their impacts on medical knowledge perception among the Saudi Arabian population: Cross-sectional study. J Med Internet Res 22: e14414. https://doi.org/10.2196/14414
|
| [32] | Diz JI (2013) Desarrollo del adolescente: Aspectos físicos, psicológicos y sociales. Pediatr Integral 17: 88-93. |
| [33] |
Salmela-Aro K (2011) Stages of adolescence. En Encyclopedia of Adolescence . USA: Elsevier 360-368. https://doi.org/10.1016/B978-0-12-373951-3.00043-0
|
| [34] |
Luk TT, Wang MP, Leung LT, et al. (2018) Perceived family relationship quality and use of poly-tobacco products during early and late adolescence. Addictive Behaviors 85: 38-42. https://doi.org/10.1016/j.addbeh.2018.05.011
|
| [35] |
Tur-Porcar AM, Jiménez-Martínez J, Mestre-Escrivá V (2019) Substance use in early and middle adolescence. The role of academic efficacy and parenting. Psychosoc Interv 28: 139-145. https://doi.org/10.5093/pi2019a11
|
| [36] |
Estoup AC, Moise-Campbell C, Varma M, et al. (2016) The impact of marijuana legalization on adolescent use, consequences, and perceived risk. Subst Use Misuse 51: 1881-1887. https://doi.org/10.1080/10826084.2016.1200623
|
| [37] |
Zimmerman GM, Farrell C (2017) Parents, peers, perceived risk of harm, and the neighborhood: Contextualizing key influences on adolescent substance use. J Youth Adolesc 46: 228-247. https://doi.org/10.1007/s10964-016-0475-5
|
| [38] | Generalitat de CatalunyaPrevention of drug use (2023). Available from: https://drogues.gencat.cat/ca/professionals/prevencio/programes_i_recursos/ambit_educatiu/programes_i_materials_deducacio_formal/#programes |
| [39] | Odériz-Echevarria7 motivos para perder la custodia de un hijo (2023). Available from: https://oderizabogados.es/motivos-perder-custodia-hijo/ |
| [40] | Federation of Associations of Journalists of SpainCode of ethics (2017). Available from: https://fape.es/home/codigo-deontologico/ |
| [41] |
Eisenberg ME, Toumbourou JW, Catalano RF, et al. (2014) Social norms in the development of adolescent substance use: A longitudinal analysis of the International Youth Development Study. J Youth Adolesc 43: 1486-1497. https://doi.org/10.1007/s10964-014-0111-1
|
| [42] |
Montgomery SC, Donnelly M, Bhatnagar P, et al. (2020) Peer social network processes and adolescent health behaviors: A systematic review. Prev Med 130: 105900. https://doi.org/10.1016/j.ypmed.2019.105900
|
| [43] |
Gupte HA, D'Costa M, Chaudhuri L (2020) Why do Adolescents initiate and continue using tobacco and areca nut?: A qualitative study tracing pathways of use among school-going adolescents in Mumbai, India. Nicotine Tob Res 22: 2022-2031. https://doi.org/10.1093/ntr/ntaa015
|
| [44] | Musitu G (2014) Why do teenagers have a low perception of risks regarding alcohol consumption? The experts' perspective.Metamorfosis. Revista del Centro Reina Sofía sobre Adolescencia y Juventud 1: 55-73. Available from: https://dialnet.unirioja.es/servlet/articulo?codigo=6163202 |
| [45] | Parissi-Poumian Y, de San Jorge-Cárdenas X, López-Ornelas M, et al. (2023) Internet search patterns for psychoactive substance use prevention and treatment in Mexico: A cross-sectional study. J Taibah Univ Med Sci 18: 246-256. https://doi.org/10.1016/j.jtumed.2022.09.009 |
| [46] |
Tomazic T, Jerkovic OS (2020) Online interventions for the selective prevention of illicit drug use in young drug users: Exploratory study. J Med Internet Res 22: e17688. https://doi.org/10.2196/17688
|
| [47] |
Evans W, Andrade E, Pratt M, et al. (2020) Peer-to-peer social media as an effective prevention strategy: Quasi-experimental evaluation. JMIR mHealth and uHealth 8: e16207. https://doi.org/10.2196/16207
|
| [48] |
Ahmad J, Joel UC, Talabi FO, et al. (2022) Impact of social media-based intervention in reducing youths' propensity to engage in drug abuse in Nigeria. Eval Program Plann 94: 102122. https://doi.org/10.1016/j.evalprogplan.2022.102122
|
| [49] |
Suarez-Lledo V, Alvarez-Galvez J (2021) Prevalence of health misinformation on social media: systematic review. J Med Internet Res 23: e17187. https://doi.org/10.2196/17187
|
| [50] | National Institute on Drug AbuseSex and differences in substance use (2020). Available from: https://nida.nih.gov/publications/research-reports/substance-use-in-women/sex-gender-differences-in-substance-use |
| [51] |
McHugh RK, Votaw VR, Sugarman DE, et al. (2018) Sex and gender differences in substance use disorders. Clin Psychol Rev 66: 12-23. https://doi.org/10.1016/j.cpr.2017.10.012
|
| [52] |
Trujillo CA, Obando D, Trujillo A (2019) An examination of the association between early initiation of substance use and interrelated multilevel risk and protective factors among adolescents. PLoS One 14: e0225384. https://doi.org/10.1371/journal.pone.0225384
|
| [53] |
Collins RL, Ellickson PL, Bell RM (1998) Simultaneous polydrug use among teens: prevalence and predictors. J Subst Abuse 10: 233-253. https://doi.org/10.2478/nsad-2014-0026
|
| [54] |
Ontaneda Aguilar MP, Ruisoto Palomera P, López Núñez C, et al. (2022) The role of age of onset in problematic alcohol consumption: Artefact or cohort effect?. Clínica y Salud 33: 11-17. https://doi.org/10.5093/clysa2021a11
|
| [55] |
DeWit DJ, Adlaf EM, Offord DR, et al. (2000) Age at first alcohol use: a risk factor for the development of alcohol disorders. Am J Psychiatry 157: 745-750. https://doi.org/10.1176/appi.ajp.157.5.745
|
| [56] |
Cosco TD, Morgan K, Currie L, et al. (2013) Early-onset drinking in Ireland: negative outcomes and behaviours. Public Health 127: 788-790. https://doi.org/10.1016/j.puhe.2013.03.004
|
| [57] |
Aiken A, Clare PJ, Wadolowski M, et al. (2018) Age of alcohol initiation and progression to binge drinking in adolescence: A prospective cohort study. A Alcohol Clin Exp Res 42: 100-110. https://doi.org/10.1111/acer.13525
|
| [58] |
Dai Z, Wang K (2023) The association between early onset of alcohol, smokeless tobacco and marijuana use with adult binge drinking in United States. Sci Rep 13: 187. https://doi.org/10.1038/s41598-023-27571-x
|
| [59] | Chassin L, Curran PJ, Presson CC, et al. (2009) Developmental trajectories of cigarette smoking from adolescence to adulthood. Phenotypes and endophenotypes: Foundations for genetic studies of nicotine use and dependence (Tobacco Control Monograph No. 20). US Department of Health and Human Services, NIH, National Cancer Institute: NIH Publication, (09–6366), 189–244 . Available from: https://cancercontrol.cancer.gov/sites/default/files/2020-06/m20_5.pdf |
| [60] |
Kendler KS, Myers J, Damaj MI, et al. (2013) Early smoking onset and risk for subsequent nicotine dependence: A monozygotic co-twin control study. Am J Psychiatry 170: 408-413. https://doi.org/10.1176/appi.ajp.2012.12030321
|
| [61] |
Rial A, Golpe S, Barreiro C, et al. (2020) The age of onset for alcohol consumption among adolescents: Implications and related variables. Adicciones 32: 52-63. http://dx.doi.org/10.20882/adicciones.1266
|
| [62] |
Millar SR, Mongan D, Smyth BP, et al. (2021) Relationships between age at first substance use and persistence of cannabis use and cannabis use disorder. BMC Public Health 21: 997. https://doi.org/10.1186/s12889-021-11023-0
|
| [63] |
Varela MDCM, Becoña E (2015) Do cigarette smoking and alcohol consumption associate with cannabis use and problem gambling among Spanish adolescents?. Adicciones 27: 8-16. http://dx.doi.org/10.20882/adicciones.189
|
| [64] |
Fairman BJ, Furr-Holden CD, Johnson RM (2019) When marijuana is used before cigarettes or alcohol: Demographic predictors and associations with heavy use, cannabis use disorder, and other drug-related outcomes. Prev Sci 20: 225-233. https://doi.org/10.1007/s11121-018-0908-3
|
| [65] |
Voisine S, Parsai M, Marsiglia FF, et al. (2008) Effects of parental monitoring, permissiveness, and injunctive norms on substance use among Mexican and Mexican American adolescents. Fam Soc 89: 264-273. https://doi.org/10.1606/1044-3894.3742
|
| [66] |
Kristjansson ÁL, Sigfusdottir ID, Allegrante JP, et al. (2008) Social correlates of cigarette smoking among Icelandic adolescents: A population-based cross sectional study. BMC Public Health 8: 86. https://doi.org/10.1186/1471-2458-8-86
|
| [67] |
Kristjansson ÁL, Sigfusdottir ID, James JE, et al. (2010) Perceived parental reactions and peer respect as predictors of adolescent cigarette smoking and alcohol use. Addict Behav 35: 256-259. https://doi.org/10.1016/j.addbeh.2009.10.002
|
| [68] |
Ozer EJ, Flores E, Tschann JM, et al. (2013) Parenting style, depressive symptoms, and substance use in Mexican American adolescents. Youth Soc 45: 365-388. https://doi.org/10.1177/0044118X11418539
|
| [69] |
Kim-Spoon J, Farley JP, Holmes C, et al. (2014) Processes linking parents' and adolescents' religiousness and adolescent substance use: Monitoring and self-control. J Youth Adolesc 43: 745-756. https://doi.org/10.1007/s10964-013-9998-1
|
| [70] |
Berge J, Sundell K, Öjehagen A, et al. (2016) Role of parenting styles in adolescent substance use: results from a Swedish longitudinal cohort study. BMJ Open 6: e008979. https://doi.org/10.1136/bmjopen-2015-008979
|
| [71] |
De Looze ME, Van Dorsselaer SAFM, Monshouwer K, et al. (2017) Trends in adolescent alcohol use in the Netherlands, 1992–2015: Differences across sociodemographic groups and links with strict parental rule-setting. Int J Drug Policy 50: 90-101. https://doi.org/10.1016/j.drugpo.2017.09.013
|
| [72] |
Stanley LR, Swaim RC, Dieterich SE (2017) The role of norms in marijuana use among American Indian adolescents. Prev Sci 18: 406-415. https://doi.org/10.1007/s11121-017-0768-2
|
| [73] |
Cruz-Salmerón VH, Martínez-Martínez ML, Garibay-López L, et al. (2011) Comparison of family functioning profiles in adolescents with and without substance addiction in a high school. Atención Primaria 43: 89-94. https://doi.org/10.1016/j.aprim.2010.04.009
|
| [74] | Jiménez-Iglesias A, Moreno C, Rivera F, et al. (2013) The role of the family in promoting responsible substance use in adolescence. Int J Child Youth Fa 22: 585-602. https://doi.org/10.1007/s10826-013-9737-y |
| [75] |
Fuentes M, Alarcón A, García F, et al. (2015) Consumo de alcohol, tabaco, cannabis y otras drogas en la adolescencia: efectos de la familia y peligro del barrio. Anales de psicología 31: 1000-1007. http://dx.doi.org/10.6018/analesps.31.3.183491
|
| [76] |
Henneberger AK, Mushonga DR, Preston AM (2021) Peer influence and adolescent substance use: A systematic review of dynamic social network research. Adolescent Res Rev 6: 57-73. https://doi.org/10.1007/s40894-019-00130-0
|
| [77] |
Burk WJ, Van der Vorst H, Kerr M, et al. (2012) Alcohol intoxication frequency and friendship dynamics: Selection and socialization in early, middle-and late-adolescent peer networks. J Stud Alcohol Drugs 73: 89-98. https://doi.org/10.15288/jsad.2012.73.89
|
| [78] | Planet Youth (2018). Available from: https://planetyouth.org/ |
| [79] |
Pappas IO, Woodside AG (2021) Fuzzy-set Qualitative Comparative Analysis (fsQCA): Guidelines for research practice in information systems and marketing. Int J Inf Ma 58: 102310. https://doi.org/10.1016/j.ijinfomgt.2021.102310
|
| [80] | McFadden D Quantitative methods for analyzing travel behaviour of individuals: Some recent developments (1979). Available from: https://elischolar.library.yale.edu/cowles-discussion-paper-series/707 |
| [81] |
Woodside AG (2014) Embrace perform model: Complexity theory, contrarian case analysis, and multiple realities. J Bu Res 67: 2495-2503. https://doi.org/10.1016/j.jbusres.2014.07.006Get
|
| [82] | Ragin CC (1999) Using qualitative comparative analysis to study causal complexity. Heal Serv Res 34: 1225-1239. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1089061/ |
| [83] |
Pagliarin S, La Mendola S, Vis B (2023) The “qualitative” in Qualitative Comparative Analysis (QCA): Research moves, case-intimacy and face-to-face interviews. Qual Quant 57: 489-507. https://doi.org/10.1007/s11135-022-01358-0
|
| [84] | Rutten R, Rubinson C A vocabulary for QCA (2022). Available from: https://compasss.org/wp-content/uploads/2023/02/vocabulary.pdf |
| [85] |
De Andrés-Sánchez J, Belzunegui-Eraso A (2022) Explaining cannabis use by adolescents: A comparative assessment of fuzzy set qualitative comparative analysis and ordered logistic regression. Healthcare (Basel) 10: 669. https://doi.org/10.3390/healthcare10040669
|
| [86] |
Kumar S, Sahoo S, Lim W M, et al. (2022) Fuzzy-set qualitative comparative analysis (fsQCA) in business and management research: A contemporary overview. Technol Forecast Soc 178: 121599. https://doi.org/10.1016/j.techfore.2022.121599
|
| [87] |
Sharmin S, Kypri K, Khanam M, et al. (2017) Effects of parental alcohol rules on risky drinking and related problems in adolescence: Systematic review and meta-analysis. Drug Alcohol Depend 178: 243-256. https://doi.org/10.1016/j.drugalcdep.2017.05.011
|
| [88] |
Staff J, Vuolo M, Kelly BC, et al. (2022) Electronic cigarette use in adolescence is associated with later cannabis use. Drug Alcohol Depend 232: 109302. http://doi.org/10.1016/j.drugalcdep.2022.109302
|
| [89] |
Mehanović E, Vigna-Taglianti F, Faggiano F, et al. (2022) Does parental permissiveness toward cigarette smoking and alcohol use influence illicit drug use among adolescents? A longitudinal study in seven European countries. Soc Psychiatry Psychiatr Epidemiol 57: 173-181. https://doi.org/10.1007/s00127-021-02118-5
|
| [90] | Lee SSY (2014) Using fuzzy-set qualitative comparative analysis. Epidemiol. Health 36: e2014038. https://doi.org/10.4178/epih/e2014038 |
| [91] |
Zhang S, Wang X, Wang H (2023) Exploring configurations of social determinants for enhancing older adult health in China: An fuzzy-set qualitative comparative analysis based on 31 provinces in China. Front Public Health 11: 1255877. https://doi.org/10.3389/fpubh.2023.1255877
|
| [92] |
De Andrés-Sánchez J (2023) A configurational evaluation of Spanish teleworkers' perception and nonperception of stress during the COVID-19 pandemic. Societies 13: 178. http://dx.doi.org/10.3390/soc13080178
|
 publichealth-11-03-039-s001.pdf publichealth-11-03-039-s001.pdf |
 |

Figures(2) / Tables(7)

Jorge de Andrés-Sánchez, Francesc Valls-Fonayet, Anna Sánchez-Aragón, Inma Pastor-Gosálbez, Angel Belzunegui-Eraso. Explanatory factors of polydrug use in mid-late teens and the relevance of information sources: Correlational and configurational assessment in Tarragona (Spain)[J]. AIMS Public Health, 2024, 11(3): 773-802. doi: 10.3934/publichealth.2024039







 DownLoad:
DownLoad: