This paper sheds light on the impact of the COVID-19 pandemic on society and the surrounding environment, with a special focus on education and the social aspect. Specifically, how the pandemic has disrupted education systems across the globe by forcing the closure of primary and secondary schools, colleges and universities is discussed. Since it is not only the students who were affected by this worldwide health emergency, the impact on educators and parents, as well as all aspects of the education system, including admissions, assessments and evaluations, is also debated. These facets are discussed while emphasizing the shifts that many organizations underwent to maintain operations while adhering to the announced governmental restrictions related to the circulation of the pandemic. Specifically, the needs to rapidly implement significant modifications to their usual practices and standard operational processes and convert their existing teaching materials to another format to make them appropriate for online delivery are highlighted and discussed.
Citation: Zaineb Chelly Dagdia, Ana Cristina Simões e Silva. Effects of COVID-19 pandemic on education and society[J]. STEM Education, 2022, 2(3): 197-220. doi: 10.3934/steme.2022013
This paper sheds light on the impact of the COVID-19 pandemic on society and the surrounding environment, with a special focus on education and the social aspect. Specifically, how the pandemic has disrupted education systems across the globe by forcing the closure of primary and secondary schools, colleges and universities is discussed. Since it is not only the students who were affected by this worldwide health emergency, the impact on educators and parents, as well as all aspects of the education system, including admissions, assessments and evaluations, is also debated. These facets are discussed while emphasizing the shifts that many organizations underwent to maintain operations while adhering to the announced governmental restrictions related to the circulation of the pandemic. Specifically, the needs to rapidly implement significant modifications to their usual practices and standard operational processes and convert their existing teaching materials to another format to make them appropriate for online delivery are highlighted and discussed.

| [1] |
Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. The lancet (2020) 395: 497-506. 
|
| [2] |
The COVID-19 pandemic. Critical reviews in clinical laboratory sciences (2020) 57: 365-388.
|
| [3] |
United Nations. End poverty in all its forms everywhere. Retrieved from: https://unstats.un.org/sdgs/report/2021/goal-01/ [Online; accessed 18-March-2022]. |
| [4] |
World Health Organization, World Health Organization best practices for the naming of new human infectious diseases. In: World Health Organization best practices for the naming of new human infectious diseases, 2015. |
| [5] |
World Health Organization, Surveillance case definitions for human infection with novel coronavirus (nCoV), interim guidance, 15 January 2020. |
| [6] |
The proximal origin of SARS-CoV-2. Nature medicine (2020) 26: 450-452.
|
| [7] |
Dr Michel NAHON, Covid-19: mise au point. Retrieved from: https://urgences-serveur.fr/covid-19-mise-au-point.html [Online; accessed 27-January-2022]. |
| [8] |
The biological and clinical significance of emerging SARS-CoV-2 variants. Nature Reviews Genetics (2021) 22: 757-773.
|
| [9] |
The World Health Organization, Tracking sars-cov-2 variants. Retrieved from: https://www.who.int/en/activities/tracking-SARS-CoV-2-variants/ [Online; accessed 27-January-2022]. |
| [10] | The prevalence of symptoms in 24,410 adults infected by the novel coronavirus (SARS-CoV-2; COVID-19): A systematic review and meta-analysis of 148 studies from 9 countries. PloS one (2020) 15: e0234765. |
| [11] | COVID-19: Transmission, prevention, and potential therapeutic opportunities. Clinica chimica acta (2020) 508: 254-266. |
| [12] |
A review of current interventions for COVID-19 prevention. Archives of medical research (2020) 51: 363-374.
|
| [13] | Coronavirus disease (COVID-19) prevention and treatment methods and effective parameters: A systematic literature review. Sustainable cities and society (2021) 64: 102568. |
| [14] | History of the COVID-19 pandemic: Origin, explosion, worldwide spreading. Biochemical and biophysical research communications (2021) 538: 14-23. |
| [15] | Understanding the origin of COVID-19 requires to change the paradigm on zoonotic emergence from the spillover to the circulation model. Infection, Genetics and Evolution (2021) 95: 104812. |
| [16] |
Wuhan seafood market may not be source of novel virus spreading globally. Science (2020) 10: 1126.
|
| [17] |
Dangerous pathogens in the laboratory: from smallpox to today's SARS setbacks and tomorrow's polio-free world. The Lancet (2004) 363: 1566-1568.
|
| [18] |
Do not blame bats and pangolins! Global consequences for wildlife conservation after the SARS-CoV-2 pandemic. Biodiversity and conservation (2020) 29: 3829-3833.
|
| [19] | Guidelines for communicating about bats to prevent persecution in the time of COVID-19. Biological Conservation (2020) 248: 108650. |
| [20] | Probability of a zoonotic spillover with seasonal variation. Infectious Disease Modelling (2021) 6: 514-531. |
| [21] |
Probable pangolin origin of SARS-CoV-2 associated with the COVID-19 outbreak. Current biology (2020) 30: 1346-1351.
|
| [22] | Isolation and characterization of 2019-nCoV-like coronavirus from Malayan pangolins. BioRxiv (2020) . |
| [23] |
Spike protein recognition of mammalian ACE2 predicts the host range and an optimized ACE2 for SARS-CoV-2 infection. Biochemical and biophysical research communications (2020) 526: 165-169.
|
| [24] |
The World Health Organization, Who coronavirus (covid-19) dashboard. Retrieved from: https://covid19.who.int/ [Online; accessed 28-January-2022]. |
| [25] |
Scientific The United Nations Educational and Cultural Organization (UNESCO). Education: From disruption to recovery. Retrieved from: https://en.unesco.org/covid19/educationresponse [Online; accessed 05-February-2022]. |
| [26] | , Impact of COVID-19 pandemic on information management research and practice: Transforming education, work and life. International journal of information management (2020) 55: 102211. |
| [27] | Digitally transforming work styles in an era of infectious disease. International Journal of Information Management (2020) 55: 102172. |
| [28] | Transition to online education in schools during a SARS-CoV-2 coronavirus (COVID-19) pandemic in Georgia. Pedagogical Research (2020) 5:. |
| [29] |
Rethinking assessment in a digital age: Opportunities, challenges and risks. British Educational Research Journal (2016) 42: 454-476.
|
| [30] | Closure of universities due to coronavirus disease 2019 (COVID-19): impact on education and mental health of students and academic staff. Cureus (2020) 12:. |
| [31] |
Scientific The United Nations Educational and Cultural Organization (UNESCO). Unesco rallies international organizations, civil society and private sector partners in a broad coalition to ensure #learningneverstops.[Online; accessed 06-February-2022]. |
| [32] |
Di Pietro, G., Biagi, F., Costa, P., Karpiński, Z. and Mazza. J., The likely impact of COVID-19 on education: Reflections based on the existing literature and recent international datasets, Vol. 30275, Luxembourg: Publications Office of the European Union, 2020. |
| [33] | In the shadow of Coronavirus: Distance education and digital literacy skills in Greece. International Journal of Social Science and Technology (2020) 5: 1-14. |
| [34] | The impact of Covid-19 on learning-the perspective of the Ghanaian student. European Journal of Education Studies (2020) . |
| [35] |
European Migration Network (EMN), the Organisation for Economic Co-operation, and Development (OECD). Inform #2 - impact of covid-19 on international students in eu and oecd member states. Retrieved from: https://ec.europa.eu/migrant-integration/library-document/inform-2-impact-covid-19-international-students-eu-and-oecd-member-states_en [Online; accessed 06-February-2022]. |
| [36] |
THE EUROPEAN PARLIAMENT and THE COUNCIL OF THE EUROPEAN UNION. Directive (eu) 2016/801 of the european parliament and of the council of 11 may 2016 on the conditions of entry and residence of third-country nationals for the purposes of research, studies, training, voluntary service, pupil exchange schemes or educational projects and au pairing. Official Journal of the European Union. |
| [37] |
Should international borders re-open? The impact of travel restrictions on COVID-19 importation risk. BMC public health (2021) 21: 1-9.
|
| [38] | Impact of "e-Learning crack-up" perception on psychological distress among college students during COVID-19 pandemic: A mediating role of "fear of academic year loss". Children and youth services review (2020) 118: 105355. |
| [39] | , Psychological impacts of COVID-19 and satisfaction from online classes: disturbance in daily routine and prevalence of depression, stress, and anxiety among students of Pakistan. Heliyon (2021) 7: e07030. |
| [40] |
Perspective: Mental health and the Covid-19 pandemic. The New England Journal of Medicine (2020) 383: 510-512.
|
| [41] |
Psychological and social impact of COVID-19. Psychological Trauma: Theory, Research, Practice, and Policy (2020) 12: 468-469.
|
| [42] |
Masten, A.S., Narayan, A.J., Silverman, W.K. and Osofsky, J.D., Children in war and disaster. Handbook of child psychology and developmental science, 2015, 1‒42. Wiley. https://doi.org/10.1002/9781118963418.childpsy418 |
| [43] |
American Psychological Association, Keeping your distance to stay safe. Retrieved from: https://www.apa.org/practice/programs/dmhi/research-information/social-distancing |
| [44] |
Economic impact of COVID-19 pandemic in healthcare facilities and systems: International perspectives. Best Practice Research in Clinical Anaesthesiology (2021) 35: 293-306.
|
| [45] |
The economic effects of COVID-19 containment measures. Open Economies Review (2022) 33: 1-32.
|
| [46] | Patient and Hospital Factors Associated With Differences in Mortality Rates Among Black and White US Medicare Beneficiaries Hospitalized With COVID-19 Infection. JAMA Network Open (2021) 4: e2112842. |
| [47] | Ethnic differences in COVID-19 mortality during the first two waves of the Coronavirus Pandemic: a nationwide cohort study of 29 million adults in England. European Journal of Epidemiology (2021) 36: 605-617. |
| [48] | Hospitalization and Mortality among Black Patients and White Patients with Covid-19. New England Journal of Medicine (2020) 382: 2534-2543. |
| [49] | Association of Race With Mortality Among Patients Hospitalized With Coronavirus Disease 2019 (COVID-19) at 92 US Hospitals. JAMA Network Open (2020) 3: e2018039. |
| [50] | The COVID-19 pandemic and health inequalities. Journal of Epidemiology and Community Health (2020) 74: 964-968. |
| [51] |
, Ethnic differences in SARS-CoV-2 infection and COVID-19-related hospitalisation, intensive care unit admission, and death in 17 million adults in England: an observational cohort study using the OpenSAFELY platform. The Lancet (2021) 397: 1711-1724.
|
| [52] | Offline: COVID-19 is not a pandemic. Lancet (2020) 396: 874. |
| [53] |
Syndemics and the biosocial conception of health. The Lancet (2017) 389: 941-950.
|
| [54] |
Multidisciplinary research priorities for the COVID-19 pandemic: a call for action for mental health science. The Lancet Psychiatry (2020) 7: 547-560.
|
| [55] |
, Emotional, behavioral, and psychological impact of the COVID-19 pandemic. Frontiers in Psychology (2020) 11: 566212.
|
| [56] |
LGBTQ populations: Psychologically vulnerable communities in the COVID-19 pandemic. Psychological Trauma (2020) 12: S239-242.
|
| [57] |
The Mental Health Impact of the COVID-19 Pandemic Across Different Cohorts. International Journal of Mental Health and Addiction (2020) 1-7.
|
| [58] |
Patients with mental health disorders in the COVID-19 epidemic. The Lancet Psychiatry (2020) 7: e21.
|
| [59] |
, Remote care for mental health: qualitative study with service users, careers and staff during the COVID-19 pandemic. British Medical Journal Open (2021) 11: e049210.
|
| [60] |
Psychological resilience and post-traumatic growth in disaster-exposed organisations: overview of the literature. British Medical Journal Military Health (2020) 166: 52-56.
|
| [61] |
'Care Under Pressure': a realist review of interventions to tackle doctors' mental ill-health and its impacts on the clinical workforce and patient care. British Medical Journal Open (2018) 8: e021273.
|
| [62] | Occurrence, prevention, and management of the psychological effects of emerging virus outbreaks on healthcare workers: rapid review and meta-analysis. British Medical Journal (2020) 369:. |
| [63] | Experiences of frontline healthcare workers and their views about support during COVID-19 and previous pandemics: a systematic review and qualitative meta-synthesis. BMC Health Services Research (2021) 21: e923. |
| [64] |
Caring for older adults during the COVID-19 pandemic. Clinical Microbiology and Infection (2022) .
|
| [65] | , The effect of age on mortality in patients with Covid-19: a meta-analysis with 611,583 subjects. Journal of the American Medical Directors Association (2020) 21: 915-918. |
| [66] |
, Social disconnectedness, perceived isolation, and symptoms of depression and anxiety among older Americans (NSHAP): a longitudinal mediation analysis. The Lancet Public Health (2020) 5: e62-70.
|
| [67] |
The effect of age, gender, income, work, and physical activity on mental health during coronavirus disease (COVID-19) lockdown in Austria. Journal of Psychosomatic Research (2020) 136: 110186.
|
| [68] | Mental health consequences during the initial stage of the 2020 coronavirus pandemic (COVID-19) in Spain. Brain Behavior and Immunity (2020) 87: 172-176. |
| [69] |
The impact of the COVID-19 pandemic on wellbeing and cognitive functioning of older adults. Scientific Report (2021) 11: 4636.
|
| [70] | A study of older adults' mental health across 33 countries during the COVID-19 pandemic. International Journal of Environmental Research in Public Health (2021) 18: 5090. |
| [71] |
Alcohol use and mental health among older American adults during the early months of the COVID-19 pandemic. International Journal of Environmental Research in Public Health (2021) 18: 4222.
|
| [72] |
How is COVID-19 pandemic impacting mental health of children and adolescents?. International Journal of Disaster Risk Reduction (2020) 51: 10184.
|
| [73] |
Challenges and burden of the Coronavirus 2019 (COVID-19) pandemic for child and adolescent mental health: a narrative review to highlight clinical and research needs in the acute phase and the long return to normality. Child and Adolescent Psychology and Mental Health (2020) 14: 20.
|
| [74] |
, COVID-19 pandemic impact on children and adolescents' mental health: Biological, environmental, and social factors. Progress in Neuro-Psychopharmacology and Biological Psychiatry (2021) 106: 110171.
|
| [75] |
Depression and anxiety among adolescents during COVID-19: a cross-sectional study. Brain Behavior and Immunity (2020) 88: 36-38.
|
| [76] | Promotive factors associated with internalising symptoms amongst college students during the COVID-19 lockdown in Enugu metropolis, Nigeria. South Africa Journal of Psychiatry (2022) 28: 1672. |
| [77] |
Impact of school closures for COVID-19 on the US health-care workforce and net mortality: a modelling study. The Lancet Public Health (2020) 5: e271-e278.
|
| [78] |
, Immediate impact of stay-at-home orders to control COVID-19 transmission on socioeconomic conditions, food insecurity, mental health, and intimate partner violence in Bangladeshi women and their families: An interrupted time series. The Lancet Global Health (2020) 8: e1380-e1389.
|
| [79] |
Domestic violence during the COVID-19 pandemic - Evidence from a systematic review and meta-analysis. Journal of Criminal Justice (2021) 74: 101806.
|
| [80] | Violence against women during the COVID-19 pandemic: An integrative review. International Journal of Gynecology and Obstetric (2020) 151: 180-187. |
| [81] |
Do psychiatric patients experience more psychiatric symptoms during COVID-19 pandemic and lockdown? A case-control study with service and research implications for immunopsychiatry. Brain, Behavior, and Immunity (2020) 87: 100-106.
|
| [82] |
Loneliness as a predictor of outcomes in mental disorders among people who have experienced a mental health crisis: A 4-month prospective study. BMC Psychiatry (2020) 20: 249.
|
| [83] |
Longitudinal analysis of the UK COVID-19 psychological wellbeing study: Trajectories of anxiety, depression and COVID-19-related stress symptomology. Psychiatry Research (2021) 304: 114138.
|






Figures(7) / Tables(4)
Zaineb Chelly Dagdia, Ana Cristina Simões e Silva. Effects of COVID-19 pandemic on education and society[J]. STEM Education, 2022, 2(3): 197-220. doi: 10.3934/steme.2022013

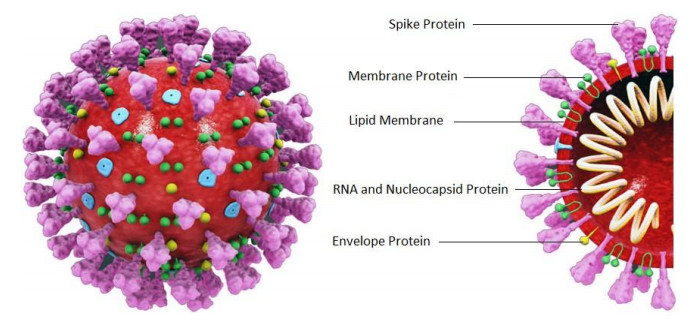
Structure of the SARS-CoV-2 virus. Source: [7]
Categorization of the SARS-CoV-2 variants
Different clusters of the COVID-19 signs and symptoms
Societal, emotional, psychological and behavioral effects of COVID-19 on vulnerable populations. PTSD: post-traumatic stress disorder





 DownLoad:
DownLoad: