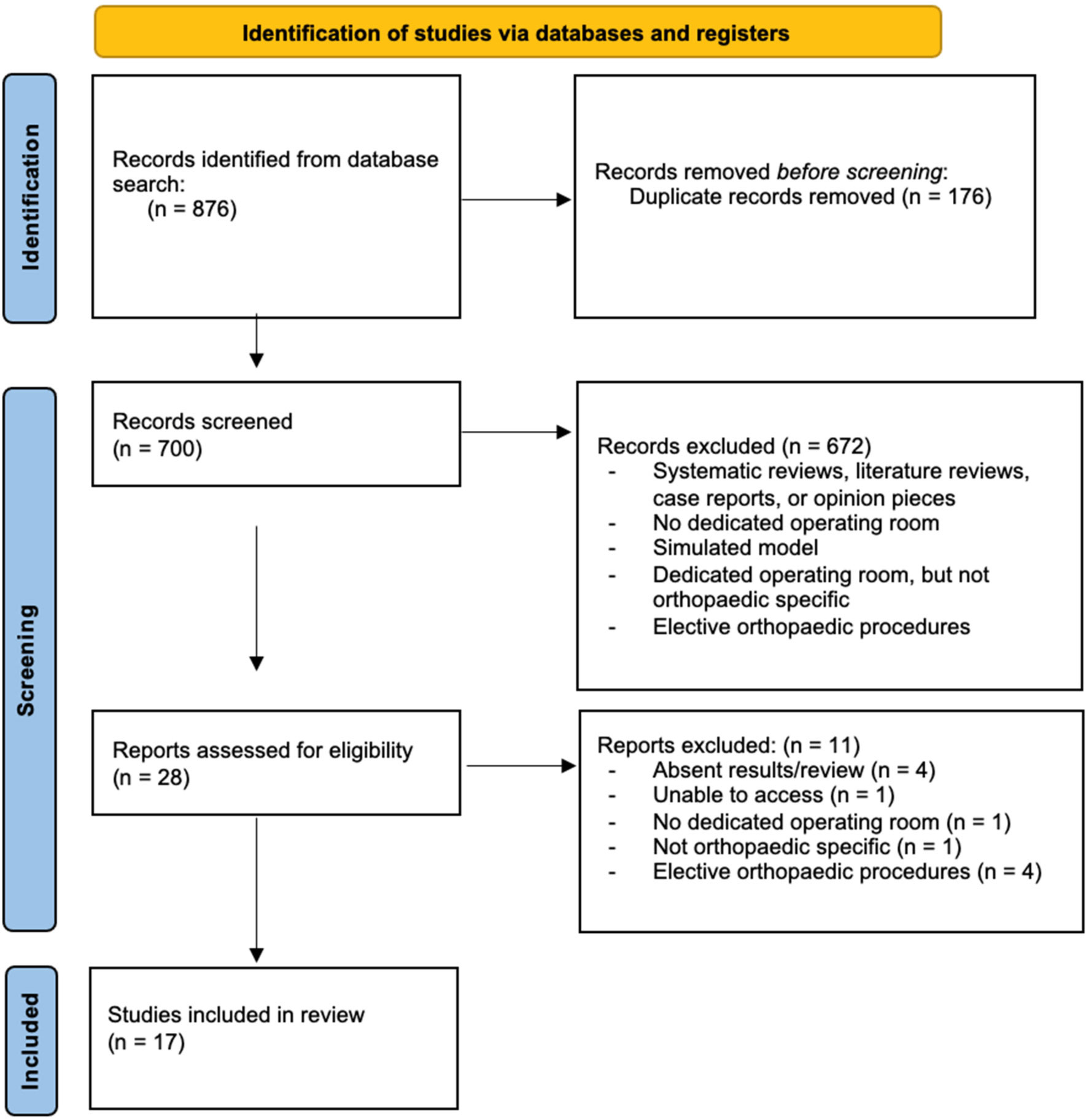
Scheduling urgent, orthopaedic trauma cases has long been a challenge for health care institutions. Traditionally, these cases are scheduled for an operating room (OR) slot in the middle of the night, by “bumping” elective cases to later in the day, by adding a case on after-hours, or by delaying the case for several days until an OR becomes available. As a solution to the challenges facing traditional scheduling modules, trauma centers around the country have instituted the use of a dedicated orthopaedic trauma room (DOTR). While there are multiple studies analyzing the effects of DOTRs on various outcomes, there is not a centralized review of these studies. This paper will serve as a review of the various models of the DOTR as well as the effect of the DOTR on after-hours procedures, time to surgery (TTS), duration of surgery (DOS), length of stay (LOS), cost, and surgical complications. An extensive review of the literature was performed through PubMed and Embase. 17 studies were found to meet eligibility criteria. This review suggests that DOTRs have favorable effects on after-hours procedures, cost, and surgical complications. There is variability in the data regarding the effect on TTS, DOS, and LOS.
Citation: Kathryn Biddle, Kelly Pagidas. Associated outcomes of various iterations of the dedicated orthopaedic trauma room: a literature review[J]. AIMS Medical Science, 2022, 9(3): 450-466. doi: 10.3934/medsci.2022024
Scheduling urgent, orthopaedic trauma cases has long been a challenge for health care institutions. Traditionally, these cases are scheduled for an operating room (OR) slot in the middle of the night, by “bumping” elective cases to later in the day, by adding a case on after-hours, or by delaying the case for several days until an OR becomes available. As a solution to the challenges facing traditional scheduling modules, trauma centers around the country have instituted the use of a dedicated orthopaedic trauma room (DOTR). While there are multiple studies analyzing the effects of DOTRs on various outcomes, there is not a centralized review of these studies. This paper will serve as a review of the various models of the DOTR as well as the effect of the DOTR on after-hours procedures, time to surgery (TTS), duration of surgery (DOS), length of stay (LOS), cost, and surgical complications. An extensive review of the literature was performed through PubMed and Embase. 17 studies were found to meet eligibility criteria. This review suggests that DOTRs have favorable effects on after-hours procedures, cost, and surgical complications. There is variability in the data regarding the effect on TTS, DOS, and LOS.
American Society of Anesthesiologists
American College of Surgeons National Surgery Quality Improvement Program
Operating room
Nil per os
Dedicated orthopaedic trauma room
Dedicated orthopaedic trauma list
Time to surgery
Duration of surgery
Length of stay
Fracture reduction room
Femoral shaft and distal femur fractures
Open reduction and internal fixation

| [1] | American College of Surgeons National Surgical Quality Improvement ProgramUser guide for the 2013 ACS NSQIP participant use data file (PUF) (2014). Available from: https://www.facs.org/~/media/files/quality programs/nsqip/2013_acs_nsqip_puf_user_guide.ashx |
| [2] | American College of Surgeons Verification Review CommitteeResources for optimal care of the injured patient (2019). Available from: https://www.facs.org/quality-programs/trauma/tqp/center-programs/vrc/standards |
| [3] |
Elder GM, Harvey EJ, Vaidya R, et al. (2005) The effectiveness of orthopaedic trauma theatres in decreasing morbidity and mortality: a study of 701 displaced subcapital hip fractures in two trauma centres. Injury 36: 1060-1066. https://doi.org/10.1016/j.injury.2005.05.001 
|
| [4] |
Thompson AL, Seghol H, Davis KJ, et al. (2021) Introducing an orthopaedic trauma list to a regional hospital: Improved efficiencies and patient outcomes. Aust J Rural Health 29: 591-595. https://doi.org/10.1111/ajr.12765
|
| [5] |
Featherall J, Bhattacharyya T (2019) The dedicated orthopaedic trauma room model: adopting a new standard of care. J Bone Joint Surg Am 101: e120. https://doi.org/10.2106/JBJS.19.00352
|
| [6] |
Ricci WM, Gallagher B, Brandt A, et al. (2009) Is after-hours orthopaedic surgery associated with adverse outcomes? A prospective comparative study. J Bone Joint Surg Am 91: 2067-2072. https://doi.org/10.2106/JBJS.H.00661
|
| [7] |
Bhattacharyya T, Vrahas MS, Morrison SM, et al. (2006) The value of the dedicated orthopaedic trauma operating room. J Trauma 60: 1336-1341. https://doi.org/10.1097/01.ta.0000220428.91423.78
|
| [8] |
Charalambous CP, Paschalides K, Gunedran T, et al. (2005) Availability of orthopaedic trauma lists in the United Kingdom. Injury 36: 1156-1158. https://doi.org/10.1016/j.injury.2005.05.023
|
| [9] |
Brusalis CM, Shah AS, Luan X, et al. (2017) A dedicated orthopaedic trauma operating room improves efficiency at a pediatric center. J Bone Joint Surg Am 99: 42-47. https://doi.org/10.2106/JBJS.16.00640
|
| [10] | Lemos D, Nilssen E, Khatiwada B, et al. (2009) Dedicated orthopedic trauma theatres: effect on morbidity and mortality in a single trauma centre. Can J Surg 52: 87-91. |
| [11] |
Steeby SF, Harvin WH, Worley JR, et al. (2018) Use of the dedicated orthopaedic trauma room for open tibia and femur fractures: Does it make a difference?. J Orthop Trauma 32: 377-380. https://doi.org/10.1097/BOT.0000000000001232
|
| [12] |
Wixted JJ, Reed M, Eskander MS, et al. (2008) The effect of an orthopedic trauma room on after-hours surgery at a level one trauma center. J Orthop Trauma 22: 234-236. https://doi.org/10.1097/BOT.0b013e31816c748b
|
| [13] | Chacko AT, Ramirez MA, Ramappa AJ, et al. (2011) Does late night hip surgery affect outcome?. J Trauma 71: 447-453. https://doi.org/10.1097/TA.0b013e3182231ad7 |
| [14] |
Roberts TT, Vanushkina M, Khasnavis S, et al. (2015) Dedicated orthopaedic operating rooms: beneficial to patients and providers alike. J Orthop Trauma 29: e18-e23. https://doi.org/10.1097/BOT.0000000000000154
|
| [15] |
Knight M, Gouk C, Jorgensen NB, et al. (2021) Patient outcomes in Tropical North Queensland after implementation of a dedicated orthopaedic trauma list. ANZ J Surg 91: 986-991. https://doi.org/10.1111/ans.16785
|
| [16] |
Runner R, Moore JrT, Reisman W (2016) Value of a dedicated Saturday orthopaedic trauma operating room. J Orthop Trauma 30: e24-e29. https://doi.org/10.1097/BOT.0000000000000441
|
| [17] |
Taylor M, Hopman W, Yach J (2016) Length of stay, wait time to surgery and 30-day mortality for patients with hip fractures after the opening of a dedicated orthopedic weekend trauma room. Can J Surg 59: 337-341. https://doi.org/10.1503/cjs.017014
|
| [18] |
McDonald M, Ward L, Wortham H, et al. (2021) Effect of a 6 am–9 am dedicated orthopaedic trauma room on hip fracture outcomes in a community level II trauma center. J Orthop Trauma 35: 245-251. https://doi.org/10.1097/BOT.0000000000001966
|
| [19] |
Whitlock PW, Little KJ, Singleton SS, et al. (2019) A dedicated fracture reduction room: a cost-effective alternative to the operating room. J Am Acad Orthop Surg 27: e887-e892. https://doi.org/10.5435/JAAOS-D-17-00800
|
| [20] |
Waters PM, Yang BW, White D, et al. (2018) A dedicated satellite trauma orthopaedic program operating room safely increases capacity. J Bone Joint Surg Am 100: e70. https://doi.org/10.2106/JBJS.17.01368
|
| [21] | Min W, Wolinsky PR (2011) The dedicated orthopedic trauma operating room. J Trauma 71: 513-515. https://doi.org/10.1097/TA.0b013e3182245d30 |
| [22] |
Cloud C, Fong B, Bloise C, et al. (2022) Advantages of a dedicated orthopaedic trauma operating room for diaphyseal femur fractures. J Orthop Trauma 36: 321. https://doi.org/10.1097/BOT.0000000000002319
|
| [23] | Denisiuk M, Layson JT, Bandovic I, et al. (2022) Implementation of a dedicated orthopaedic trauma room in hip and femur fracture care: a 17-year analysis. J Orthop Trauma . in press. https://doi.org/10.1097/BOT.0000000000002413 |
| [24] |
Moody AE, Gurnea TP, Shul CP, et al. (2020) True cost of operating room time: implications for an orthopaedic trauma service. J Orthop Trauma 34: 271-275. https://doi.org/10.1097/BOT.0000000000001688
|
| [25] |
van Veen-Berkx E, Elkhuizen SG, Kuijper B, et al. (2016) Dedicated operating room for emergency surgery generates more utilization, less overtime, and less cancellations. Am J Surg 211: 122-128. https://doi.org/10.1016/j.amjsurg.2015.06.021
|
| [26] |
Parmar D, Woodman M, Pandit JJ (2022) A graphical assessment of emergency surgical list efficiency to determine operating theatre capacity needs. Br J Anaesth 128: 574-583. https://doi.org/10.1016/j.bja.2021.10.033
|
| [27] |
Schoenfelder J, Kohl S, Glaser M, et al. (2021) Simulation-based evaluation of operating room management policies. BMC Health Serv Res 21: 271. https://doi.org/10.1186/s12913-021-06234-5
|
| [28] |
Ferrand Y, Magazine M, Rao U (2010) Comparing two operating-room-allocation policies for elective and emergency surgeries. Proceedings of the 2010 Winter Simulation Conference : 2364-2374. https://doi.org/10.1109/WSC.2010.5678933
|
| [29] |
Wullink G, Van Houdenhoven M, Hans EW, et al. (2007) Closing emergency operating rooms improves efficiency. J Med Syst 31: 543-546. https://doi.org/10.1007/s10916-007-9096-6
|
| [30] |
Bowers J, Mould G (2004) Managing uncertainty in orthopaedic trauma theatres. Eur J Oper Res 154: 599-608. https://doi.org/10.1016/S0377-2217(02)00816-0
|
Figures(1) / Tables(5)

Kathryn Biddle, Kelly Pagidas. Associated outcomes of various iterations of the dedicated orthopaedic trauma room: a literature review[J]. AIMS Medical Science, 2022, 9(3): 450-466. doi: 10.3934/medsci.2022024







 DownLoad:
DownLoad: