In the rural areas of Saudi Arabia, which are not connected to the national grid, electricity is supplied mainly from diesel generators. This is not just a non-renewable energy source, but it has also resulted in environmental damage and may be hazardous to human health. In order to mitigate the problem, integration with a solar photovoltaic system is proposed. A Photovoltaic-Diesel Hybrid System (PvDHS) was designed, analyzed, and optimized based on the climate data of Yanbu, Saudi Arabia. Measured local solar insolation and climate data were used in the Hybrid Optimization Model for Electric Renewables (HOMER) software with different system components and configurations in order to optimize the design that yields the best energy cost. A system consisting of a 3 kW photovoltaic system, a 2 kW diesel engine, a 1 kW converter, and 14 kWh batteries were identified to be the most cost-effective for the average daily electricity demand of 10.5 kWh. The total Net Present Cost (NPC) of this system is $17, 800, a reduction of 50% over the $35, 770 cost of the diesel-only system. The PvDHS useful electrical energy is found to be $0.36/kWh, while the Cost of Energy (COE) of the diesel-only system is $0.72/kWh. The system is expected to pay for itself in 2.8 years and reduce CO2 emissions by 8110 kg per year.
Citation: Abshir Ashour, Taib Iskandar Mohamad, Kamaruzzaman Sopian, Norasikin Ahmad Ludin, Khaled Alzahrani, Adnan Ibrahim. Performance optimization of a photovoltaic-diesel hybrid power system for Yanbu, Saudi Arabia[J]. AIMS Energy, 2021, 9(6): 1260-1273. doi: 10.3934/energy.2021058
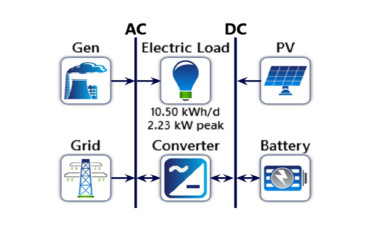
In the rural areas of Saudi Arabia, which are not connected to the national grid, electricity is supplied mainly from diesel generators. This is not just a non-renewable energy source, but it has also resulted in environmental damage and may be hazardous to human health. In order to mitigate the problem, integration with a solar photovoltaic system is proposed. A Photovoltaic-Diesel Hybrid System (PvDHS) was designed, analyzed, and optimized based on the climate data of Yanbu, Saudi Arabia. Measured local solar insolation and climate data were used in the Hybrid Optimization Model for Electric Renewables (HOMER) software with different system components and configurations in order to optimize the design that yields the best energy cost. A system consisting of a 3 kW photovoltaic system, a 2 kW diesel engine, a 1 kW converter, and 14 kWh batteries were identified to be the most cost-effective for the average daily electricity demand of 10.5 kWh. The total Net Present Cost (NPC) of this system is $17, 800, a reduction of 50% over the $35, 770 cost of the diesel-only system. The PvDHS useful electrical energy is found to be $0.36/kWh, while the Cost of Energy (COE) of the diesel-only system is $0.72/kWh. The system is expected to pay for itself in 2.8 years and reduce CO2 emissions by 8110 kg per year.

| [1] | Saudi Arabia-Urban Issues (2020) Available from: https://unhabitat.org/saudi-arabia-urban-issues. |
| [2] |
Bawah U, Addoweesh KE, Eltamaly AM (2013) Comparative study of economic viability of rural electrification using renewable energy resources versus the diesel generator option in Saudi Arabia. J Renewable Sustainable Energy 5: 042701. doi: 10.1063/1.4812646

|
| [3] |
Ghenai C, Bettayeb M, Brdjanin B, et al. (2019) Hybrid solar PV/PEM fuel Cell/Diesel generator power system for cruise ships: A case study in Stockholm, Sweden. Case Stud in Therm Eng 14: 100497. doi: 10.1016/j.csite.2019.100497
|
| [4] |
Post HN, Thomas MG (1988) Photovoltaic systems for current and future applications. Sol Energy 41: 465-473. doi: 10.1016/0038-092X(88)90020-5
|
| [5] |
Mahmoud M (1990) Experience results and techno-economic feasibility of using photovoltaic generators instead of diesel motors for water pumping from rural desert wells in Jordan. IEE Proc C Gener, Transm Distrib 137: 391-394. doi: 10.1049/ip-c.1990.0053
|
| [6] |
Shaahid SM, Elhadidy MA (2007) Technical and economic assessment of grid-independent hybrid photovoltaic‑diesel‑battery power systems for commercial loads in desert environments. Renewable Sustainable Energy Rev 11: 1794-1810. doi: 10.1016/j.rser.2006.03.001
|
| [7] |
Oparaku OU (2002) Assessment of the cost-effectiveness of photovoltaic systems for telecommunications in Nigeria. Int J Sol Energy 22: 123-129. doi: 10.1080/0142591031000094551
|
| [8] |
Mazzeo D, Matera N, De Luca P, et al. (2021) A literature review and statistical analysis of photovoltaic-wind hybrid renewable system research by considering the most relevant 550 articles: An upgradable matrix literature database. J Cleaner Prod 295: 126070. doi: 10.1016/j.jclepro.2021.126070
|
| [9] | Ball GJ (2016) Grid-Connected PV systems, In Reinders A., Verlinden P., Sark W. and Freundlich A., Photovoltaic Solar Energy. Wiley Online Library, 511-529. Available from: https://doi.org/10.1002/9781118927496.ch46. |
| [10] | Stapleton G, Neill S (2012) Grid-connected solar electric systems: The earthscan expert handbook for planning, design and ınstallation, 1st Ed., Routledge, ISBN 9780367787486. |
| [11] |
Gharibi M, Askarzadeh A (2019) Size and power exchange optimization of a grid-connected diesel generator-photovoltaic-fuel cell hybrid energy system considering reliability, cost and renewability. Int J Hydrogen Energy 44: 25428-25441. doi: 10.1016/j.ijhydene.2019.08.007
|
| [12] | Hankins M (2010) Stand-alone solar electric systems: The earthscan expert handbook for planning, design and ınstallation, 1st Ed. ISBN 9780367787509. |
| [13] |
Hocaoğlu FO, Gerek ÖN, Kurban M (2019) A novel hybrid (wind-photovoltaic) system sizing procedure. Sol Energy 83: 2019-2028. doi: 10.1016/j.solener.2009.07.010
|
| [14] |
Smaoui M, Abdelkafi A, Krichen L (2015) Optimal sizing of stand-alone photovoltaic/wind/hydrogen hybrid system supplying a desalination unit. Sol Energy 120: 263-276. doi: 10.1016/j.solener.2015.07.032
|
| [15] |
Bahramara S, Parsa Moghaddam M, Haghifam MR (2016) Optimal planning of hybrid renewable energy systems using HOMER: A review. Renewable Sustainable Energy Rev 62: 609-620. doi: 10.1016/j.rser.2016.05.039
|
| [16] |
Kaabeche A, Ibtiouen R (2014) Techno-economic optimization of hybrid photovoltaic/wind/diesel/battery generation in a stand-alone power system. Sol Energy 103: 171-182. doi: 10.1016/j.solener.2014.02.017
|
| [17] |
Mazzeo D, Matera N, Bevilacqua P, et al. (2015) Energy and economic analysis of solar photovoltaic plants located at the university of calabria. Int J Heat Tech 33: 41-50. doi: 10.18280/ijht.330406
|
| [18] | Abdul Razak N, Othman M, Musirin I (2010) Optimal sizing and operational strategy of hybrid renewable energy system using homer. 2010 4th International Power Engineering and Optimization Conference (PEOCO), Shah Alam, Malaysia: IEEE, 495-501. Available from: https://doi.org/10.1109/PEOCO.2010.5559240. |
| [19] | Fulzele JB, Dutt S (2011) Optimium planning of hybrid renewable energy system using HOMER. Int J Electrical Com Eng 2: 68-74. |
| [20] | Abbas MK, Qadeer-ul-Hasan (2015) Economic power generation for an off-grid site in Pakistan. Power Gener Syst Renewable Energy Tech: 1-6. |
| [21] | Givler T, Lilienthal P (2005) Using HOMER software, NREL's micropower optimization model, to explore the role of gen-sets in small solar power systems; case study: Sri Lanka. |
| [22] |
Cai W, Li X, Maleki A, et al. (2020) Optimal sizing and location based on economic parameters for an off-grid application of a hybrid system with photovoltaic, battery and diesel technology. Energy 201: 117480. doi: 10.1016/j.energy.2020.117480
|
| [23] |
Dufo-López R, Bernal-Agustín JL (2005) Design and control strategies of PV-Diesel systems using genetic algorithms. Sol Energy 79: 33-46. doi: 10.1016/j.solener.2004.10.004
|
| [24] |
Rehman S, Al-Hadhrami LM (2010) Study of a solar PV-diesel-battery hybrid power system for a remotely located population near Rafha, Saudi Arabia. Energy 35: 4986-4995. doi: 10.1016/j.energy.2010.08.025
|
| [25] |
Mazzeo D, Matera N, Luca PD, et al. (2020) Worldwide geographical mapping and optimization of stand-alone and grid-connected hybrid renewable system techno-economic performance across Köppen-Geiger climates. Appl Energy 276: 115507. doi: 10.1016/j.apenergy.2020.115507
|
| [26] |
Jordan DC, Kurtz SR (2013) Photovoltaic degradation rates—an analytical review. Prog in Photovoltaics: Res Appl 21: 12-29. doi: 10.1002/pip.1182
|
| [27] | Jordan, D. C., and S. R. Kurtz. 2013. "Photovoltaic Degradation Rates-an Analytical Review." Prog in Photovoltaics: Res Appl. Available from: https://doi.org/10.1002/pip.1182. |
| [28] |
Zell E, Gasim S, Wilcox S, et al. (2015) Assessment of solar radiation resources in Saudi Arabia. Sol Energy 119: 422-438. doi: 10.1016/j.solener.2015.06.031
|
| [29] |
Rezzouk H, Mellit A (2015) Feasibility study and sensitivity analysis of a stand-alone photovoltaic‑diesel‑battery hybrid energy system in the north of Algeria. Renewable Sustainable Energy Rev 43: 1134-1150. doi: 10.1016/j.rser.2014.11.103
|
| [30] | Benghanem M, Almohammedi A, Khan MT, et al. (2018) Effect of dust accumulation on the performance of photovoltaic panels in desert countries: A case study for Madinah, Saudi Arabia. Int J Power Electronics Drive Syst 9: 1356-1366. |
| [31] | Saudi Arabia Gasoline Prices. Ministry of Energy, Industry and Mineral Resources, 2021. Available from: https://tradingeconomics.com/saudi-arabia/gasoline-prices. |












Figures(13) / Tables(3)

Abshir Ashour, Taib Iskandar Mohamad, Kamaruzzaman Sopian, Norasikin Ahmad Ludin, Khaled Alzahrani, Adnan Ibrahim. Performance optimization of a photovoltaic-diesel hybrid power system for Yanbu, Saudi Arabia[J]. AIMS Energy, 2021, 9(6): 1260-1273. doi: 10.3934/energy.2021058







 DownLoad:
DownLoad: