Periodontal diseases (PD) seem to appear today as predictors of some cardiovascular diseases (CVD). There is a lack of data on the oral health among Cameroonian military population, and its relationship with CVD.
Investigate on the link between oral health of Cameroonian military from the Ngaoundéré garrison and their cardiovascular risk profile.
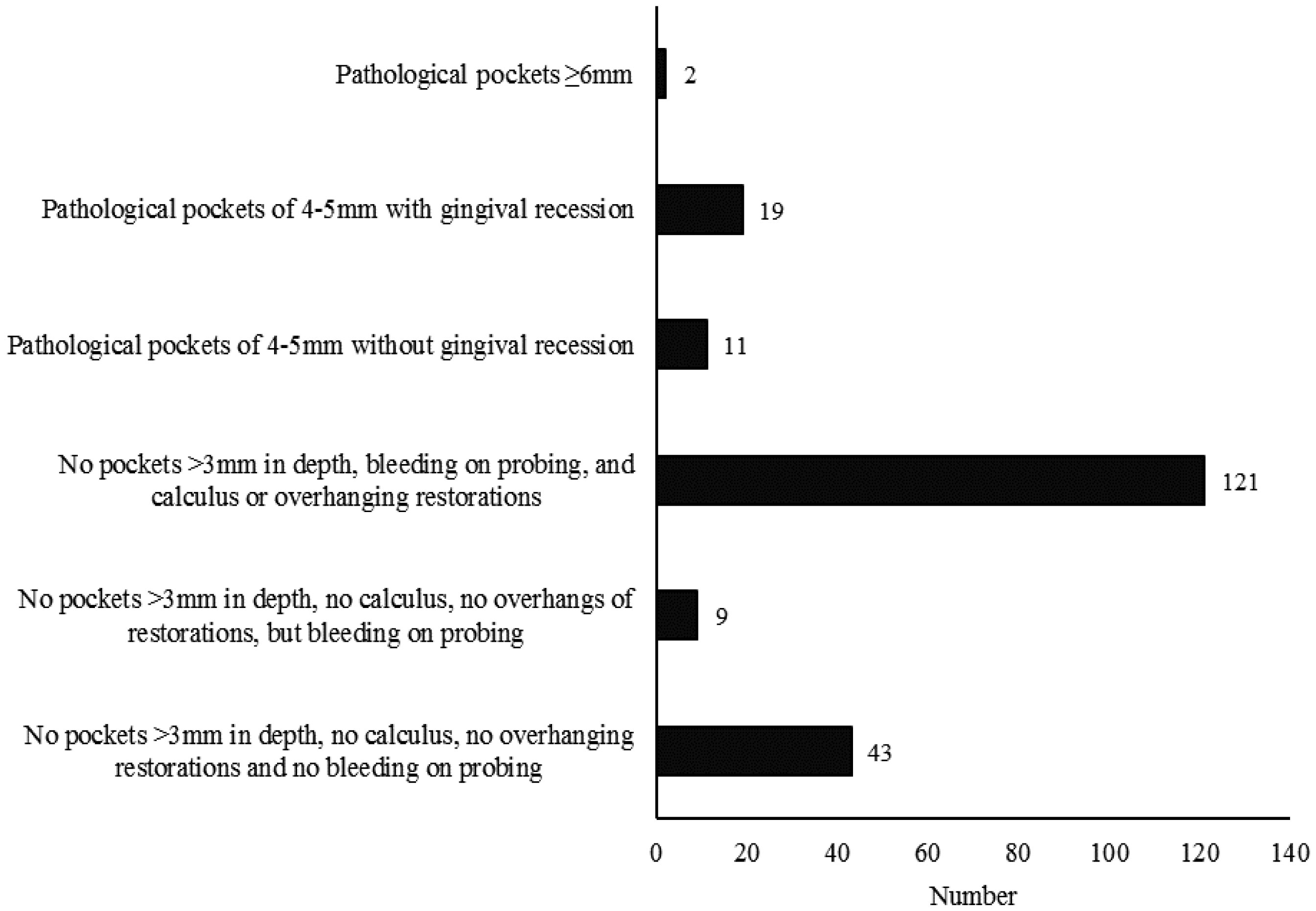
A cross-sectional study at the Fifth Military Sector Health Center in Ngaoundéré was conducted. General health parameters assessment was done according to the World Health Organization STEPS manual for surveillance of risk factors for non-communicable chronic diseases and the Alcohol Use Disorders Identification Test. The periodontal status was assessed using Dutch Periodontal Screening Index.
Two hundred and five participants who were officers and non-commissioned officers (aged 47 ± 08 and 32 ± 08 years respectively), with 86.4% of men were included. Smoking was associated to periodontitis (OR = 4.44 [1.73–11.43], p = 0.0031). Quality of oral hygiene was associated to high cardiovascular risk profile, poor/good (OR = 3.96 [1.07–14.57], p = 0.0386) and medium/good (OR = 3.44 [1.11–10.66], p = 0.0322).
Lifestyle as tobacco consumption and poor oral hygiene were associated to CVD among military, and this call for change.
Citation: W Bell Ngan, L Essama Eno Belinga, SAP Essam Nlo'o, E Abeng Mbozo'o, E Otsomoti, J Mekoulou Ndongo, EC Bika Lele, D Hupin, SH Mandengue, F Roche, B Bongue. Oral health status and cardiovascular risk profile in Cameroonian military population[J]. AIMS Public Health, 2021, 8(1): 100-109. doi: 10.3934/publichealth.2021008
Periodontal diseases (PD) seem to appear today as predictors of some cardiovascular diseases (CVD). There is a lack of data on the oral health among Cameroonian military population, and its relationship with CVD.
Investigate on the link between oral health of Cameroonian military from the Ngaoundéré garrison and their cardiovascular risk profile.
A cross-sectional study at the Fifth Military Sector Health Center in Ngaoundéré was conducted. General health parameters assessment was done according to the World Health Organization STEPS manual for surveillance of risk factors for non-communicable chronic diseases and the Alcohol Use Disorders Identification Test. The periodontal status was assessed using Dutch Periodontal Screening Index.
Two hundred and five participants who were officers and non-commissioned officers (aged 47 ± 08 and 32 ± 08 years respectively), with 86.4% of men were included. Smoking was associated to periodontitis (OR = 4.44 [1.73–11.43], p = 0.0031). Quality of oral hygiene was associated to high cardiovascular risk profile, poor/good (OR = 3.96 [1.07–14.57], p = 0.0386) and medium/good (OR = 3.44 [1.11–10.66], p = 0.0322).
Lifestyle as tobacco consumption and poor oral hygiene were associated to CVD among military, and this call for change.

| [1] | WHO Global status report on non-communicable diseases 2018 Internet (2020) .Available from: http://apps.who.int/iris/bitstream/10665/148114/1/9789241564854_eng.pdf. |
| [2] |
Somma P, Lo Muzio L, Mansueto G, et al. (2005) Squamous cell carcinoma of the lower lip: FAS/FASL expression, lymphocyte subtypes and outcome. Int J Immunopathol Pharmacol 18: 59-64. doi: 10.1177/039463200501800107

|
| [3] |
Celetti A, Testa D, Staibano S, et al. (2005) Overexpression of the cytokine osteopontin identifies aggressive laryngeal squamous cell carcinomas and enhances carcinoma cell proliferation and invasiveness. Clin Cancer Res 11: 8019-8027. doi: 10.1158/1078-0432.CCR-05-0641
|
| [4] |
Humphrey LL, Fu R, Buckley DI, et al. (2008) Periodontal Disease and Coronary Heart Disease Incidence: A Systematic Review and Meta-analysis. J Gen Intern Med 23: 2079-2086. doi: 10.1007/s11606-008-0787-6
|
| [5] | Blaizot A, Vergnes JN, Nuwwareh S, et al. (2009) Periodontal diseases and cardiovascular events: meta-analysis of observational studies. Int Dent J 59: 197-209. |
| [6] |
Thomas D, Praveen S, Clemens W, et al. (2013) The epidemiological evidence behind the association between periodontitis and incident atherosclerotic cardiovascular disease. J Clin Periodontol 40: 70-84. doi: 10.1111/jcpe.12062
|
| [7] | Schmitt A, Carra MC, Boutourye P, et al. (2016) Parodontite et rigidité artérielle: revue systématique et méta-analyse. JPIO 42: 977-987. |
| [8] | Belinga LEE, Ngan WB, Lemougoum D, et al. (2018) Association between periodontal diseases and cardiovascular diseases in Cameroon. J Public Health Afr 9: 761. |
| [9] |
Sanz M, Castillo AMD, Jepsen S, et al. (2020) Periodontitis and cardiovascular diseases: Consensus report. J Clin Periodontol 47: 268-288. doi: 10.1111/jcpe.13189
|
| [10] |
Otomo-Corgel J, Pucher JJ, Rethman MP, et al. (2012) State of science: chronic periodontitis and systemic health. J Evid Base Dent Pract 12: 20-28. doi: 10.1016/S1532-3382(12)70006-4
|
| [11] |
Lockhart PB, Bolger AF, Papapanou PN, et al. (2012) Periodontal Disease and Atherosclerotic Vascular Disease: Does the Evidence Support an Independent Association? A scientific statement from the American Hearth Association. Circulation 125: 2520-2544. doi: 10.1161/CIR.0b013e31825719f3
|
| [12] | Leong XF, Ng CY, Badiah B, et al. (2014) Association between Hypertension and Periodontitis: Possible Mechanisms. Sci World J 2014: 768237. |
| [13] |
D'Aiuto F, Orlandi M, Gunsolley J, et al. (2013) Evidence that periodontal treatment improves biomarkers and CVD outcomes. J Periodontol 84: S85-S105. doi: 10.1902/jop.2013.134007
|
| [14] |
Roth GA, Johnson C, Abajobir A, et al. (2017) Global, Regional, and National Burden of Cardiovascular Diseases for 10 Causes, 1990 to 2015. J Am Coll Cardiol 70: 1-25. doi: 10.1016/j.jacc.2017.04.052
|
| [15] |
Watt RG, Sheiham A (2012) Integrating the common risk factor approach into a social determinants framework. Community Dent Oral Epidemiol 40: 289-296. doi: 10.1111/j.1600-0528.2012.00680.x
|
| [16] |
de Nigris F, Cacciatore F, Mancini FP, et al. (2018) Epigenetic Hallmarks of Fetal Early Atherosclerotic Lesions in Humans. JAMA Cardiol 3: 1184-1191. doi: 10.1001/jamacardio.2018.3546
|
| [17] |
Baygi F, Herttua K, Jensen OC, et al. (2020) Global prevalence of cardiometabolic risk factors in the military population: a systematic review and meta-analysis. BMC Endocr Disord 20: 8. doi: 10.1186/s12902-020-0489-6
|
| [18] |
Hoerster KD, Lehavot K, Simpson T (2012) Health and health behavior differences: U.S. Military, veteran, and civilian men. Am J Prev Med 43: 483-489. doi: 10.1016/j.amepre.2012.07.029
|
| [19] |
Suman M, Spalj S, Plancak D, et al. (2008) The influence of war on the oral health of professional soldiers. Int Dent J 58: 71-74. doi: 10.1111/j.1875-595X.2008.tb00178.x
|
| [20] |
Yamashita K, Nishiyama T, Nagata E, et al. (2017) Impact of a 7-Day Field Training on Oral Health Condition in Japan Ground Self-Defense Force Personnel. Mil Med 182: 1869-1877. doi: 10.7205/MILMED-D-16-00383
|
| [21] |
Dakovic D, Lekic M, Bokonjic D, et al. (2020) Evaluation of periodontal status and treatment needs of the Serbian military forces population. Vojnosanit Pregl 10. doi: 10.2298/VSP191125010D
|
| [22] |
Gunepin M, Derache F, Trousselard M, et al. (2018) Impact of chronic stress on periodontal health. J Oral Med Oral Surg 24: 44-50. doi: 10.1051/mbcb/2017028
|
| [23] |
Lloro V, Lozano-de LV, Lloro I, et al. (2019) The Incidence of Dental Needs During Isolated Missions Compared to Non-Isolated Missions: A Systematic Review and Implications for Future Prevention Strategies. Mil Med 184: 148-155. doi: 10.1093/milmed/usy364
|
| [24] | Olivier PM, Diana D, Ngoufack TJO, et al. (2016) A Community-Based Assessment of Hypertension and Some Other Cardiovascular Disease Risk Factors in Ngaoundéré, Cameroon. Int J Hypertens 2016: 4754636. |
| [25] |
Bigna JJ, Nansseu JR, Katte JC, et al. (2018) Prevalence of prediabetes and diabetes mellitus among adults residing in Cameroon: A systematic review and meta-analysis. Diabetes Res Clin Pract 137: 109-118. doi: 10.1016/j.diabres.2017.12.005
|
| [26] |
Kuate DB, Mbanya JC, Kingue S, et al. (2019) Blood pressure and burden of hypertension in Cameroon, a microcosm of Africa: a systematic review and meta-analysis of population-based studies. J Hypertens 37: 2190-2199. doi: 10.1097/HJH.0000000000002165
|
| [27] |
Ndiaye AA, Seck SM, Tall AB, et al. (2015) Les maladies chroniques non transmissibles chez les militaires Sénégalais: étude transversale en 2013. Pan Afr Med J 22. doi: 10.11604/pamj.2015.22.59.4777
|
| [28] |
Van der Velden U (2009) The Dutch periodontal screening index validation and its application in The Netherlands. J Clin Periodontol 36: 1018-1024. doi: 10.1111/j.1600-051X.2009.01495.x
|
Figures(1) / Tables(3)

W Bell Ngan, L Essama Eno Belinga, SAP Essam Nlo'o, E Abeng Mbozo'o, E Otsomoti, J Mekoulou Ndongo, EC Bika Lele, D Hupin, SH Mandengue, F Roche, B Bongue. Oral health status and cardiovascular risk profile in Cameroonian military population[J]. AIMS Public Health, 2021, 8(1): 100-109. doi: 10.3934/publichealth.2021008







 DownLoad:
DownLoad: