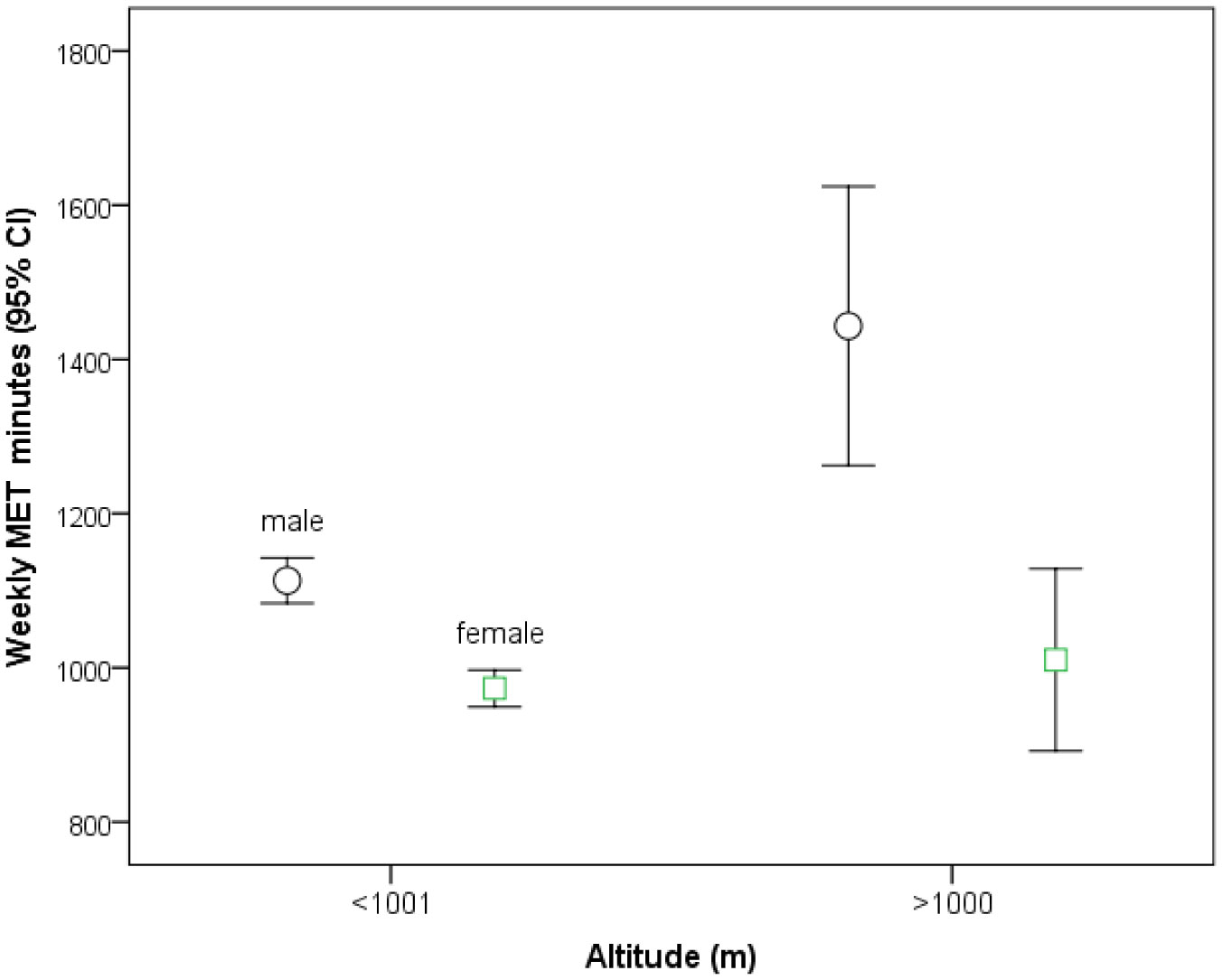
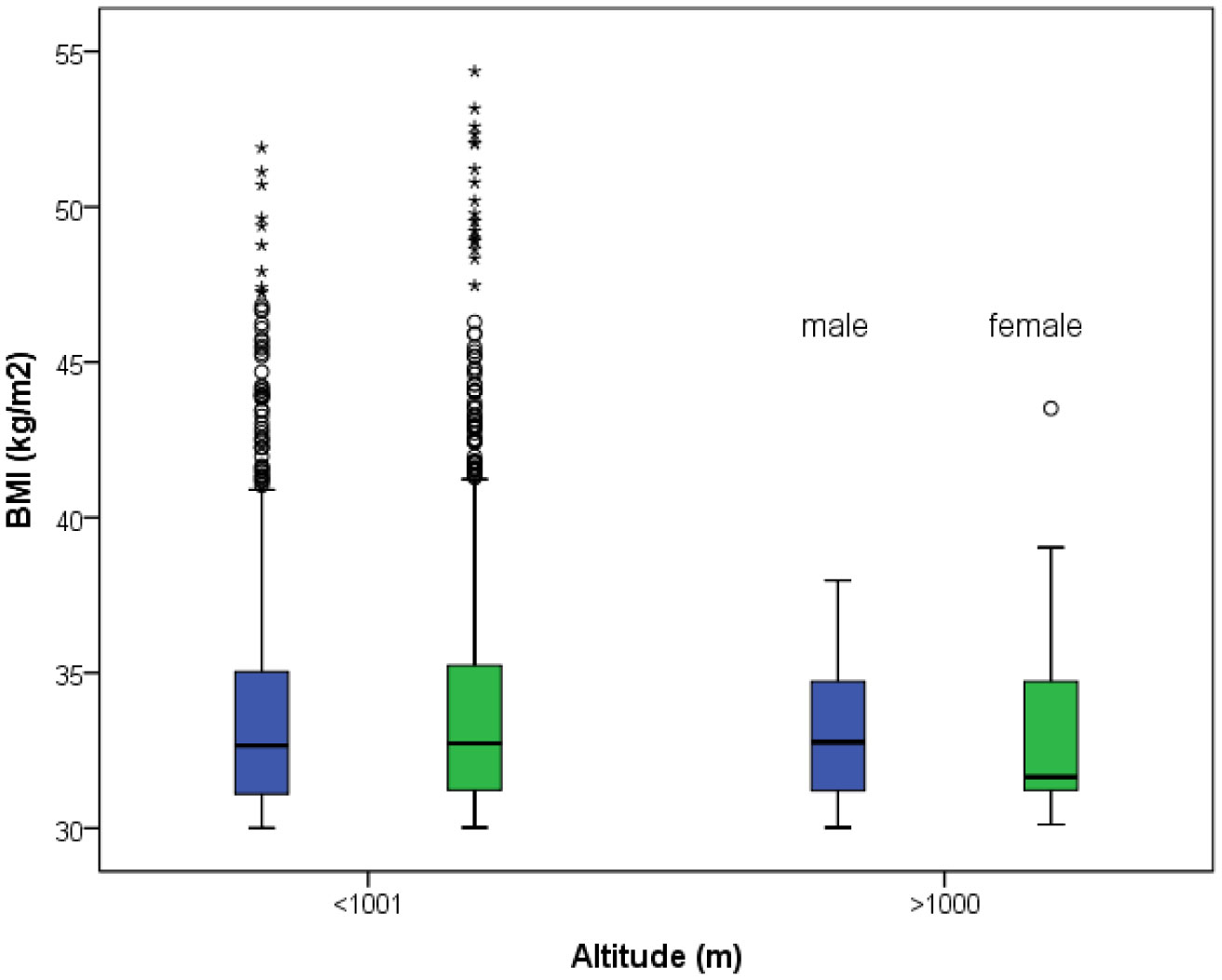
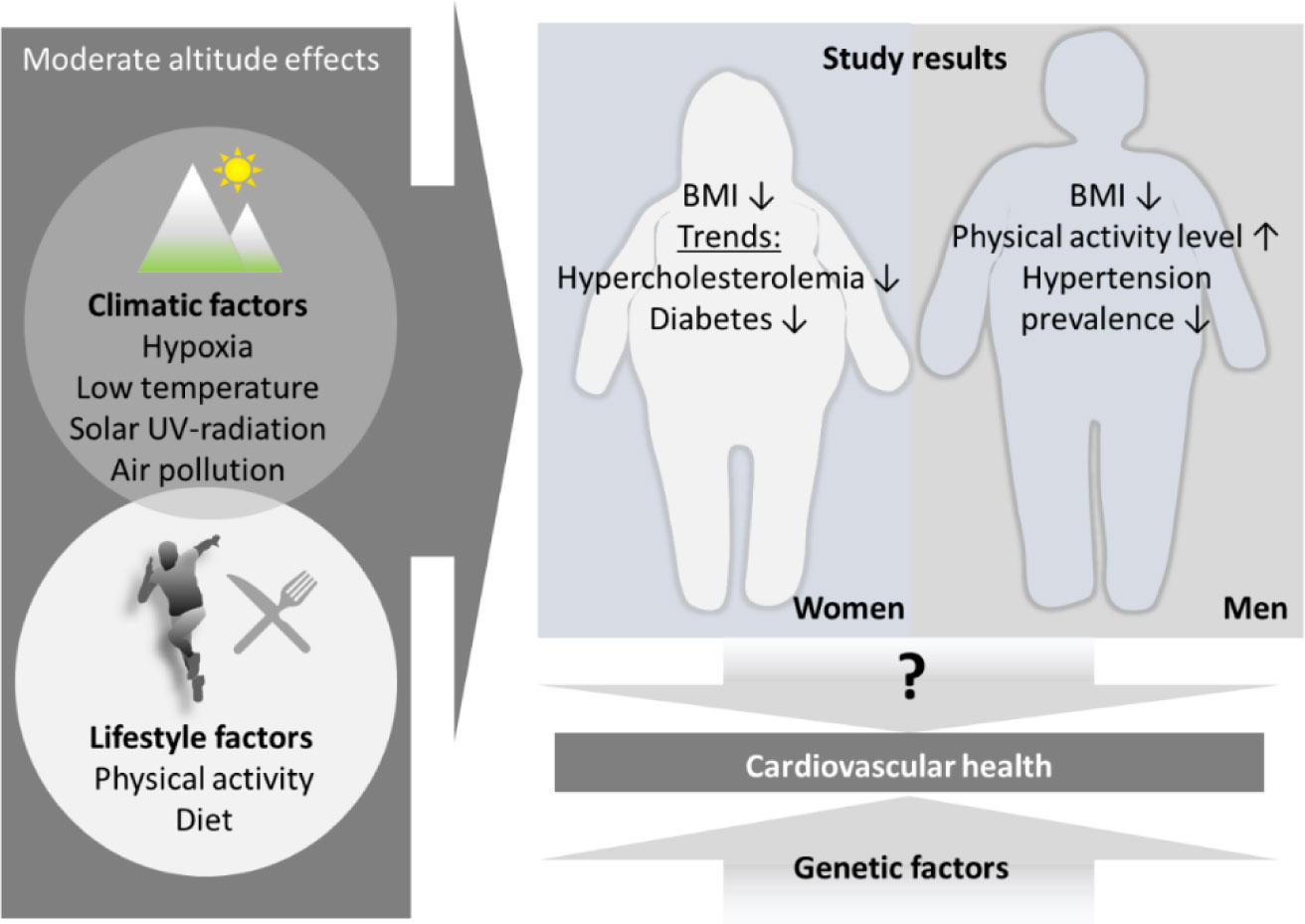
Living at moderate altitude (up to about 2,000 m) was shown to be associated with distinct health benefits, including lower mortality from cardiovascular diseases and certain cancers. However, it remains unclear, whether those benefits are mainly due to environmental conditions (e.g., hypoxia, temperature, solar ultra-violet radiation) or differences in lifestyle behavior, including regular physical activity levels. This study aims to compare altitude-related differences in levels of physical activity and the prevalence of cardiovascular risk factors such as obesity, hypertension, hypercholesterolemia, and diabetes in an Alpine country. We interrogated the Austrian Health Interview Survey (ATHIS) 2019, a nationally representative study of persons aged over 15 years living in private Austrian households. The results confirm a higher prevalence of hypertension (24.2% vs. 16.8%) in men living at low (<1,001 m) compared to those at moderate (1,001 to 2,000 m) altitude. Women living above 1,000 m tend to have a lower prevalence of hypercholesterolemia (14.8% vs. 18.8%) and diabetes (3.2% vs. 5.6%) than their lower living peers. Both sexes have lower average body mass index (BMI) when residing at moderate altitude (men: 25.7, women: 23.9) compared to those living lower (26.6 and 25.2). Severe obesity (BMI > 40) is almost exclusively restricted to low altitude dwellers. Only men report to be more physically active on average when living higher (1,453 vs. 1,113 weekly MET minutes). These novel findings confirm some distinct benefits of moderate altitude residence on heath. Beside climate conditions, differences in lifestyle behavior, i.e., physical activity, have to be considered when interpreting those health-related divergences, and consequently also mortality data, between people residing at low and moderate altitudes.
Citation: Martin Burtscher, Grégoire P Millet, Jeannette Klimont, Johannes Burtscher. Differences in the prevalence of physical activity and cardiovascular risk factors between people living at low (<1,001 m) compared to moderate (1,001–2,000 m) altitude[J]. AIMS Public Health, 2021, 8(4): 624-635. doi: 10.3934/publichealth.2021050
Living at moderate altitude (up to about 2,000 m) was shown to be associated with distinct health benefits, including lower mortality from cardiovascular diseases and certain cancers. However, it remains unclear, whether those benefits are mainly due to environmental conditions (e.g., hypoxia, temperature, solar ultra-violet radiation) or differences in lifestyle behavior, including regular physical activity levels. This study aims to compare altitude-related differences in levels of physical activity and the prevalence of cardiovascular risk factors such as obesity, hypertension, hypercholesterolemia, and diabetes in an Alpine country. We interrogated the Austrian Health Interview Survey (ATHIS) 2019, a nationally representative study of persons aged over 15 years living in private Austrian households. The results confirm a higher prevalence of hypertension (24.2% vs. 16.8%) in men living at low (<1,001 m) compared to those at moderate (1,001 to 2,000 m) altitude. Women living above 1,000 m tend to have a lower prevalence of hypercholesterolemia (14.8% vs. 18.8%) and diabetes (3.2% vs. 5.6%) than their lower living peers. Both sexes have lower average body mass index (BMI) when residing at moderate altitude (men: 25.7, women: 23.9) compared to those living lower (26.6 and 25.2). Severe obesity (BMI > 40) is almost exclusively restricted to low altitude dwellers. Only men report to be more physically active on average when living higher (1,453 vs. 1,113 weekly MET minutes). These novel findings confirm some distinct benefits of moderate altitude residence on heath. Beside climate conditions, differences in lifestyle behavior, i.e., physical activity, have to be considered when interpreting those health-related divergences, and consequently also mortality data, between people residing at low and moderate altitudes.

| [1] |
Faeh D, Gutzwiller F, Bopp M, et al. (2099) Lower mortality from coronary heart disease and stroke at higher altitudes in Switzerland. Circulation 120: 495-501. doi: 10.1161/CIRCULATIONAHA.108.819250

|
| [2] |
Burtscher M (2016) Lower mortality rates in those living at moderate altitude. Aging (Albany NY) 8: 2603-2604. doi: 10.18632/aging.101057
|
| [3] |
Burtscher J, Millet GP, Burtscher M (2021) Does living at moderate altitudes in Austria affect mortality rates of various causes? An ecological study. BMJ Open 11: e048520. doi: 10.1136/bmjopen-2020-048520
|
| [4] |
Ekelund U, Tarp J, Steene-Johannessen J, et al. (2019) Dose-response associations between accelerometry measured physical activity and sedentary time and all cause mortality: systematic review and harmonised meta-analysis. BMJ 366: l4570. doi: 10.1136/bmj.l4570
|
| [5] |
Burtscher J, Ruedl G, Posch M, et al. (2019) The upper limit of cardiorespiratory fitness associated with longevity: an update. AIMS Public Health 6: 225-228. doi: 10.3934/publichealth.2019.3.225
|
| [6] |
Millet GP, Debevec T, Brocherie F, et al. (2021) Altitude and COVID-19: Friend or foe? A narrative review. Physiol Rep 8: e14615. doi: 10.14814/phy2.14615
|
| [7] | Klimont J (2020) Österreichische Gesundheitsbefragung 2019 Vienna: Bundesministerium für Soziales, Gesundheit, Pflege und Konsumentenschutz (BMSGPK), Available from: https://www.sozialministerium.at/Themen/Gesundheit/Gesundheitssystem/Gesundheitsberichte/%C3%96sterreichische-Gesundheitsbefragung-2014-(ATHIS).html. |
| [8] |
Piercy KL, Troiano RP, Ballard RM, et al. (2018) The Physical Activity Guidelines for Americans. JAMA 320: 2020-2028. doi: 10.1001/jama.2018.14854
|
| [9] |
Myers J, Prakash M, Froelicher V, et al. (2002) Exercise capacity and mortality among men referred for exercise testing. N Engl J Med 346: 793-801. doi: 10.1056/NEJMoa011858
|
| [10] |
Arem H, Moore SC, Patel A, et al. (2015) Leisure time physical activity and mortality: a detailed pooled analysis of the dose-response relationship. JAMA Intern Med 175: 959-967. doi: 10.1001/jamainternmed.2015.0533
|
| [11] | Santos-Lozano A, Barrán AT, Fernández-Navarro P, et al. (2021) Association between physical activity and cardiovascular risk factors: Dose and sex matter. J Sport Health Sci . |
| [12] |
Voss JD, Allison DB, Webber BJ, et al. (2014) Lower obesity rate during residence at high altitude among a military population with frequent migration: a quasi experimental model for investigating spatial causation. PLoS One 9: e93493. doi: 10.1371/journal.pone.0093493
|
| [13] |
Kayser B, Verges S (2013) Hypoxia, energy balance and obesity: from pathophysiological mechanisms to new treatment strategies. Obes Rev 14: 579-592. doi: 10.1111/obr.12034
|
| [14] | Kayser B, Verges S (2021) Hypoxia, energy balance, and obesity: An update. Obes Rev 22: e13192. |
| [15] |
Dwivedi AK, Dubey P, Cistola DP, et al. (2020) Association Between Obesity and Cardiovascular Outcomes: Updated Evidence from Meta-analysis Studies. Curr Cardiol Rep 22: 25. doi: 10.1007/s11886-020-1273-y
|
| [16] |
Barone I, Giordano C, Bonofiglio D, et al. (2020) The weight of obesity in breast cancer progression and metastasis: Clinical and molecular perspectives. Semin Cancer Biol 60: 274-284. doi: 10.1016/j.semcancer.2019.09.001
|
| [17] |
Aghili SMM, Ebrahimpur M, Arjmand B, et al. (2021) Obesity in COVID-19 era, implications for mechanisms, comorbidities, and prognosis: a review and meta-analysis. Int J Obes (Lond) 45: 998-1016. doi: 10.1038/s41366-021-00776-8
|
| [18] |
Seclén SN, Nunez-Robles E, Yovera-Aldana M, et al. (2020) Incidence of COVID-19 infection and prevalence of diabetes, obesity and hypertension according to altitude in Peruvian population. Diabetes Res Clin Pract 169: 108463. doi: 10.1016/j.diabres.2020.108463
|
| [19] |
Pietiläinen KH, Kaprio J, Borg P, et al. (2008) Physical inactivity and obesity: a vicious circle. Obesity (Silver Spring) 16: 409-414. doi: 10.1038/oby.2007.72
|
| [20] |
Wander K, Su M, Mattison PM, et al. (2020) High-altitude adaptations mitigate risk for hypertension and diabetes-associated anemia. Am J Phys Anthropol 172: 156-164. doi: 10.1002/ajpa.24032
|
| [21] | Burtscher M (2014) Effects of living at higher altitudes on mortality: a narrative review. Aging Dis 5: 274-280. |
| [22] |
Mortimer EA, Monson RR, MacMahon B (1977) Reduction in mortality from coronary heart disease in men residing at high altitude. N Eng J Med 296: 581-585. doi: 10.1056/NEJM197703172961101
|
| [23] |
Faeh D, Moser A, Panczak R, et al. (2016) Independent at heart: persistent association of altitude with ischaemic heart disease mortality after consideration of climate, topography and built environment. J Epidemiol Community Health 70: 798-806. doi: 10.1136/jech-2015-206210
|
| [24] |
Ezzati M, Horwitz ME, Thomas DS, et al. (2012) Altitude, life expectancy and mortality from ischaemic heart disease, stroke, COPD and cancers: national population-based analysis of US counties. J Epidemiol Community Health 66: e17. doi: 10.1136/jech.2010.112938
|
| [25] |
Thiersch M, Swenson ER (2018) High Altitude and Cancer Mortality. High Alt Med Biol 19: 116-123. doi: 10.1089/ham.2017.0061
|
| [26] |
Woolcott OO, Castillo OA, Gutierrez C, et al. (2014) Inverse association between diabetes and altitude: a cross-sectional study in the adult population of the United States. Obesity (Silver Spring) 22: 2080-2090. doi: 10.1002/oby.20800
|
| [27] |
Woolcott OO, Castillo OA, Torres J, et al. (2002) Serum leptin levels in dwellers from high altitude lands. High Alt Med Biol 3: 245-246. doi: 10.1089/15270290260131975
|
| [28] |
Lopez-Pascual A, Arévalo J, Martínez JA, et al. (2018) Inverse Association Between Metabolic Syndrome and Altitude: A Cross-Sectional Study in an Adult Population of Ecuador. Front Endocrinol (Lausanne) 9: 658. doi: 10.3389/fendo.2018.00658
|
| [29] |
Lopez-Pascual A, Bes-Rastrollo M, Sayón-Orea C, et al. (2017) Living at a geographically higher elevation is associated with lower risk of metabolic syndrome: prospective analysis of the SUN cohort. Front Physiol 7: 658. doi: 10.3389/fphys.2016.00658
|
| [30] |
Lo MY, Daniels JD, Levine BD, et al. (2013) Sleeping altitude and sudden cardiac death. Am Heart J 166: 71-75. doi: 10.1016/j.ahj.2013.04.003
|
| [31] |
Burtscher M, Faulhaber M, Flatz M, et al. (2006) Effects of short-term acclimatization to altitude (3200 m) on aerobic and anaerobic exercise performance. Int J Sports Med 27: 629-635. doi: 10.1055/s-2005-872823
|
| [32] |
Semenza GL (2012) Hypoxia-inducible factors in physiology and medicine. Cell 148: 399-408. doi: 10.1016/j.cell.2012.01.021
|
| [33] |
Ban HS, Uno M, Nakamura H (2010) Suppression of hypoxia-induced HIF-1alpha accumulation by VEGFR inhibitors: Different profiles of AAL993 versus SU5416 and KRN633. Cancer Lett 296: 17-26. doi: 10.1016/j.canlet.2010.03.010
|
| [34] |
Ambrosini G, Nath AK, Sierra-Honigmann MR, et al. (2002) Transcriptional activation of the human leptin gene in response to hypoxia. Involvement of hypoxia-inducible factor 1. J Biol Chem 277: 34601-34609. doi: 10.1074/jbc.M205172200
|
| [35] |
Palmer BF, Clegg DJ (2014) Ascent to altitude as a weight loss method: the good and bad of hypoxia inducible factor activation. Obesity (Silver Spring) 22: 311-317. doi: 10.1002/oby.20499
|
| [36] |
Park S, Kario K, Chia YC, et al. (2020) The influence of the ambient temperature on blood pressure and how it will affect the epidemiology of hypertension in Asia. J Clin Hypertens (Greenwich) 22: 438-444. doi: 10.1111/jch.13762
|
| [37] |
Hirschler V, Gonzalez C, Molinari C, et al. (2019) Blood pressure level increase with altitude in three argentinean indigenous communities. AIMS Public Health 6: 370-379. doi: 10.3934/publichealth.2019.4.370
|
| [38] |
Mäkinen TM, Mäntysaari M, Pääkkönen T, et al. (2008) Autonomic nervous function during whole-body cold exposure before and after cold acclimation. Aviat Space Environ Med 79: 875-882. doi: 10.3357/ASEM.2235.2008
|
| [39] |
van der Lans AA, Hoeks J, Brans B, et al. (2013) Cold acclimation recruits human brown fat and increases nonshivering thermogenesis. J Clin Invest 123: 3395-3403. doi: 10.1172/JCI68993
|
| [40] |
Weller RB (2017) The health benefits of UV radiation exposure through vitamin D production or non-vitamin D pathways. Blood pressure and cardiovascular disease. Photochem Photobiol Sci 16: 374-380. doi: 10.1039/C6PP00336B
|
| [41] |
Najafi E, Khanjani N, Ghotbi MR, et al. (2019) The association of gastrointestinal cancers (esophagus, stomach, and colon) with solar ultraviolet radiation in Iran-an ecological study. Environ Monit Assess 191: 152. doi: 10.1007/s10661-019-7263-0
|
Figures(3) / Tables(3)

Martin Burtscher, Grégoire P Millet, Jeannette Klimont, Johannes Burtscher. Differences in the prevalence of physical activity and cardiovascular risk factors between people living at low (<1,001 m) compared to moderate (1,001–2,000 m) altitude[J]. AIMS Public Health, 2021, 8(4): 624-635. doi: 10.3934/publichealth.2021050







 DownLoad:
DownLoad: