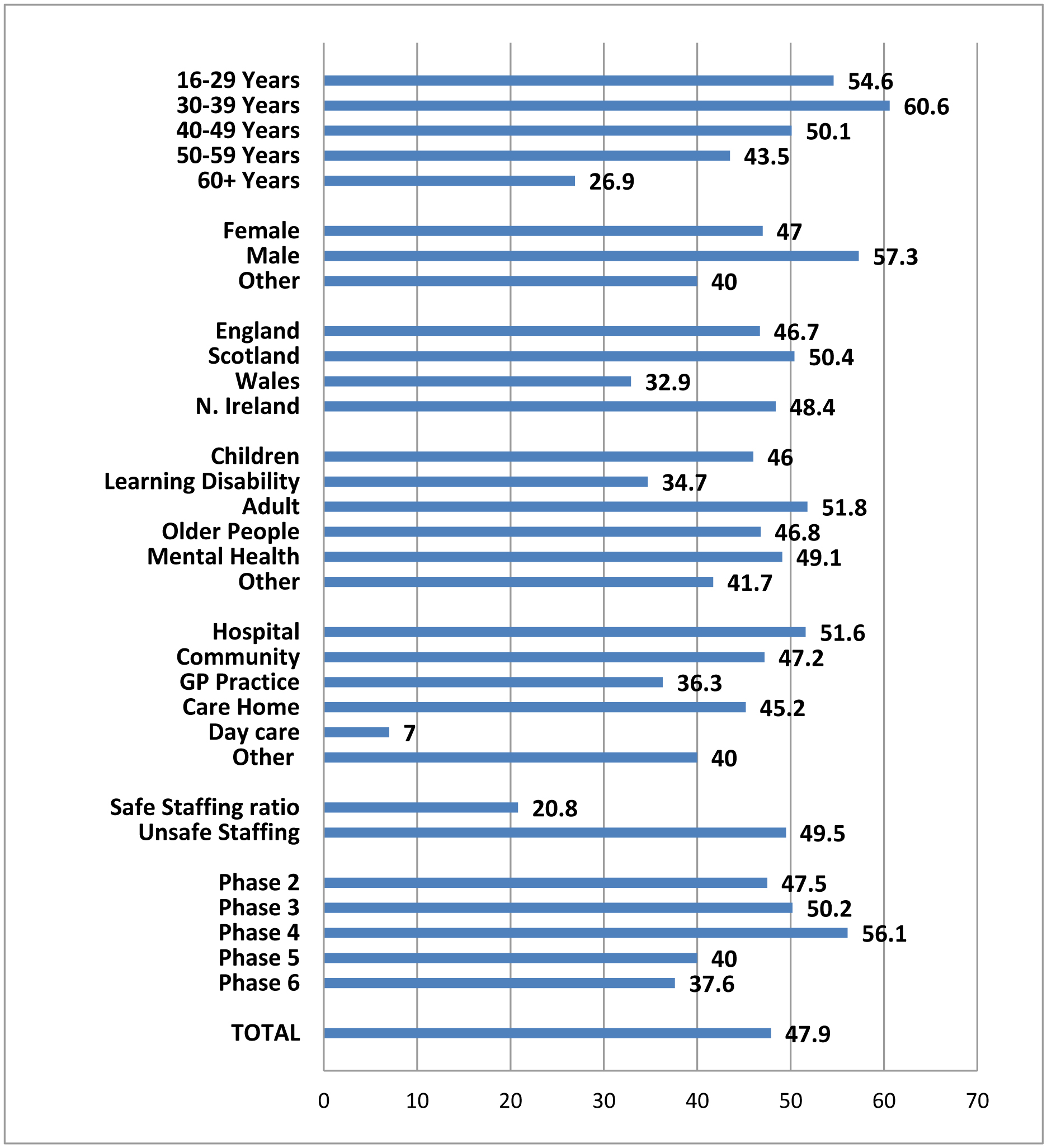
The challenges of maintaining an effective and sustainable healthcare workforce include the recruitment and retention of skilled nurses. COVID-19 exacerbated these challenges, but they persist beyond the pandemic. We explored the impact of work-related quality of life and burnout on reported intentions to leave a variety of healthcare professions including nursing. We collected data at five time-points from November 2020 to February 2023 via an online survey. The validated measures used included the Copenhagen Burnout Inventory and Work-Related Quality of Life (WRQoL) scale; with subscales for Job-Career Satisfaction, General Wellbeing, Control at work, Stress at work, Working conditions, and Home-work interface. Our findings showed that 47.6% of nursing respondents (n = 1780) had considered changing their profession throughout the study period, with the 30–39-year age group most likely to express intentions to leave. Regression analysis reveale that for WRQoL, lower general wellbeing and job-career satisfaction scores predicted intentions to leave when controlling for demographic variables (p < 0.001). When burnout was added to the regression model, both work-related and client-related burnout were predictive of intentions to leave (p < 0.001). These findings highlighted that significant numbers of nurses considered leaving their profession during and shortly after the pandemic and the need for interventions to improve nurses' wellbeing and reduce burnout to improve their retention.
Citation: Susan McGrory, John Mallett, Justin MacLochlainn, Jill Manthorpe, Jermaine Ravalier, Heike Schroder, Denise Currie, Patricia Nicholl, Rachel Naylor, Paula McFadden. The impact of self-reported burnout and work-related quality of life on nurses' intention to leave the profession during the COVID-19 pandemic: A cross-sectional study[J]. AIMS Public Health, 2024, 11(4): 1082-1104. doi: 10.3934/publichealth.2024056
The challenges of maintaining an effective and sustainable healthcare workforce include the recruitment and retention of skilled nurses. COVID-19 exacerbated these challenges, but they persist beyond the pandemic. We explored the impact of work-related quality of life and burnout on reported intentions to leave a variety of healthcare professions including nursing. We collected data at five time-points from November 2020 to February 2023 via an online survey. The validated measures used included the Copenhagen Burnout Inventory and Work-Related Quality of Life (WRQoL) scale; with subscales for Job-Career Satisfaction, General Wellbeing, Control at work, Stress at work, Working conditions, and Home-work interface. Our findings showed that 47.6% of nursing respondents (n = 1780) had considered changing their profession throughout the study period, with the 30–39-year age group most likely to express intentions to leave. Regression analysis reveale that for WRQoL, lower general wellbeing and job-career satisfaction scores predicted intentions to leave when controlling for demographic variables (p < 0.001). When burnout was added to the regression model, both work-related and client-related burnout were predictive of intentions to leave (p < 0.001). These findings highlighted that significant numbers of nurses considered leaving their profession during and shortly after the pandemic and the need for interventions to improve nurses' wellbeing and reduce burnout to improve their retention.

| [1] | International Council of NursesICN international workforce forum calls for urgent action from governments to address global nursing shortage (2019). Available from: https://www.icn.ch/news/icn-international-workforce-forum-calls-urgent-action-governments-address-global-nursing |
| [2] |
Catton H (2021) COVID-19: The future of nursing will determine the fate of our health services. Int Nurs Rev 68: 9-11. https://doi.org/10.1111/inr.12673 
|
| [3] |
Bell M, Sheridan A (2020) How organisational commitment influences nurses' intention to stay in nursing throughout their career. Int J Nurs Stud Adv 2: 100007. https://doi.org/10.1016/j.ijnsa.2020.100007
|
| [4] |
Said RM, El-Shafei DA (2021) Occupational stress, job satisfaction, and intent to leave: nurses working on front lines during COVID-19 pandemic in Zagazig City, Egypt. Environ Sci Pollut Res 28: 8791-8801. https://doi.org/10.1007/s11356-020-11235-8
|
| [5] | Nursing and Midwifery Council2023 NMC Register Leavers Survey (2023). Available from: https://www.nmc.org.uk/globalassets/sitedocuments/data-reports/may-2023/annual-data-report-leavers-survey-2023.pdf |
| [6] | Shembavnekar N, Kelly E (2023) Retaining NHS nurses: What do trends in staff turnover tell us?. USA: The Health Foundation. Available from: https://www.health.org.uk/news-and-comment/charts-and-infographics/retaining-nhs-nurses-what-do-trends-in-staff-turnover-tell-us |
| [7] |
Lo WY, Chien LY, Hwang FM, et al. (2018) From job stress to intention to leave among hospital nurses: A structural equation modelling approach. J Adv Nurs 74: 677-688. https://doi.org/10.1111/jan.13481
|
| [8] | Hasselhorn HM, Müller BH, Tackenberg P, et al. (2005) Nursing in Europe: Intention to leave the nursing profession. NEXT Scientific Report : 17-24. Available from: https://www.researchgate.net/publication/260592268_Next_Scientific_Report_July_2005 |
| [9] |
Duffield CM, Roche MA, Homer C, et al. (2014) A comparative review of nurse turnover rates and costs across countries. J Adv Nurs 70: 2703-2712. https://doi.org/10.1111/jan.12483
|
| [10] |
Falatah R (2021) The impact of the coronavirus disease (COVID-19) pandemic on nurses' turnover intention: An integrative review. Nurs Rep 11: 787-810. https://doi.org/10.3390/nursrep11040075
|
| [11] |
Kaddourah B, Abu-Shaheen AK, Al-Tannir M (2018) Quality of nursing work life and turnover intention among nurses of tertiary care hospitals in Riyadh: A cross-sectional survey. BMC Nurs 17: 43. https://doi.org/10.1186/s12912-018-0312-0
|
| [12] |
Al-Hamdan Z, Nussera H, Masa'deh R (2016) Conflict management style of Jordanian nurse managers and its relationship to staff nurses' intent to stay. J Nurs Manag 22: e137-e145. https://doi.org/10.1111/jonm.12314
|
| [13] | Albougami AS, Almazan JU, Cruz JP, et al. (2020) Factors affecting nurses' intention to leave their current jobs in Saudi Arabia. Int J Health Sci 14: 33-40. |
| [14] |
Sasso L, Bagnasco A, Catania G, et al. (2019) Push and pull factors of nurses' intention to leave. J Nurs Manag 27: 946-954. https://doi.org/10.1111/jonm.12745
|
| [15] | Kantorski LP, Oliveira MMD, Alves PF, et al. (2022) Intention to leave nursing during the COVID-19 pandemic. Rev Lat Am Enfermagem 30: e3613. https://doi.org/10.1590/1518-8345.5815.3549 |
| [16] |
Engström M, Jarnheden SH, Tham P (2023) Staff quality of working life and turnover intentions in municipal nursing care and social welfare: A cross-sectional study. BMC Nurs 22: 171. https://doi.org/10.1186/s12912-023-01339-0
|
| [17] |
Heinen MM, van Achterberg T, Schwendimann R, et al. (2013) Nurses intention to leave their profession: A cross-sectional observational study in 10 European countries. Int J Nurs Stud 50: 174-184. https://doi:10.1016/j.ijnurstu.2012.09.019
|
| [18] |
Raso R, Fitzpatrick JJ, Masick K (2021) Nurses' intent to leave their position and the profession during the COVID-19 pandemic. J Nurs Adm 51: 488-494. https://doi.org/10.1097/NNA.0000000000001052
|
| [19] |
Nantsupawat A, Kunaviktikul W, Nantsupawat R, et al. (2017) Effects of nurse work environment on job dissatisfaction, burnout, intention to leave. Int Nurs Rev 64: 91-98. https://doi.org/10.1111/inr.12342
|
| [20] |
Lavoie-Tremblay M, Gélinas C, Aubé T, et al. (2022) Influence of caring for COVID-19 patients on nurse's turnover, work satisfaction and quality of care. J Nurs Manag 30: 33-43. https://doi.org/10.1111/jonm.13462
|
| [21] |
Aiken LH, Sermeus W, McKee M, et al. (2024) Physician and nurse well-being, patient safety and recommendations for interventions: Cross-sectional survey in hospitals in six European countries. BMJ Open 14: e079931. https://doi.org/10.1136/bmjopen-2023-079931
|
| [22] | Maslach C, Jackson S, Leiter M (1996) Maslach Burnout Inventory Manual. Palo Alto, CA: Consulting Psychologists Press 192. |
| [23] |
Kristensen TS, Borritz M, Villadsen E, et al. (2005) The Copenhagen Burnout Inventory: A new tool for the assessment of burnout. Work Stress 19: 192-207. https://doi.org/10.1080/02678370500297720
|
| [24] | Kelly LA, Gee PM, Butler RJ (2021) Impact of nurse burnout on organizational and position turnover. Nurs Outlook 69: 96102. https://doi.org/10.1016/j.outlook.2020.06.008 |
| [25] |
Meneguin S, Ignácio I, Pollo FC, et al. (2023) Burnout and quality of life in nursing staff during the COVID-19 pandemic. BMC Nurs 22: 14. https://doi.org/10.1186/s12912-022-01168-7
|
| [26] |
Gillen P, Neill RD, Manthorpe J, et al. (2022) Decreasing wellbeing and increasing use of negative coping strategies: The effect of the COVID-19 pandemic on the UK health and social care workforce. Epidemiologia 3: 26-39. https://doi.org/10.3390/epidemiologia3010003
|
| [27] |
Lee MM, Gensimore MM, Maduro RS, et al. (2021) The impact of burnout on emergency nurses' intent to leave: A cross-sectional survey. J Emerg Nurs 47: 892-901. https://doi.org/10.1016/j.jen.2021.07.004
|
| [28] |
Hämmig O (2018) Explaining burnout and the intention to leave the profession among health professionals–a cross-sectional study in a hospital setting in Switzerland. BMC Health Serv Res 18: 785. https://doi.org/10.1186/s12913-018-3556-1
|
| [29] |
Moloney W, Boxall P, Parsons M, et al. (2018) Factors predicting Registered Nurses' intentions to leave their organization and profession: A job demands-resources framework. J Adv Nurs 74: 864-875. https://doi.org/10.1111/jan.13497
|
| [30] |
Labrague LJ, De Los Santos JAA, Falguera CC, et al. (2020) Predictors of nurses' turnover intention at one and five years' time. Int Nurs Rev 67: 191-198. https://doi.org/10.1111/inr.12581
|
| [31] |
Slater P, Roos M, Eskola S, et al. (2021) Challenging and redesigning a new model to explain intention to leave nursing. Scan J Car Sci 35: 626-635. https://doi.org/10.1111/scs.12884
|
| [32] |
Bratt C, Gautun H (2018) Should I stay, or should I go? Nurses' wishes to leave nursing homes and home nursing. J Nurs Manag 26: 1074-1082. https://doi.org/10.1111/jonm.12639
|
| [33] |
Zhang Y, Wu J, Fang Z, et al. (2017) Newly graduated nurses' intention to leave in their first year of practice in Shanghai: A longitudinal study. Nurs Outlook 65: 202-211. https://doi.org/10.1016/j.outlook.2016.10.007
|
| [34] |
Bae SH (2023) Comprehensive assessment of factors contributing to the actual turnover of newly licensed registered nurses working in acute care hospitals: A systematic review. BMC Nurs 22: 31. https://doi.org/10.1186/s12912-023-01190-3
|
| [35] | Flinkman M, Isopahkala-Bouret U, Salanterä S (2013) Young registered nurses' intention to leave the profession and professional turnover in early career: A qualitative case study. ISRN Nurs 2013: e.916061. https://doi.org/10.1155/2013/916061 |
| [36] | Mulud ZA, Mohamad N, Rozi HSZA, et al. (2022) The impacts of stress and resilience on intentions to leave the nursing profession among newly graduated nurses. Proceedings 82: 100. https://doi.org/10.3390/proceedings2022082100 |
| [37] |
Nayak T, Sahoo CK (2015) Quality of work life and organizational performance. J Health Manag 17: 263-273. https://doi.org/10.1177/0972063415589236
|
| [38] |
van Laar D, Edwards JA, Easton S (2007) The work-related quality of life scale for healthcare workers. J Adv Nurs 60: 325-333. https://doi.org/10.1111/j.1365-2648.2007.04409.x
|
| [39] |
Holland P, Tham TL, Sheehan C, et al. (2019) The impact of perceived workload on nurse satisfaction with work-life balance and intention to leave the occupation. App Nurs Res 49: 70-76. https://doi.org/10.1016/j.apnr.2019.06.001
|
| [40] |
Senek M, Robertson S, King R, et al. (2023) Should I stay or should I go? Why nurses are leaving community nursing in the UK. BMC Health Serv Res 23: 164. https://doi.org/10.1186/s12913-023-09163-7
|
| [41] |
Chen YC, Guo YLL, Chin WS, et al. (2019) Patient–nurse ratio is related to nurses' intention to leave their job through mediating factors of burnout and job dissatisfaction. Int J Environ Res Public Health 16: 4801. https://doi.org/10.3390/ijerph16234801
|
| [42] |
Labrague LJ, de Los Santos JAA (2021) Fear of Covid-19, psychological distress, work satisfaction and turnover intention among frontline nurses. J Nurs Manag 29: 395-403. https://doi.org/10.1111/jonm.13168
|
| [43] |
Chegini Z, Asghari Jafarabadi M, Kakemam E (2019) Occupational stress, quality of working life and turnover intention amongst nurses. Nurs Crit Car 24: 283-289. https://doi.org/10.1111/nicc.12419
|
| [44] | Easton S, Van Laar D (2018) User manual for the Work-Related Quality of Life (WRQoL) Scale: A measure of quality of working life. UK: University of Portsmouth 8-67. https://doi.org/10.17029/EASTON2018 |
| [45] |
Creedy DK, Sidebotham M, Gamble J, et al. (2017) Prevalence of burnout, depression, anxiety and stress in Australian midwives: A cross-sectional survey. BMC Pregnancy Childbirth 17: 13. https://doi.org/10.1186/s12884-016-1212-5
|
| [46] |
Guttman L (1954) Some necessary conditions for common factor analysis. Psychometrika 19: 149-161. https://doi.org/10.1007/BF02289162
|
| [47] |
Kaiser HF (1960) The application of electronic computers to factor analysis. Educ Psychol Meas 20: 141-151. https://doi.org/10.1177/001316446002000116
|
| [48] |
Coste J, Bouée S, Ecosse E, et al. (2005) Methodological issues in determining the dimensionality of composite health measures using principal component analysis: Case illustration and suggestions for practice. Qual Life Res 14: 641-654. https://doi.org/10.1007/s11136-004-1260-6
|
| [49] | Osborne JW (2015) Best practices in logistic regression. Los Angeles: Sage 98-99. |
| [50] |
Kim JH (2019) Multicollinearity and misleading statistical results. Korean J Anesthesiology 72: 558-569. https://doi.org/10.4097/kja.19087
|
| [51] |
Taylor LM, Eost-Telling CL, Ellerton A (2019) Exploring preceptorship programmes: Implications for future design. J Clin Nur 28: 1164-1173. https://doi.org/10.1111/jocn.14714
|
| [52] | Nursing and Midwifery CouncilPrinciples of preceptorship (2023). Available from: https://www.nmc.org.uk/standards/guidance/preceptorship/ |
| [53] |
Barrett R (2020) Changing preceptorship to achieve better quality training and less attrition in newly qualified nurses. Brit J Nurs 29: 706-709. https://doi.org/10.12968/bjon.2020.29.12.706
|
| [54] |
Forrest B (2023) Men in nursing; smoke and mirrors. Brit J Nurs 32: 234-234. https://doi.org/10.12968/bjon.2023.32.5.234
|
| [55] | Institute for GovernmentTimeline of UK government coronavirus lockdowns and measures, March 2020 to December 2021 (2022). Available from: https://www.instituteforgovernment.org.uk/data-visualisation/timeline-coronavirus-lockdowns |
| [56] |
Farhadi A, Bagherzadeh R, Moradi A, et al. (2021) The relationship between professional self-concept and work-related quality of life of nurses working in the wards of patients with COVID-19. BMC Nurs 20: 75. https://doi.org/10.1186/s12912-021-00595-2
|
| [57] |
Neill RD, McFadden P, Manthorpe J, et al. (2023) Changing responses during the COVID-19 pandemic: a comparison of psychological wellbeing and work-related quality of life of UK health and social care workers. BioMed 3: 369-386. https://doi.org/10.3390/biomed3030030
|
| [58] |
MacLochlainn J, Manthorpe J, Mallett J, et al. (2023) The COVID-19 pandemic's impact on UK older people's social workers: A mixed-methods study. Brit J Soc Work 53: 3838-3859. https://doi.org/10.1093/bjsw/bcad139
|
| [59] | UK GovtCOVID-19 response: Living with Covid (2022). Available from: https://www.gov.uk/government/publications/covid-19-response-living-with-covid-19/ |
| [60] | National Council of State Boards of NursingNCSBN research projects significant nursing workforce shortages and crisis, 2023 (2023). Available from: https://www.ncsbn.org/news/ncsbn-research-projects-significant-nursing-workforce-shortages-and-crisis |
| [61] |
Poon Y-SR, Lin YP, Griffiths P, et al. (2022) A global overview of healthcare workers' turnover intention amid COVID-19 pandemic: A systematic review with future directions. Hum Resour Health 20: 70. https://doi.org/10.1186/s12960-022-00764-7
|
| [62] | Payne A, Koen L, Niehaus DJH, et al. (2020) Burnout and job satisfaction of nursing staff in a South African acute mental health setting. S Afr J Psychiat 26: 1454. https://doi.org/10.4102/sajpsychiatry.v26i0.1454 |
| [63] |
Al Zamel LG, Lim Abdullah K, Chan CM, et al. (2020) Factors influencing nurses' intention to leave and intention to stay: An integrative review. Home Health Care Manag Prac 32: 218-228. https://doi.org/10.1177/1084822320931363
|
| [64] |
Montgomery AP, Azuero A, Patrician PA (2021) Psychometric properties of Copenhagen Burnout Inventory among nurses. Res Nurs Health 44: 308-318. https://doi.org/10.1002/nur.22114
|
| [65] | RCNValuing nursing in the UK (2023). Available from: https://www.rcn.org.uk/Professional-Development/publications/valuing-nursing-in-the-uk-uk-pub-010-695#:~:text=Despite%20public%20support%20for%20the,to%20leave%20the%20profession%20altogether |
| [66] |
Burmeister EA, Kalisch BJ, Xie B, et al. (2019) Determinants of nurse absenteeism and intent to leave: An international study. J Nurs Manag 27: 143-153. https://doi.org/10.1111/jonm.12659
|
| [67] |
Senek M, Robertson S, Ryan T, et al. (2020) Determinants of nurse job dissatisfaction-findings from a cross-sectional survey analysis in the UK. BMC Nurs 19: 1-10. https://doi.org/10.1186/s12912-020-00481-3
|
| [68] |
Montgomery AP, Azuero A, Baernholdt M, et al. (2021) Nurse burnout predicts self-reported medication administration errors in acute care hospitals. J Healthc Qual 43: 13-23. https://doi.org/10.1097/JHQ.0000000000000274
|
| [69] | Lee YH, Lin MH (2019) Exploring the relationship between burnout and job satisfaction among clinical nurses. Eur Sci J 15: 449-460. http://dx.doi.org/10.19044/esj.2019.v15n3p449 |
| [70] |
Catania G, Zanini M, Cremona MA, et al. (2024) Nurses' intention to leave, nurse workload and in-hospital patient mortality in Italy: A descriptive and regression study. Health Policy 143: 105032. https://doi.org/10.1016/j.healthpol.2024.105032
|
| [71] |
Dall'Ora C, Ball J, Reinius M, et al. (2020) Burnout in nursing: A theoretical review. Hum Resour Health 18: 41. https://doi.org/10.1186/s12960-020-00469-9
|
| [72] | Church E Nursing UCAS applications fall for third year running (2024). Available from: https://www.nursingtimes.net/news/workforce/nursing-ucas-applications-fall-for-third-year-running-15-02-2024/#:~:text=A%20total%20of%2031%2C100%20people,%2C%20and%208%25%20in%20Scotland |
| [73] |
Labrague LJ, Nwafor CE, Tsaras K (2020) Influence of toxic and transformational leadership practices on nurses' job satisfaction, job stress, absenteeism and turnover intention: A cross-sectional study. J Nurs Manag 28: 1104-1113. https://doi.org/10.1111/jonm.13053
|
| [74] |
Gnanapragasam SN, Hodson A, Smith LE, et al. (2021) COVID-19 survey burden for healthcare workers: Literature review and audit. Public Health 206: 94-101. https://doi.org/10.1016/j.puhe.2021.05.006
|
| [75] |
Patel SS, Webster RK, Greenberg N, et al. (2020) Research fatigue in COVID-19 pandemic and post-disaster research: Causes, consequences and recommendations. Disaster Prev Manag Int J 29: 445-455. https://doi.org/10.1108/DPM-05-2020-0164
|
| [76] | Bornstein MH, Jager J, Putnick DL (2013) Sampling in developmental science: Situations, shortcomings, solutions, and standards. Dev Res 33: 357-370. https://doi.org/10.1016/j.dr.2013.08.003 |
| [77] |
Scriven A, Smith-Ferrier S (2003) The application of online surveys for workplace health research. J R Soc Promot Health 123: 95-101. https://doi.org/10.1177/146642400312300213
|
| [78] |
Wise J (2023) Covid-19: WHO declares end of global health emergency. BMJ 381: 1041. https://doi.org/10.1136/bmj.p1041
|
Figures(1) / Tables(8)

Susan McGrory, John Mallett, Justin MacLochlainn, Jill Manthorpe, Jermaine Ravalier, Heike Schroder, Denise Currie, Patricia Nicholl, Rachel Naylor, Paula McFadden. The impact of self-reported burnout and work-related quality of life on nurses' intention to leave the profession during the COVID-19 pandemic: A cross-sectional study[J]. AIMS Public Health, 2024, 11(4): 1082-1104. doi: 10.3934/publichealth.2024056







 DownLoad:
DownLoad: