Artificial intelligence (AI) is playing an increasing role in several fields of medicine. It is also gaining popularity among surgeons as a valuable screening and diagnostic tool for many conditions such as benign and malignant colorectal, gastric, thyroid, parathyroid, and breast disorders. In the literature, there is no review that groups together the various application domains of AI when it comes to the screening and diagnosis of main surgical diseases. The aim of this review is to describe the use of AI in these settings. We performed a literature review by searching PubMed, Web of Science, Scopus, and Embase for all studies investigating the role of AI in the surgical setting, published between January 01, 2000, and June 30, 2023. Our focus was on randomized controlled trials (RCTs), meta-analysis, systematic reviews, and observational studies, dealing with large cohorts of patients. We then gathered further relevant studies from the reference list of the selected publications. Based on the studies reviewed, it emerges that AI could strongly enhance the screening efficiency, clinical ability, and diagnostic accuracy for several surgical conditions. Some of the future advantages of this technology include implementing, speeding up, and improving the automaticity with which AI recognizes, differentiates, and classifies the various conditions.
Citation: Giuseppe Palomba, Agostino Fernicola, Marcello Della Corte, Marianna Capuano, Giovanni Domenico De Palma, Giovanni Aprea. Artificial intelligence in screening and diagnosis of surgical diseases: A narrative review[J]. AIMS Public Health, 2024, 11(2): 557-576. doi: 10.3934/publichealth.2024028
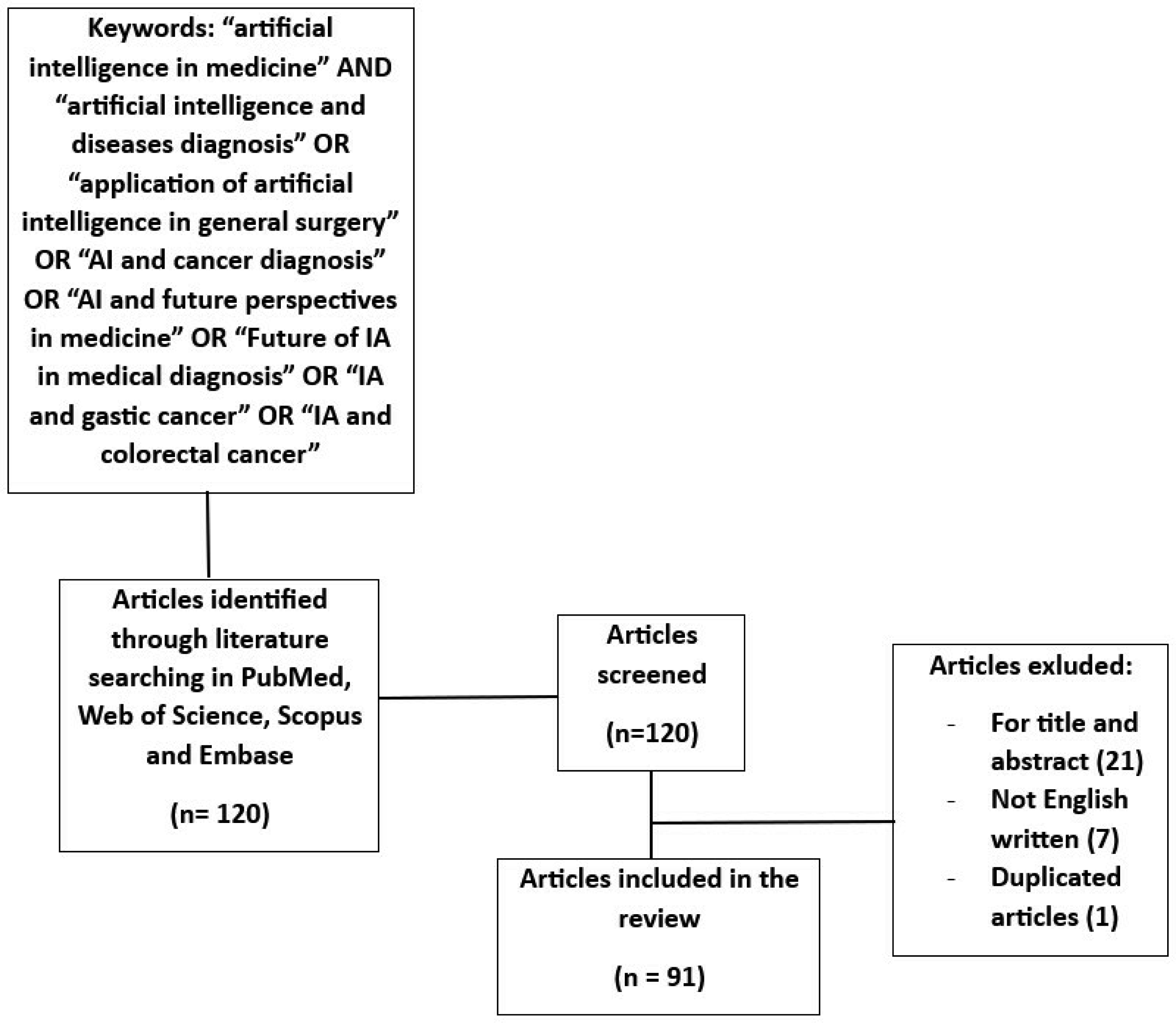
Artificial intelligence (AI) is playing an increasing role in several fields of medicine. It is also gaining popularity among surgeons as a valuable screening and diagnostic tool for many conditions such as benign and malignant colorectal, gastric, thyroid, parathyroid, and breast disorders. In the literature, there is no review that groups together the various application domains of AI when it comes to the screening and diagnosis of main surgical diseases. The aim of this review is to describe the use of AI in these settings. We performed a literature review by searching PubMed, Web of Science, Scopus, and Embase for all studies investigating the role of AI in the surgical setting, published between January 01, 2000, and June 30, 2023. Our focus was on randomized controlled trials (RCTs), meta-analysis, systematic reviews, and observational studies, dealing with large cohorts of patients. We then gathered further relevant studies from the reference list of the selected publications. Based on the studies reviewed, it emerges that AI could strongly enhance the screening efficiency, clinical ability, and diagnostic accuracy for several surgical conditions. Some of the future advantages of this technology include implementing, speeding up, and improving the automaticity with which AI recognizes, differentiates, and classifies the various conditions.

| [1] |
Kaul V, Enslin S, Gross SA (2020) History of artificial intelligence in medicine. Gastrointest Endosc 92: 807-812. https://doi.org/10.1016/j.gie.2020.06.040 
|
| [2] |
Cobianchi L, Piccolo D, Dal Mas F, et al. (2023) Surgeons' perspectives on artificial intelligence to support clinical decision-making in trauma and emergency contexts: Results from an international survey. World J Emerg Surg 18: 1. https://doi.org/10.1186/s13017-022-00467-3. Erratum in:
|
| [3] |
Jackson RS, Schmalbach CE (2017) New frontiers in surgical innovation. Otolaryngol Clin North Am 50: 733-746.
|
| [4] | Szold A (2016) The death of surgery as we know it. Exponential Medicine, Singularity University . Available from: https://exponential.singularityu.org/medicine/amirszold-on-the-death-of-surgery-aswe-know-it/ |
| [5] | Mohr C (2016) Future intervention. Exponential medicine, Singularity University . Available from: https://exponential.singularityu.org/medicine/catherine-mohr-on-thefuture-of-intervention/ |
| [6] |
Hsiao YJ, Wen YC, Lai WY, et al. (2021) Application of artificial intelligence-driven endoscopic screening and diagnosis of gastric cancer. World J Gastroenterol 27: 2979-2993. https://doi.org/10.3748/wjg.v27.i22.2979
|
| [7] |
Chen ZH, Lin L, Wu CF, et al. (2021) Artificial intelligence for assisting cancer diagnosis and treatment in the era of precision medicine. Cancer Commun (Lond) 41: 1100-1115. https://doi.org/10.1002/cac2.12215
|
| [8] |
Loftus TJ, Upchurch GR, Bihorac A (2021) Building an artificial intelligence-competent surgical workforce. JAMA Surg 156: 511. https://doi.org/10.1001/jamasurg.2021.0045
|
| [9] |
Pinsky PF (2015) Principles of Cancer Screening. Surg Clin North Am 95: 953-966. https://doi.org/10.1016/j.suc.2015.05.009
|
| [10] |
López-Labraca J, González-Díaz I, Díaz-de-María F, et al. (2022) An interpretable CNN-based CAD system for skin lesion diagnosis. Artif Intell Med 132: 102370. https://doi.org/10.1016/j.artmed.2022.102370
|
| [11] | Huang Q, Zhang F, Li X (2018) Machine learning in ultrasound computer-aided diagnostic systems: A survey. Biomed Res Int 2018: 5137904. https://doi.org/10.1155/2018/5137904 |
| [12] |
Johnson-Mann CN, Loftus TJ, Bihorac A (2021) Equity and artificial intelligence in surgical care. JAMA Surg 156: 509. https://doi.org/10.1001/jamasurg.2020.7208
|
| [13] |
Ingraham NE, Jones EK, King S, et al. (2022) Re-aiming equity evaluation in clinical decision support: A scoping review of equity assessments in surgical decision support systems. Ann Surg 277: 359-364. https://doi.org/10.1097/SLA.0000000000005661
|
| [14] |
Balch J, Upchurch GR, Bihorac A, et al. (2021) Bridging the artificial intelligence valley of death in surgical decision-making. Surgery 169: 746-748. https://doi.org/10.1016/j.surg.2021.01.008
|
| [15] |
Kanth P, Inadomi JM (2021) Screening and prevention of colorectal cancer. BMJ 374: n1855. https://doi.org/10.1136/bmj.n1855
|
| [16] |
Lauby-Secretan B, Vilahur N, Bianchini F, et al. (2018) International agency for research on cancer handbook working group The IARC perspective on colorectal cancer screening. N Engl J Med 378: 1734-1740. https://doi.org/10.1056/NEJMsr1714643
|
| [17] |
Mitsala A, Tsalikidis C, Pitiakoudis M, et al. (2021) Artificial intelligence in colorectal cancer screening, diagnosis and treatment. A New Era. Curr Oncol 28: 1581-1607. https://doi.org/10.3390/curroncol28030149
|
| [18] | Hewitson P, Glasziou P, Irwig L, et al. (2007) Screening for colorectal cancer using the fecal occult blood test, Hemoccult. Cochrane Database Syst Rev 1: CD001216. https://doi.org/10.1002/14651858.CD001216.pub2 |
| [19] |
Hu HP, Niu ZJ, Bai YP, et al. (2015) Cancer classification based on gene expression using neural networks. Genet Mol Res 14: 17605-17611. https://doi.org/10.4238/2015.December.21.33
|
| [20] |
Xu G, Zhang M, Zhu H, et al. (2017) A 15-gene signature for prediction of colon cancer recurrence and prognosis based on SVM. Gene 604: 33-40. https://doi.org/10.1016/j.gene.2016.12.016
|
| [21] | Wang Q, Wei J, Chen Z, et al. (2019) Establishment of multiple diagnosis models for colorectal cancer with artificial neural networks. Oncol Lett 17: 3314-3322. https://doi.org/10.3892/ol.2019.10010 |
| [22] |
Chang KH, Miller N, Kheirelseid EAH, et al. (2011) MicroRNA signature analysis in colorectal cancer: Identification of expression profiles in stage II tumors associated with aggressive disease. Int J Color Dis 26: 1415-1422. https://doi.org/10.1007/s00384-011-1279-4
|
| [23] | Herreros-Villanueva M, Duran-Sanchon S, Martín AC, et al. (2019) Plasma MicroRNA signature validation for early detection of colorectal cancer. Clin. Transl. Gastroenterol 10: e00003. https://doi.org/10.14309/ctg.0000000000000003 |
| [24] |
Xuan P, Dong Y, Guo Y, et al. (2018) Dual convolutional neural network based method for predicting disease-related miRNAs. Int J Mol Sci 19: 3732. https://doi.org/10.3390/ijms19123732
|
| [25] |
Morris EJA, Rutter MD, Finan PJ, et al. (2014) Post-colonoscopy colorectal cancer (PCCRC) rates vary considerably depending on the method used to calculate them: A retrospective observational population-based study of PCCRC in the English National Health Service. Gut 64: 1248-1256.
|
| [26] |
Wang P, Berzin TM, Brown JRG, et al. (2019) Real-time automatic detection system increases colonoscopic detection rates of polyps and adenomas: A prospective controlled study. Gut 68: 1813-1819. https://doi.org/10.1136/gutjnl-2018-317500
|
| [27] |
Mori Y, Kudo SE, Berzin TM, et al. (2017) Computer-aided diagnosis for colonoscopy. Endoscopy 49: 813-819.
|
| [28] |
Deliwala SS, Hamid K, Barbarawi M, et al. (2021) Artificial intelligence (AI) real-time detection vs. routine colonoscopy for colorectal neoplasia: A meta-analysis and trial sequential analysis. Int J Colorectal Dis 36: 2291-2303. https://doi.org/10.1007/s00384-021-03929-3
|
| [29] |
Hori K, Ikematsu H, Yamamoto Y, et al. (2022) Detecting colon polyps in endoscopic images using artificial intelligence constructed with automated collection of annotated images from an endoscopy reporting system. Dig Endosc 34: 1021-1029. https://doi.org/10.1111/den.14185
|
| [30] |
Hassan C, Balsamo G, Lorenzetti R, et al. (2022) Artificial intelligence allows leaving-in-situ colorectal polyps. Clin Gastroenterol Hepatol 20: 2505-2513.e4. https://doi.org/10.1016/j.cgh.2022.04.045
|
| [31] | Ruggiero Bollino, Giampaolo Bovenzi, Francesco Cipolletta, et al. (2022) Synergy-Net: Artificial intelligence at the service of oncological prevention. Handbook of Artificial Intelligence in Healthcare. Intelligent Systems Reference Library, vol 211 . Cham: Springer 389-424. https://doi.org/10.1007/978-3-030-79161-2_16 |
| [32] |
Kudo SE, Ichimasa K, Villard B, et al. (2021) Artificial intelligence system to determine risk of T1 colorectal cancer metastasis to lymph node. Gastroenterology 160: 1075-1084.e2. https://doi.org/10.1053/j.gastro.2020.09.027
|
| [33] |
Ferrari R, Mancini-Terracciano C, Voena C, et al. (2019) MR-based artificial intelligence model to assess response to therapy in locally advanced rectal cancer. Eur J Radiol 118: 1-9. https://doi.org/10.1016/j.ejrad.2019.06.013
|
| [34] |
Shi L, Zhang Y, Nie K, et al. (2019) Machine learning for prediction of chemoradiation therapy response in rectal cancer using pre-treatment and mid-radiation multi-parametric MRI. Magn Reson Imaging 61: 33-40. https://doi.org/10.1016/j.mri.2019.05.003
|
| [35] |
Abraham JP, Magee D, Cremolini C, et al. (2021) Clinical validation of a machine-learning-derived signature predictive of outcomes from first-line oxaliplatin-based chemotherapy in advanced colorectal cancer. Clin Cancer Res 27: 1174-1183. https://doi.org/10.1158/1078-0432.CCR-20-3286
|
| [36] |
Oyaga-Iriarte E, Insausti A, Sayar O, et al. (2019) Prediction of irinotecan toxicity in metastatic colorectal cancer patients based on machine learning models with pharmacokinetic parameters. J Pharmacol Sci 140: 20-25. https://doi.org/10.1016/j.jphs.2019.03.004
|
| [37] | Prashanth R, Barsouk A (2019) Epidemiology of gastric cancer: Global trends, risk factors and prevention. Prz Gastroenterol 14: 26-38. https://doi.org/10.5114/pg.2018.80001 |
| [38] | American Cancer SocietyKey statistics about stomach cancer (2024). Available from: https://www.cancer.org/cancer/stomach-cancer/about/key-statistics.html#:~:text=How%20common%20is%20stomach%20cancer,6%2C740%20men%20and%204%2C440%20women |
| [39] |
Rugge M, Fassan M, Graham DY (2015) Epidemiology of gastric cancer. Gastric Cancer 2015: 23-34. https://doi.org/10.1007/978-3-319-15826-6_2
|
| [40] |
Amin MB, Greene FL, Edge SB, et al. (2017) The eighth edition AJCC cancer staging manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J Clin 67: 93-99. https://doi.org/10.3322/caac.21388
|
| [41] |
Sano T, Coit DG, Kim HH, et al. (2017) Proposal of a new stage grouping of gastric cancer for TNM classification: International gastric cancer association staging project. Gastric Cancer 20: 217-225. https://doi.org/10.1007/s10120-016-0601-9
|
| [42] |
Luo H, Xu G, Li C, et al. (2019) Real-time artificial intelligence for detection of upper gastrointestinal cancer by endoscopy: A multicentre, case-control, diagnostic study. Lancet Oncol 20: 1645-1654. https://doi.org/10.1016/S1470-2045(19)30637-0
|
| [43] | Sakai Y, Takemoto S, Hori K, et al. (2018) Automatic detection of early gastric cancer in endoscopic images using a transferrine convolutional neural network. Annu Int Conf IEEE Eng Med Biol Soc 2018: 4138-4141. https://doi.org/10.1109/EMBC.2018.8513274 |
| [44] |
Hirasawa T, Aoyama K, Tanimoto T, et al. (2018) Application of artificial intelligence using a convolutional neural network for detecting gastric cancer in endoscopic images. Gastric Cancer 21: 653-660. https://doi.org/10.1007/s10120-018-0793-2
|
| [45] |
Wu L, Zhou W, Wan X, et al. (2019) A deep neural network improves endoscopic detection of early gastric cancer without blind spots. Endoscopy 51: 522-531. https://doi.org/10.1055/a-0855-3532
|
| [46] |
Correa P, Piazuelo MB (2012) The gastric precancerous cascade. J Dig Dis 13: 2-9. https://doi.org/10.1111/j.1751-2980.2011.00550.x
|
| [47] |
Guimarães P, Keller A, Fehlmann T, et al. (2020) Deep-learning based detection of gastric precancerous conditions. Gut 69: 4-6. https://doi.org/10.1136/gutjnl-2019-319347
|
| [48] |
Horiuchi Y, Aoyama K, Tokai Y, et al. (2020) Convolutional neural network for differentiating gastric cancer from gastritis using magnified endoscopy with narrow band imaging. Dig Dis Sci 65: 1355-1363. https://doi.org/10.1007/s10620-019-05862-6
|
| [49] |
Ueyama H, Kato Y, Akazawa Y, et al. (2021) Application of artificial intelligence using a convolutional neural network for diagnosis of early gastric cancer based on magnifying endoscopy with narrow-band imaging. J Gastroenterol Hepatol 36: 482-489. https://doi.org/10.1111/jgh.15190
|
| [50] |
Li L, Chen Y, Shen Z, et al. (2020) Convolutional neural network for the diagnosis of early gastric cancer based on magnifying narrow band imaging. Gastric Cancer 23: 126-132. https://doi.org/10.1007/s10120-019-00992-2
|
| [51] | Wang FH, Shen L, Li J, et al. (2019) The Chinese Society of Clinical Oncology (CSCO): clinical guidelines for the diagnosis and treatment of gastric cancer. Cancer Commun (Lond) 39: 10. https://doi.org/10.1186/s40880-019-0349-9 |
| [52] |
Huang Z, Liu D, Chen X, et al. (2020) Retrospective imaging studies of gastric cancer: Study protocol clinical trial (SPIRIT Compliant). Medicine (Baltimore) 99: e19157. https://doi.org/10.1097/MD.0000000000019157
|
| [53] | Li C, Zhang S, Zhang H, et al. (2012) Using the K-nearest neighbor algorithm for the classification of lymph node metastasis in gastric cancer. Comput Math Methods Med 2012: 876545. https://doi.org/10.1155/2012/876545 |
| [54] |
Li C, Shi C, Zhang H, et al. (2015) Multiple instance learning for computer aided detection and diagnosis of gastric cancer with dual-energy CT imaging. J Biomed Inform 57: 358-368. https://doi.org/10.1016/j.jbi.2015.08.017
|
| [55] |
Abe S, Oda I, Shimazu T, et al. (2011) Depth-predicting score for differentiated early gastric cancer. Gastric Cancer 14: 35-40. https://doi.org/10.1007/s10120-011-0002-z
|
| [56] |
Zhu Y, Wang QC, Xu MD, et al. (2019) Application of convolutional neural network in the diagnosis of the invasion depth of gastric cancer based on conventional endoscopy. Gastrointest Endosc 89: 806-815.e1. https://doi.org/10.1016/j.gie.2018.11.011
|
| [57] |
Nagao S, Tsuji Y, Sakaguchi Y, et al. (2020) Highly accurate artificial intelligence systems to predict the invasion depth of gastric cancer: Efficacy of conventional white-light imaging, nonmagnifying narrow-band imaging, and indigo-carmine dye contrast imaging. Gastrointest Endosc 92: 866-873.e1. https://doi.org/10.1016/j.gie.2020.06.047
|
| [58] |
Jiang Y, Xie J, Han Z, et al. (2018) Immunomarker support vector machine classifier for prediction of gastric cancer survival and adjuvant chemotherapeutic benefit. Clin Cancer Res 24: 5574-5584. https://doi.org/10.1158/1078-0432.CCR-18-0848
|
| [59] | Lu F, Chen ZK, Yuan X, Li Q, Du ZD, Luo L, Zhang FY MMHG: Multi-modal Hypergraph Learning for Overall Survival After D2 Gastrectomy for Gastric Cancer. 2017: Proceedings of the 15th Intl Conf on Dependable, Autonomic and Secure Computing, 15th Intl Conf on Pervasive Intelligence and Computing, 3rd Intl Conf on Big Data Intelligence and Computing and Cyber Science and Technology Congress; 2017 Nov 6–10; Orlando, FL, USA. California: IEEE Computer Society 164-169. https://doi.org/10.1109/DASC-PICom-DataCom-CyberSciTec.2017.40 |
| [60] |
Hensler K, Waschulzik T, Mönig SP, et al. (2005) Quality-assured Efficient Engineering of Feedforward Neural Networks (QUEEN) -- pretherapeutic estimation of lymph node status in patients with gastric carcinoma. Methods Inf Med 44: 647-654. https://doi.org/10.1055/s-0038-1634021
|
| [61] |
Jagric T, Potrc S, Jagric T (2010) Prediction of liver metastases after gastric cancer resection with the use of learning vector quantization neural networks. Dig Dis Sci 55: 3252-3261. https://doi.org/10.1007/s10620-010-1155-z
|
| [62] |
Jiang Y, Zhang Z, Yuan Q, et al. (2022) Predicting peritoneal recurrence and disease-free survival from CT images in gastric cancer with multitask deep learning: A retrospective study. Lancet Digit Health 4: e340-e350. https://doi.org/10.1016/S2589-7500(22)00040-1
|
| [63] |
Sechopoulos I, Teuwen J, Mann R (2021) Artificial intelligence for breast cancer detection in mammography and digital breast tomosynthesis: State of the art. Semin Cancer Biol 72: 214-225. https://doi.org/10.1016/j.semcancer.2020.06.002
|
| [64] |
Plevritis SK, Munoz D, Kurian AW (2018) Association of screening and treatment with breast cancer mortality by molecular subtype in us women, 2000–2012. J Am Med Assoc 319: 154-164. https://doi.org/10.1001/jama.2017.19130
|
| [65] |
Sechopoulos I, Mann RM (2020) Stand-alone artificial intelligence-The future of breast cancer screening?. Breast 49: 254-260. https://doi.org/10.1016/j.breast.2019.12.014
|
| [66] |
Birdwell RL, Ikeda DM, O'Shaughnessy KF, et al. (2001) Mammographic characteristics of 115 missed cancers later detected with screening mammography and the potential utility of computer-aided detection. Radiology 219: 192-202. https://doi.org/10.1148/radiology.219.1.r01ap16192
|
| [67] |
Warren Burhenne LJ, Wood SA, D'Orsi CJ (2000) Potential contribution of computer-aided detection to the sensitivity of screening mammography. Radiology 215: 554-562. https://doi.org/10.1148/radiology.215.2.r00ma15554
|
| [68] |
Freer TW, Ulissey MJ (2001) Screening mammography with computer-aided detection: prospective study of 12,860 patients in a community breast center. Radiology 220: 781-786. https://doi.org/10.1148/radiol.2203001282
|
| [69] |
Destounis SV, DiNitto P, Logan-Young W, et al. (2004) Can computer-aided detection with double reading of screening mammograms help decrease the false-negative rate?. Radiology 232: 578-584. https://doi.org/10.1148/radiol.2322030034
|
| [70] |
Lehman CD, Wellman RD, Buist DSM, et al. (2015) Diagnostic accuracy of digital screening mammography with and without computer-aided detection. JAMA Int Med 175: 1828-1837. https://doi.org/10.1001/jamainternmed.2015.5231
|
| [71] |
McDonald ES, Clark AS, Tchou J, et al. (2016) Clinical diagnosis and management of breast cancer. J Nucl Med 57: 9S-16S. https://doi.org/10.2967/jnumed.115.157834
|
| [72] |
Destounis SV, Santacroce A, Arieno A (2020) Update on breast density, risk estimation, and supplemental screening. Am J Roentgenol 214: 296-305. https://doi.org/10.2214/AJR.19.21994
|
| [73] | D'Orsi CJ (2013) ACR BI-RADS atlas: Breast imaging reporting and data system. Reston: American College of Radiology. |
| [74] |
Mohamed AA, Berg WA, Peng H, et al. (2018) A deep learning method for classifying mammographic breast density categories. Med Phys 45: 314-321. https://doi.org/10.1002/mp.12683
|
| [75] |
Lehman CD, Yala A, Schuster T, et al. (2019) Mammographic breast density assessment using deep learning: clinical implementation. Radiology 290: 52-58. https://doi.org/10.1148/radiol.2018180694
|
| [76] |
Dontchos BN, Yala A, Barzilay R, et al. (2021) External validation of a deep learning model for predicting mammographic breast density in routine clinical practice. Acad Radiol 28: 475-480. https://doi.org/10.1016/j.acra.2019.12.012
|
| [77] |
Kallenberg M, Petersen K, Nielsen M, et al. (2016) Unsupervised deep learning applied to breast density segmentation and mammographic risk scoring. IEEE Trans Med Imaging 35: 1322-1331. https://doi.org/10.1109/TMI.2016.2532122
|
| [78] |
Gastounioti A, Pantalone L, Scott CG, et al. (2021) Fully automated volumetric breast density estimation from digital breast tomosynthesis. Radiology 301: 561-568. https://doi.org/10.1148/radiol.2021210190
|
| [79] |
Lorkowski J, Grzegorowska O, Pokorski M (2021) Artificial intelligence in the healthcare system: An overview. Adv Exp Med Biol 1335: 1-10. https://doi.org/10.1007/5584_2021_620
|
| [80] |
Gruson D, Helleputte T, Rousseau P, et al. (2019) Data science, artificial intelligence and machine learning: Opportunities for laboratory medicine and the value of positive regulation. Clin Biochem 69: 1-7. https://doi.org/10.1016/j.clinbiochem.2019.04.013
|
| [81] |
Wang B, Zheng J, Yu JF, et al. (2022) Development of artificial intelligence for parathyroid recognition during endoscopic thyroid surgery. Laryngoscope 132: 2516-2523. https://doi.org/10.1002/lary.30173
|
| [82] |
Avci SN, Isiktas G, Ergun O, et al. (2022) A visual deep learning model to predict abnormal versus normal parathyroid glands using intraoperative autofluorescence signals. J Surg Oncol 126: 263-267. https://doi.org/10.1002/jso.26884
|
| [83] |
Akbulut S, Erten O, Kim YS, et al. (2021) Development of an algorithm for intraoperative autofluorescence assessment of parathyroid glands in primary hyperparathyroidism using artificial intelligence. Surgery 170: 454-461. https://doi.org/10.1016/j.surg.2021.01.033
|
| [84] |
Squires MH, Jarvis R, Shirley LA, et al. (2019) Intraoperative parathyroid autofluorescence detection in patients with primary hyperparathyroidism. Ann Surg Oncol 26: 1142-1148. https://doi.org/10.1245/s10434-019-07161-w
|
| [85] |
Randolph GW, Duh QY, Heller KS, et al. (2012) American Thyroid Association Surgical Affairs Committee's Taskforce on Thyroid Cancer Nodal Surgery. The prognostic significance of nodal metastases from papillary thyroid carcinoma can be stratified based on the size and number of metastatic lymph nodes, as well as the presence of extranodal extension. Thyroid 22: 1144-1152. https://doi.org/10.1089/thy.2012.0043
|
| [86] |
Esce AR, Redemann JP, Sanchez AC, et al. (2021) Predicting nodal metastases in papillary thyroid carcinoma using artificial intelligence. Am J Surg 222: 952-958. https://doi.org/10.1016/j.amjsurg.2021.05.002
|
| [87] |
Esce A, Redemann JP, Olson GT, et al. (2023) Lymph node metastases in papillary thyroid carcinoma can be predicted by a convolutional neural network: A multi-institution study. Ann Otol Rhinol Laryngol 132: 1373-1379. https://doi.org/10.1177/00034894231158464
|
| [88] |
Wang C, Yu P, Zhang H, et al. (2023) Artificial intelligence-based prediction of cervical lymph node metastasis in papillary thyroid cancer with CT. Eur Radiol 33: 6828-6840. https://doi.org/10.1007/s00330-023-09700-2
|
| [89] |
Hoang JK, Sosa JA, Nguyen XV, et al. (2015) Thyroid disease imaging: Updates, imaging approach, and management pearls. Radiol Clin North Am 53: 145-161. https://doi.org/10.1016/j.rcl.2014.09.002
|
| [90] |
Lee YH, Baek JH, Jung SL, et al. (2015) Ultrasound-guided fine needle aspiration of thyroid nodules: A consensus statement from the Korean Society of thyroid radiology. Corean J Radiol 16: 391-401. https://doi.org/10.3348/kjr.2015.16.2.391
|
| [91] |
Wang Y, Ge X, Ma H, et al. (2021) Deep learning in medical ultrasound image analysis: A review. IEEE Access 9: 54310-24. https://doi.org/10.1109/access.2021.3071301
|
| [92] | Hirning T, Zuna I, Schlaps D, et al. (1989) Quantification and classification of echographic findings in the thyroid gland by computerized b-mode texture analysis. Eur J Radiol 9: 244-247. |
| [93] |
Tsantis S, Cavouras D, Kalatzis I, et al. (2005) Development of a support vector machine-based image analysis system for assessing the thyroid nodule malignancy risk on ultrasound. Ultrasound Med Biol 31: 1451-1459. https://doi.org/10.1016/j.ultrasmedbio.2005.07.009
|
| [94] |
Chang CY, Chen SJ, Tsai MF (2010) Application of support-vector-machine-based method for feature selection and classification of thyroid nodules in ultrasound images. Pattern Recogn 43: 3494-3506. https://doi.org/10.1016/j.patcog.2010.04.023
|
| [95] |
Iakovidis DK, Keramidas EG, Maroulis D (2010) Fusion of fuzzy statistical distributions for classification of thyroid ultrasound patterns. Artif Intell Med 50: 33-41. https://doi.org/10.1016/j.artmed.2010.04.004
|
| [96] |
Fernandez S, Ito T, Cruz-Piris L, et al. (2022) Fuzzy ontology-based system for driver behavior classification. Sensors (Basel) 22: 7954. https://doi.org/10.3390/s22207954
|
| [97] |
Kezlarian B, Lin O (2021) Artificial intelligence in thyroid fine needle aspiration biopsies. Acta Cytol 65: 324-329. https://doi.org/10.1159/000512097
|
| [98] |
Savala R, Dey P, Gupta N (2018) Artificial neural network model to distinguish follicular adenoma from follicular carcinoma on fine needle aspiration of thyroid. Diagn Cytopathol 46: 244-249. https://doi.org/10.1002/dc.23880
|
| [99] | Shapiro NA, Poloz TL, Shkurupij VA, et al. (2007) Application of artificial neural network for classification of thyroid follicular tumors. Anal Quant Cytol Histol 29: 87-94. |
| [100] |
Chen KY, Chen CN, Wu MH, et al. (2011) Computerized detection and quantification of microcalcifications in thyroid nodules. Ultrasound Med Biol 37: 870-878. https://doi.org/10.1016/j.ultrasmedbio.2011.03.002
|
| [101] |
Choi WJ, Park JS, Kim KG, et al. (2015) Computerized analysis of calcification of thyroid nodules as visualized by ultrasonography. Eur J Radiol 84: 1949-1953. https://doi.org/10.1016/j.ejrad.2015.06.021
|
Figures(1) / Tables(4)

Giuseppe Palomba, Agostino Fernicola, Marcello Della Corte, Marianna Capuano, Giovanni Domenico De Palma, Giovanni Aprea. Artificial intelligence in screening and diagnosis of surgical diseases: A narrative review[J]. AIMS Public Health, 2024, 11(2): 557-576. doi: 10.3934/publichealth.2024028







 DownLoad:
DownLoad: