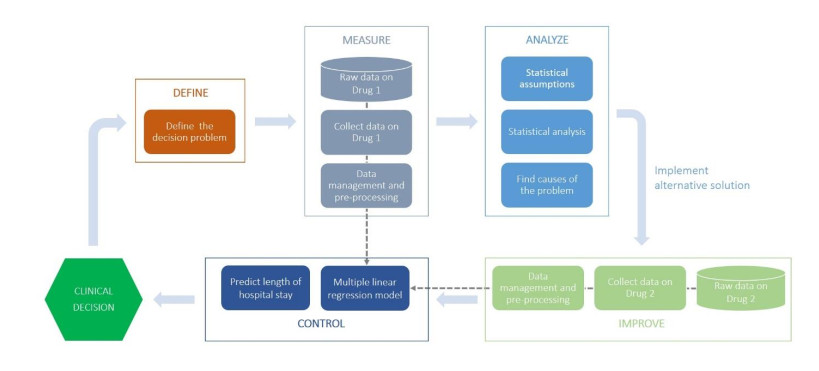
Health Technology Assessment (HTA) and Six Sigma (SS) have largely proved their reliability in the healthcare context. The former focuses on the assessment of health technologies to be introduced in a healthcare system. The latter deals with the improvement of the quality of services, reducing errors and variability in the healthcare processes. Both the approaches demand a detailed analysis, evidence-based decisions, and efficient control plans. In this paper, the SS is applied as a support tool for HTA of two antibiotics with the final aim of assessing their clinical and organizational impact in terms of postoperative Length Of Stay (LOS) for patients undergoing tongue cancer surgery. More specifically, the SS has been implemented through its main tool, namely the DMAIC (Define, Measure, Analyse, Improve, Control) cycle. Moreover, within the DMAIC cycle, a modelling approach based on a multiple linear regression analysis technique is introduced, in the Control phase, to add complementary information and confirm the results obtained by the statistical analysis performed within the other phases of the SS DMAIC. The obtained results show that the proposed methodology is effective to determine the clinical and organizational impact of each of the examined antibiotics, when LOS is taken as a measure of performance, and guide the decision-making process. Furthermore, our study provides a systematic procedure which, properly combining different and well-assessed tools available in the literature, demonstrated to be a useful guidance for choosing the right treatment based on the available data in the specific circumstance.
Citation: Alfonso Maria Ponsiglione, Carlo Ricciardi, Giovanni Improta, Giovanni Dell'Aversana Orabona, Alfonso Sorrentino, Francesco Amato, Maria Romano. A Six Sigma DMAIC methodology as a support tool for Health Technology Assessment of two antibiotics[J]. Mathematical Biosciences and Engineering, 2021, 18(4): 3469-3490. doi: 10.3934/mbe.2021174
Health Technology Assessment (HTA) and Six Sigma (SS) have largely proved their reliability in the healthcare context. The former focuses on the assessment of health technologies to be introduced in a healthcare system. The latter deals with the improvement of the quality of services, reducing errors and variability in the healthcare processes. Both the approaches demand a detailed analysis, evidence-based decisions, and efficient control plans. In this paper, the SS is applied as a support tool for HTA of two antibiotics with the final aim of assessing their clinical and organizational impact in terms of postoperative Length Of Stay (LOS) for patients undergoing tongue cancer surgery. More specifically, the SS has been implemented through its main tool, namely the DMAIC (Define, Measure, Analyse, Improve, Control) cycle. Moreover, within the DMAIC cycle, a modelling approach based on a multiple linear regression analysis technique is introduced, in the Control phase, to add complementary information and confirm the results obtained by the statistical analysis performed within the other phases of the SS DMAIC. The obtained results show that the proposed methodology is effective to determine the clinical and organizational impact of each of the examined antibiotics, when LOS is taken as a measure of performance, and guide the decision-making process. Furthermore, our study provides a systematic procedure which, properly combining different and well-assessed tools available in the literature, demonstrated to be a useful guidance for choosing the right treatment based on the available data in the specific circumstance.

| [1] |
P. Thokala, A. Duenas, Multiple criteria decision analysis for health technology assessment, Value Health, 15 (2012), 1172-1181. doi: 10.1016/j.jval.2012.06.015

|
| [2] |
M. J. Liberatore, Six Sigma in healthcare delivery, Int. J. Health Care Qual. Assur., 26 (2013), 601-626. doi: 10.1108/IJHCQA-09-2011-0054
|
| [3] | K. Facey, L. A. Topfer, L. Chan, Health Technology Assessment (HTA) Glossary, INAHTA-The International Network of Agencies for Health Technology Assessment, 2006. |
| [4] | World Health Organization, Health technology assessment. Available from: https://www.who.int/medical_devices/assessment/en/. |
| [5] |
A. Angelis, P. Kanavos, Multiple Criteria Decision Analysis (MCDA) for evaluating new medicines in Health Technology Assessment and beyond: The Advance Value Framework, Soc. Sci. Med., 188 (2017), 137-156. doi: 10.1016/j.socscimed.2017.06.024
|
| [6] |
D. Dankó, G. Petrova, Health technology assessment in the Balkans: opportunities for a balanced drug assessment system, Biotechnol. Biotechnol. Equip., 28 (2014), 1181-1189. doi: 10.1080/13102818.2014.978636
|
| [7] |
A. Angelis, A. Lange, P. Kanavos, Using health technology assessment to assess the value of new medicines: results of a systematic review and expert consultation across eight European countries, Eur. J. Health Econ., 19 (2018), 123-152. doi: 10.1007/s10198-017-0871-0
|
| [8] | A. Nasution, S. A. S. Sulaiman, A. A. Shafie, PHP33 Drug-Related Problems and Length of Stay in the Management of Infection in Patients with Chronic Kidney Disease, Value Health, 15 (2012), A615. |
| [9] | T. Priyadharshini, Comparison of Nebulised Adrenaline, Nebulised Salbutamol, Nebulised Budesonide in the treatment of Bronchiolitis: A Double Blinded Randomized Trial, Masters thesis, Government Mohan Kumaramangalam Medical College, Salem, 2017. |
| [10] |
L. Sampietro-Colom, I. Morilla-Bachs, S. Gutierrez-Moreno, P. Gallo, Development and test of a decision support tool for hospital health technology assessment, Int. J. Technol. Assess. Health Care, 28 (2012), 460-465. doi: 10.1017/S0266462312000487
|
| [11] |
A. F. Shorr, S. T. Micek, E. C. Welch, J. A. Doherty, R. M. Reichley, M. H. Kollef, Inappropriate antibiotic therapy in Gram-negative sepsis increases hospital length of stay, Crit. Care Med., 39 (2011), 46-51. doi: 10.1097/CCM.0b013e3181fa41a7
|
| [12] | T. N. Desai, R. Shrivastava, Six Sigma-a new direction to quality and productivity management, in Proceedings of the World Congress on Engineering and Computer Science, (2008), 22-24. |
| [13] |
G. Improta, G. Balato, M. Romano, A. M. Ponsiglione, E. Raiola, M. A. Russo, et al., Improving performances of the knee replacement surgery process by applying DMAIC principles, J. Eval. Clin. Pract., 23 (2017), 1401-1407. doi: 10.1111/jep.12810
|
| [14] |
G. Improta, G. Guizzi, C. Ricciardi, V. Giordano, A. M. Ponsiglione, G. Converso, et al., Agile six sigma in healthcare: Case study at santobono pediatric hospital, Int. J. Environ. Res. Public. Health, 17 (2020), 1052. doi: 10.3390/ijerph17031052
|
| [15] |
J. de Mast, J. Lokkerbol, An analysis of the Six Sigma DMAIC method from the perspective of problem solving, Int. J. Prod. Econ., 139 (2012), 604-614. doi: 10.1016/j.ijpe.2012.05.035
|
| [16] |
R. Brown, P. Grehan, M. Brennan, D. Carter, A. Brady, E. Moore, et al., Using Lean Six Sigma to improve rates of day of surgery admission in a national thoracic surgery department, Int. J. Qual. Health Care, 31 (2019), 14-21. doi: 10.1093/intqhc/mzz083
|
| [17] |
D. S. Chang, J. D. Leu, W. S. Wang, Y. C. Chen, Improving waiting time for surgical rooms using workflow and the six-sigma method, Total Qual. Manag. Bus. Excell., 31 (2020), 869-886. doi: 10.1080/14783363.2018.1456329
|
| [18] |
E. P. Tagge, A. S. Thirumoorthi, J. Lenart, C. Garberoglio, K. W. Mitchell, Improving operating room efficiency in academic children's hospital using Lean Six Sigma methodology, J. Pediatr. Surg., 52 (2017), 1040-1044. doi: 10.1016/j.jpedsurg.2017.03.035
|
| [19] |
G. Improta, G. Balato, C. Ricciardi, M. A. Russo, I. Santalucia, M. Triassi, et al., Lean Six Sigma in healthcare: Fast track surgery for patients undergoing prosthetic hip replacement surgery, TQM J., 31 (2019), 526-540. doi: 10.1108/TQM-10-2018-0136
|
| [20] |
C. Ricciardi, A. Fiorillo, A. S. Valente, A. Borrelli, C. Verdoliva, M. Triassi, et al., Lean Six Sigma approach to reduce LOS through a diagnostic-therapeutic-assistance path at AORNA Cardarelli, TQM J., 31 (2019), 657-672. doi: 10.1108/TQM-02-2019-0065
|
| [21] |
A. Scala, A. M. Ponsiglione, I. Loperto, A. Della Vecchia, A. Borrelli, G. Russo, et al., Lean Six Sigma Approach for Reducing Length of Hospital Stay for Patients with Femur Fracture in a University Hospital, Int. J. Environ. Res. Public. Health, 18 (2021), 2843. doi: 10.3390/ijerph18062843
|
| [22] |
A. Al Kuwaiti, A.V. Subbarayalu, Reducing hospital-acquired infection rate using the Six Sigma DMAIC approach, Saudi J. Med. Med. Sci., 5 (2017), 260. doi: 10.4103/sjmms.sjmms_98_16
|
| [23] |
G. Improta, M. Cesarelli, P. Montuori, L. C. Santillo, M. Triassi, Reducing the risk of healthcare-associated infections through Lean Six Sigma: The case of the medicine areas at the Federico II University Hospital in Naples (Italy), J. Eval. Clin. Pract., 24 (2018), 338-346. doi: 10.1111/jep.12844
|
| [24] |
E. Montella, M. V. D. Cicco, A. Ferraro, P. Centobelli, E. Raiola, M. Triassi, et al., The application of Lean Six Sigma methodology to reduce the risk of healthcare-associated infections in surgery departments, J. Eval. Clin. Pract., 23 (2017), 530-539. doi: 10.1111/jep.12662
|
| [25] | V. S. M, S. Mahalingam, S. N. K. M, Improving patients' satisfaction in a mobile hospital using Lean Six Sigma - a design-thinking intervention, Prod. Plan. Control, 31 (2020), 512-526. |
| [26] |
M. Godley, J. B. Jenkins, Decreasing wait times and increasing patient satisfaction: a lean six sigma approach, J. Nurs. Care Qual., 34 (2019), 61-65. doi: 10.1097/NCQ.0000000000000332
|
| [27] | N. V. Fursule, S. V. Bansod, S. N. Fursule, Understanding the benefits and limitations of Six Sigma methodology, Int. J. Sci. Res. Publ., 2 (2012), 1-9. |
| [28] | H. de Koning, J. P. S. Verver, J. van den Heuvel, S. Bisgaard, R. J. M. M. Does, Lean six sigma in healthcare, J. Healthcare. Qual., 28 (2006), 4-11. |
| [29] | C. Ricciardi, A. Sorrentino, G. Improta, V. Abbate, I. Latessa, A. Perrone, et al., A health technology assessment between two pharmacological therapies through Six Sigma: the case study of bone cancer, TQM J., 32 (2020), 1507-1524. |
| [30] |
E. Polverejan, J. C. Gardiner, C. J. Bradley, M. Holmes‐Rovner, D. Rovner, Estimating mean hospital cost as a function of length of stay and patient characteristics, Health Econ., 12 (2003), 935-947. doi: 10.1002/hec.774
|
| [31] |
E. Kulinskaya, D. Kornbrot, H. Gao, Length of stay as a performance indicator: robust statistical methodology, IMA J. Manag. Math., 16 (2005), 369-381. doi: 10.1093/imaman/dpi015
|
| [32] | Publications Office of the European Union, Tools and methodologies to assess the efficiency of health care services in Europe: An overview of current approaches and opportunities for improvement, Report by the Expert Group on Health System Performance Assessment. Available from: http://op.europa.eu/it/publication-detail/-/publication/27d2db38-76bc-11e9-9f05-01aa75ed71a1. |
| [33] |
H. Egawa, Average length of stay in hospitals, J. UOEH, 6 (1984), 1-14. doi: 10.7888/juoeh.6.1
|
| [34] |
E. Y. Bae, J. M. Hong, H. Y. Kwon, S. Jang, H. J. Lee, S. Bae, et al., Eight-year experience of using HTA in drug reimbursement: South Korea, Health Policy Amst. Neth., 120 (2016), 612-620. doi: 10.1016/j.healthpol.2016.03.013
|
| [35] |
P. K. Tsantoulis, N. G. Kastrinakis, A. D. Tourvas, G. Laskaris, V. G. Gorgoulis, Advances in the biology of oral cancer, Oral Oncol., 43 (2007), 523-534. doi: 10.1016/j.oraloncology.2006.11.010
|
| [36] | B. C. Migueláñez-Medrán, J. J. Pozo-Kreilinger, J. L. Cebrián-Carretero, M. A. Martínez-García, A. F. López-Sánchez, Oral squamous cell carcinoma of tongue: Histological risk assessment. A pilot study, Med. Oral Patol. Oral Cirugia Bucal, 24 (2019), e603-e609. |
| [37] |
M. L. Gillison, A. K. Chaturvedi, W. F. Anderson, C. Fakhry, Epidemiology of human papillomavirus-positive head and neck squamous cell carcinoma, J. Clin. Oncol., 33 (2015), 3235-3242. doi: 10.1200/JCO.2015.61.6995
|
| [38] | C. H. Shiboski, B. L. Schmidt, R. C. K. Jordan, Tongue and tonsil carcinoma: increasing trends in the U.S. population ages 20-44 years, Cancer, 103 (2005), 1843-1849. |
| [39] |
C. G. Gourin, J. T. Johnson, Surgical treatment of squamous cell carcinoma of the base of tongue, Head Neck, 23 (2001), 653-660. doi: 10.1002/hed.1092
|
| [40] |
Y. Kimata, M. Sakuraba, S. Hishinuma, S. Ebihara, R. Hayashi, T. Asakage, et al., Analysis of the relations between the shape of the reconstructed tongue and postoperative functions after subtotal or total glossectomy, The Laryngoscope, 113 (2003), 905-909. doi: 10.1097/00005537-200305000-00024
|
| [41] | V. Cantoni, R. Green, C. Ricciardi, R. Assante, E. Zampella, C. Nappi, et al., A machine learning-based approach to directly compare the diagnostic accuracy of myocardial perfusion imaging by conventional and cadmium-zinc telluride SPECT, J. Nucl. Cardiol., 2020 (2020) 1-10. |
| [42] | T. Mannarino, R. Assante, C. Ricciardi, E. Zampella, C. Nappi, V. Gaudieri, et al., Head-to-head comparison of diagnostic accuracy of stress-only myocardial perfusion imaging with conventional and cadmium-zinc telluride single-photon emission computed tomography in women with suspected coronary artery disease, J. Nucl. Cardiol., 2019 (2019), 1-10. |
| [43] |
M. L. Durand, B. B. Yarlagadda, D. L. Rich, D. T. Lin, K. S. Emerick, J. W. Rocco, et al., The time course and microbiology of surgical site infections after head and neck free flap surgery, The Laryngoscope, 125 (2015), 1084-1089. doi: 10.1002/lary.25038
|
| [44] |
J. T. Johnson, L. Y. Victor, E. N. Myers, R. R. Muder, P. B. Thearle, W. F. Diven, Efficacy of two third-generation cephalosporins in prophylaxis for head and neck surgery, Arch. Otolaryngol., 110 (1984), 224-227. doi: 10.1001/archotol.1984.00800300016003
|
| [45] | A. Świderski, A. Borucka, P. Skoczyński, Characteristics and assessment of the road safety level in Poland with multiple regression model, in Transport Means', Proceedings of the 22nd Interna tional Scientific Conference, Part I, Lithuania, (2018), 92-97. |
| [46] |
R. Jiménez, L. López, D. Dominguez, H. Fariñas, Difference between observed and predicted length of stay as an indicator of inpatient care inefficiency, Int. J. Qual. Health Care J. Int. Soc. Qual. Health Care, 11 (1999), 375-384. doi: 10.1093/intqhc/11.5.375
|
| [47] |
V. K. Omachonu, S. Suthummanon, M. Akcin, S. Asfour, Predicting length of stay for Medicare patients at a teaching hospital, Health Serv. Manage. Res., 17 (2004), 1-12. doi: 10.1258/095148404322772688
|
 mbe-18-04-174-Supplementary.pdf mbe-18-04-174-Supplementary.pdf |
 |
Figures(4) / Tables(9)

Alfonso Maria Ponsiglione, Carlo Ricciardi, Giovanni Improta, Giovanni Dell'Aversana Orabona, Alfonso Sorrentino, Francesco Amato, Maria Romano. A Six Sigma DMAIC methodology as a support tool for Health Technology Assessment of two antibiotics[J]. Mathematical Biosciences and Engineering, 2021, 18(4): 3469-3490. doi: 10.3934/mbe.2021174







 DownLoad:
DownLoad: