Food allergies are adverse reactions to a specific food antigen which is mediated by immunological mechanisms and are fast rising to become a significant public health concern. Around 1% of the world's adult population suffers from food allergies. The prevalence of food allergies which can be life-threatening is commonly estimated to affect 3–5% of the adult population in North America.
The purpose of this study is to review published food allergy knowledge and training amongst food service workers and identify the policies in place concerning food allergies globally.
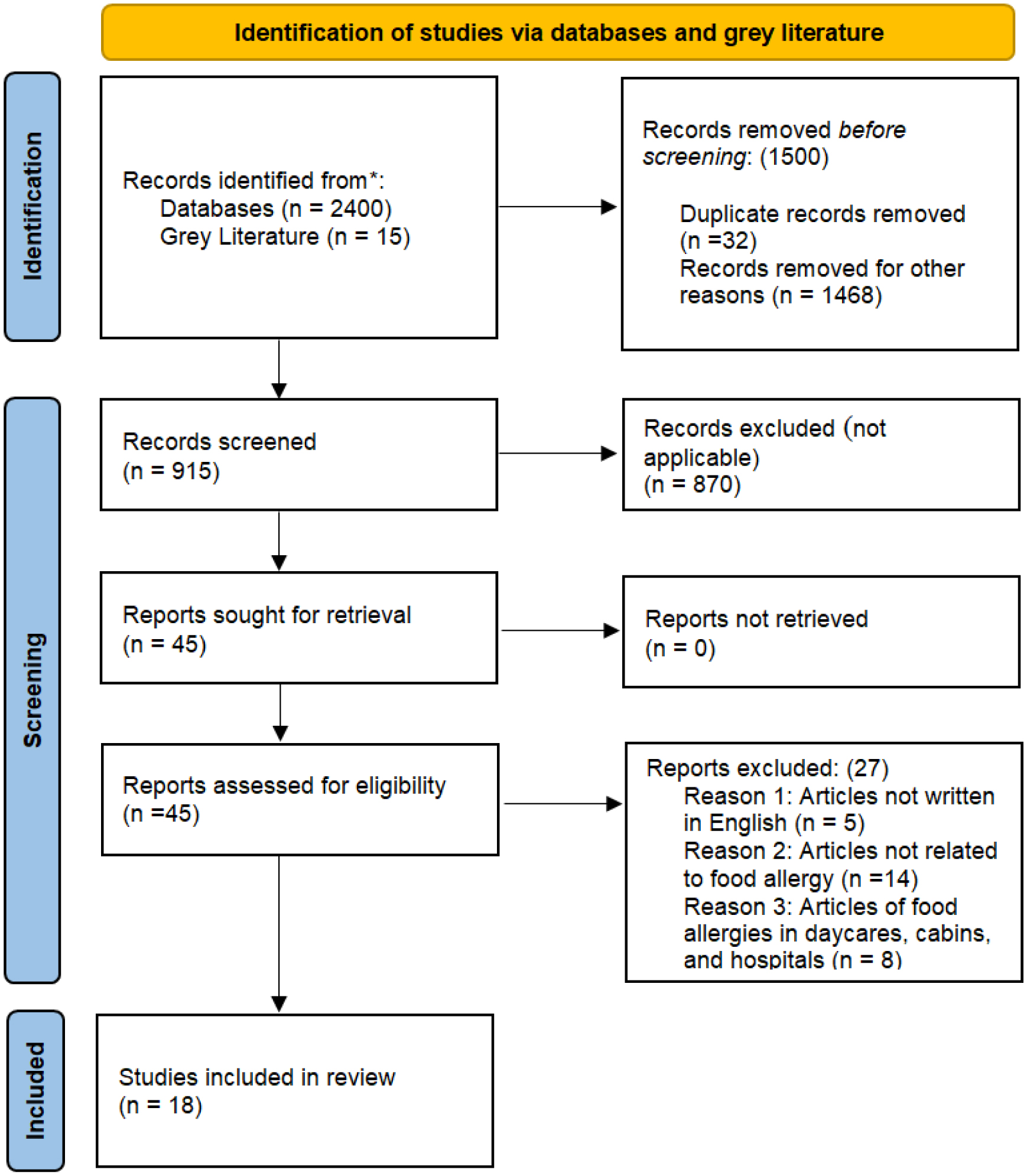
Documented food service workers' knowledge and training about food allergies published between September 2006 and February 2021 were comprehensively reviewed. A widespread literature search was carried out using subject headings, search terms, and keywords. Results were examined in groups to explore patterns through research.
A total of 18 relevant studies that analyzed the food allergies knowledge and training of food service workers were reviewed. Eight studies (44%) were performed in the USA, followed by two studies (11%) in the UK, and one study each (5%) for New Zealand, Turkey, Malaysia, France, Western Romania, Germany, Brazil, and Canada. In the studies, respondents were asked a series of questions to assess their level of knowledge and the types of training relating to food allergies they received.
This study identified the gaps in policy, as well as knowledge and training among food service workers, to manage food allergies safely, thus emphasizing the importance and need for food allergy training.
Citation: Temilorun Ajibade, Cecilia Bukutu, Aleksandra Marinkovic, Chuku Okorie, Ricardo Izurieta, Adekunle Sanyaolu. A systematic review of the knowledge and training of food service workers on food allergies[J]. AIMS Allergy and Immunology, 2023, 7(3): 195-212. doi: 10.3934/Allergy.2023014
Food allergies are adverse reactions to a specific food antigen which is mediated by immunological mechanisms and are fast rising to become a significant public health concern. Around 1% of the world's adult population suffers from food allergies. The prevalence of food allergies which can be life-threatening is commonly estimated to affect 3–5% of the adult population in North America.
The purpose of this study is to review published food allergy knowledge and training amongst food service workers and identify the policies in place concerning food allergies globally.
Documented food service workers' knowledge and training about food allergies published between September 2006 and February 2021 were comprehensively reviewed. A widespread literature search was carried out using subject headings, search terms, and keywords. Results were examined in groups to explore patterns through research.
A total of 18 relevant studies that analyzed the food allergies knowledge and training of food service workers were reviewed. Eight studies (44%) were performed in the USA, followed by two studies (11%) in the UK, and one study each (5%) for New Zealand, Turkey, Malaysia, France, Western Romania, Germany, Brazil, and Canada. In the studies, respondents were asked a series of questions to assess their level of knowledge and the types of training relating to food allergies they received.
This study identified the gaps in policy, as well as knowledge and training among food service workers, to manage food allergies safely, thus emphasizing the importance and need for food allergy training.

| [1] |
Young I, Thaivalappil A (2018) A systematic review and meta-regression of the knowledge, practices, and training of restaurant and food service personnel toward food allergies and celiac disease. PloS One 13: e0203496. https://doi.org/10.1371/journal.pone.0203496 
|
| [2] |
Krewen MS (2014) Food allergies update: facts, bylaw changes, and the importance of training. Environ Health Rev 57: 37-39. https://doi.org/10.5864/d2014-017
|
| [3] | Eisenblätter J, Schumacher G, Hirt M, et al. (2021) How do food businesses provide information on allergens in non-prepacked foods? A cross-sectional survey in Switzerland. Allergo J Int 3: 1-8. https://doi.org/10.1007/s40629-021-00191-5 |
| [4] |
Ajala AR, Cruz AG, Faria J, et al. (2010) Food allergens: Knowledge and practices of food handlers in restaurants. Food Control 21: 1318-1321. https://doi.org/10.1016/j.foodcont.2010.04.002
|
| [5] |
Waserman S, Bégin P, Watson W (2018) IgE-mediated food allergy. Allergy Asthma Clin Immunol 14: 1-11. https://doi.org/10.1186/s13223-018-0284-3
|
| [6] | (2023) Food Allergy CanadaFood Allergy and Anaphylaxis. Food Allergy Canada. Available from: https://foodallergycanada.ca/allergies/peanut/. |
| [7] | (2006) Government of CanadaPaper on the allergen control activities within the Canadian Food Inspection Agency (Cat. No.: H39-649/2002E-IN). Government of Canada. Available from: https://www.canada.ca/en/health-canada/services/food-nutrition/food-safety/food-safety-assessments/assessment-reports/paper-allergen-control-activities-within-canadian-food-inspection-agency.html. |
| [8] |
Waserman S, Watson W (2011) Food allergy. Allergy Asthma Clin Immunol 7: S7. https://doi.org/10.1186/1710-1492-7-S1-S7
|
| [9] | Metcalfe DD, Sampson HA, Simon RA (2011) Food Allergy: Adverse Reactions to Foods and Food Additives. Hoboken: John Wiley & Sons. |
| [10] |
Umasunthar T, Leonardi-Bee J, Hodes M, et al. (2013) Incidence of fatal food anaphylaxis in people with food allergy: a systematic review and meta-analysis. Clin Exp Allergy 43: 1333-1341. https://doi.org/10.1111/cea.12211
|
| [11] |
Conrado AB, Lerodiakonou D, Gowland MH, et al. (2021) Food anaphylaxis in the United Kingdom: analysis of national data, 1998–2018. BMJ 372: n251. https://doi.org/10.1136/bmj.n251
|
| [12] | (2018) USDA Foreign Agricultural ServicesCanada food service—Hotel restaurant institutional 2018 (Report No. CA18060). U.S. Department of Agriculture. Available from: https://apps.fas.usda.gov/newgainapi/api/report/downloadreportbyfilename?filename=Food%20Service%20-%20Hotel%20Restaurant%20Institutional_Ottawa_Canada_2-14-2019.pdf. |
| [13] | Saksena MJ, Okrent AM, Anekwe TD, et al. (2018) America's eating habits: Food away from home (No. 281119). United States Department of Agriculture, Economic Research Service. Available from: https://www.ers.usda.gov/webdocs/publications/90228/eib-196.pdf. |
| [14] |
Auad LI, Ginani VC, Stedefeldt E, et al. (2019) Food safety knowledge, attitudes, and practices of brazilian food truck food handlers. Nutrients 11: 1784. https://doi.org/10.3390/nu11081784
|
| [15] | Zeballos E (2020) Market Segments. U.S. Department of Agriculture. Available from: https://www.ers.usda.gov/topics/food-markets-prices/food-service-industry/market-segments/. |
| [16] |
Lessa K, Lozano M, Esteve MJ, et al. (2016) Food allergy knowledge, attitudes and practices: a pilot study of the general public and food handlers. European J Nutr Food Saf 6: 58-64. https://doi.org/10.9734/EJNFS/2016/20696
|
| [17] |
Xu YS, Kastner M, Harada L, et al. (2014) Anaphylaxis-related deaths in Ontario: a retrospective review of cases from 1986 to 2011. Allergy Asthma Clin Immunol 10: 38. https://doi.org/10.1186/1710-1492-10-38
|
| [18] |
Gupta RS, Warren CM, Smith BM, et al. (2019) Prevalence and severity of food allergies among US adults. JAMA Netw Open 2: e185630. https://doi.org/10.1001/jamanetworkopen.2018.5630
|
| [19] |
Oriel RC, Waqar O, Sharma HP, et al. (2021) Characteristics of food allergic reactions in United States restaurants. J Allergy Clin Immunol Pract 9: 1675-1682. https://doi.org/10.1016/j.jaip.2020.12.018
|
| [20] |
Cherkaoui S, Ben-Shoshan M, Alizadehfar R, et al. (2015) Accidental exposures to peanut in a large cohort of Canadian children with peanut allergy. Clin Transl Allergy 5: 16. https://doi.org/10.1186/s13601-015-0055-x
|
| [21] |
Bailey S, Albardiaz R, Frew AJ, et al. (2011) Restaurant staff's knowledge of anaphylaxis and dietary care of people with allergies. Clin Exp Allergy 41: 713-717. https://doi.org/10.1111/j.1365-2222.2011.03748.x
|
| [22] |
Choi JH, Rajagopal L (2013) Food allergy knowledge, attitudes, practices, and training of foodservice workers at a university foodservice operation in the Midwestern United States. Food Control 31: 474-481. https://doi.org/10.1016/j.foodcont.2012.10.023
|
| [23] |
Lee YM, Sozen E (2016) Food allergy knowledge and training among restaurant employees. Int J Hosp Manag 57: 52-59. https://doi.org/10.1016/j.ijhm.2016.05.004
|
| [24] |
Lee YM, Barker GC (2017) Comparison of food allergy policies and training between Alabama (AL) and national restaurant industry. J Culin Sci Technol 15: 1-16. https://doi.org/10.1080/15428052.2016.1185071
|
| [25] |
Jianu C, Golet I (2019) Food allergies: Knowledge and practice among food service workers operating in Western Romania. J Food Protect 82: 207-216. https://doi.org/10.4315/0362-028X.JFP-18-170
|
| [26] |
Dupuis R, Meisel Z, Grande D, et al. (2016) Food allergy management among restaurant workers in a large US city. Food Control 63: 147-157. https://doi.org/10.1016/j.foodcont.2015.11.026
|
| [27] |
McAdams B, Deng A, MacLaurin T (2018) Food allergy knowledge, attitudes, and resources of restaurant employees. Br Food J 120: 2681-2694. https://doi.org/10.1108/BFJ-01-2018-0028
|
| [28] |
Lee YM, Sozen E (2018) Who knows more about food allergies—restaurant managerial staff or employees?. Br Food J 120: 876-890. https://doi.org/10.1108/BFJ-07-2017-0387
|
| [29] |
Soon JM (2020) ‘Food allergy? Ask before you eat’: Current food allergy training and future training needs in food services. Food Control 112: 107129. https://doi.org/10.1016/j.foodcont.2020.107129
|
| [30] |
Sogut A, Kavut AB, Kartal İ, et al. (2015) Food allergy knowledge and attitude of restaurant personnel in Turkey. Int Forum Allergy Rhinol 5: 157-161. https://doi.org/10.1002/alr.21427
|
| [31] |
Loerbrooks A, Tolksdorf SJ, Wagenmann M, et al. (2019) Food allergy knowledge, attitudes and their determinants among restaurant staff: A cross-sectional study. PloS One 14: e0214625. https://doi.org/10.1371/journal.pone.0214625
|
| [32] |
Shafie AA, Azman AW (2015) Assessment of knowledge, attitude and practice of food allergies among food handlers in the state of Penang, Malaysia. Public Health 129: 1278-1284. https://doi.org/10.1016/j.puhe.2015.03.016
|
| [33] |
Radke TJ, Brown LG, Hoover ER, et al. (2016) Food allergy knowledge and attitudes of restaurant managers and staff: an EHS-Net study. J Food Protect 79: 1588-1598. https://doi.org/10.4315/0362-028X.JFP-16-085
|
| [34] |
Wham CA, Sharma KM (2014) Knowledge of café and restaurant managers to provide a safe meal to food allergic consumers. Nutr Diet 71: 265-269. https://doi.org/10.1111/1747-0080.12104
|
| [35] |
Ahuja R, Sicherer SH (2007) Food allergy management from the perspective of restaurant and food establishment personnel. Ann Allerg Asthma Im 98: 344-348. https://doi.org/10.1016/S1081-1206(10)60880-0
|
| [36] |
Lefèvre S, Abitan L, Goetz C, et al. (2019) Multicenter survey of restaurant staff's knowledge of food allergy in eastern France. Allergo J Int 28: 57-62. https://doi.org/10.1007/s40629-018-0062-2
|
| [37] | Wen H, Kwon J (2016) Food allergy risk communication in restaurants. Food Prot Trends 36: 372-383. |
| [38] |
Rezaei K, Jenab E, Temelli F (2007) Effects of water on enzyme performance with an emphasis on the reactions in supercritical fluids. Crit Rev Biotechnol 27: 183-195. https://doi.org/10.1080/07388550701775901
|
| [39] | (2020) FAREAvoiding cross-contact. Food Allergy Research and Education. Available from: https://www.foodallergy.org/resources/avoiding-cross-contact. |
| [40] |
Arendt SW, Roberts KR, Strohbehn C, et al. (2014) Motivating foodservice employees to follow safe food handling practices: Perspectives from a multigenerational workforce. J Hum Resour Hosp Tour 13: 323-349. https://doi.org/10.1080/15332845.2014.888505
|
| [41] | (2020) FSANZFood allergies. Food Standards Australia and New Zealand. Available from: https://www.foodstandards.gov.au/consumer/foodallergies/Pages/default.aspx. |
| [42] | (2020) Allergen BureauUK Food Standards Authority updates allergen labelling guidance. Allergen Bureau. Available from: http://allergenbureau.net/uk-food-standards-authority-updates-allergen-labelling-guidance/. |
| [43] | (2020) Government of CanadaAllergens and gluten sources labelling. Government of Canada. Available from: https://www.canada.ca/en/health-canada/services/food-allergies-intolerances/avoiding-allergens-food/allergen-labelling.html. |
| [44] |
Pádua I, Moreira A, Moreira P, et al. (2020) Impact of a web-based program to improve food allergy management in schools and restaurants. Pediatr Allergy Immu 31: 851-857. https://doi.org/10.1111/pai.13264
|
| [45] |
Vale SL, Said M, Smith J, et al. (2022) Welcome back Kotter—developing a national allergy strategy for Australia. World Allergy Organ J 15: 100706. https://doi.org/10.1016/j.waojou.2022.100706
|
 allergy-07-03-014-s001.pdf allergy-07-03-014-s001.pdf |
 |
Figures(1) / Tables(6)

Temilorun Ajibade, Cecilia Bukutu, Aleksandra Marinkovic, Chuku Okorie, Ricardo Izurieta, Adekunle Sanyaolu. A systematic review of the knowledge and training of food service workers on food allergies[J]. AIMS Allergy and Immunology, 2023, 7(3): 195-212. doi: 10.3934/Allergy.2023014







 DownLoad:
DownLoad: