Mental health nurses' (MHNs) stigma and discrimination against people with mental illnesses are obstacles to recovery and the development of effective care and treatment. Although many authors have been interested in exploring stigma among general health professionals, paradoxically, less and non-generalizable evidence is available on this phenomenon among MHNs. Understanding the factors associated with stigma and its relationship to recovery attitudes among MHNs could allow for more accurate interventions and improve patient care outcomes.
This study conducted on a sample of Italian psychiatric nurses had the objective of analyzing the aptitude for recovery and the tendency towards stigma of these professionals towards mental illness.
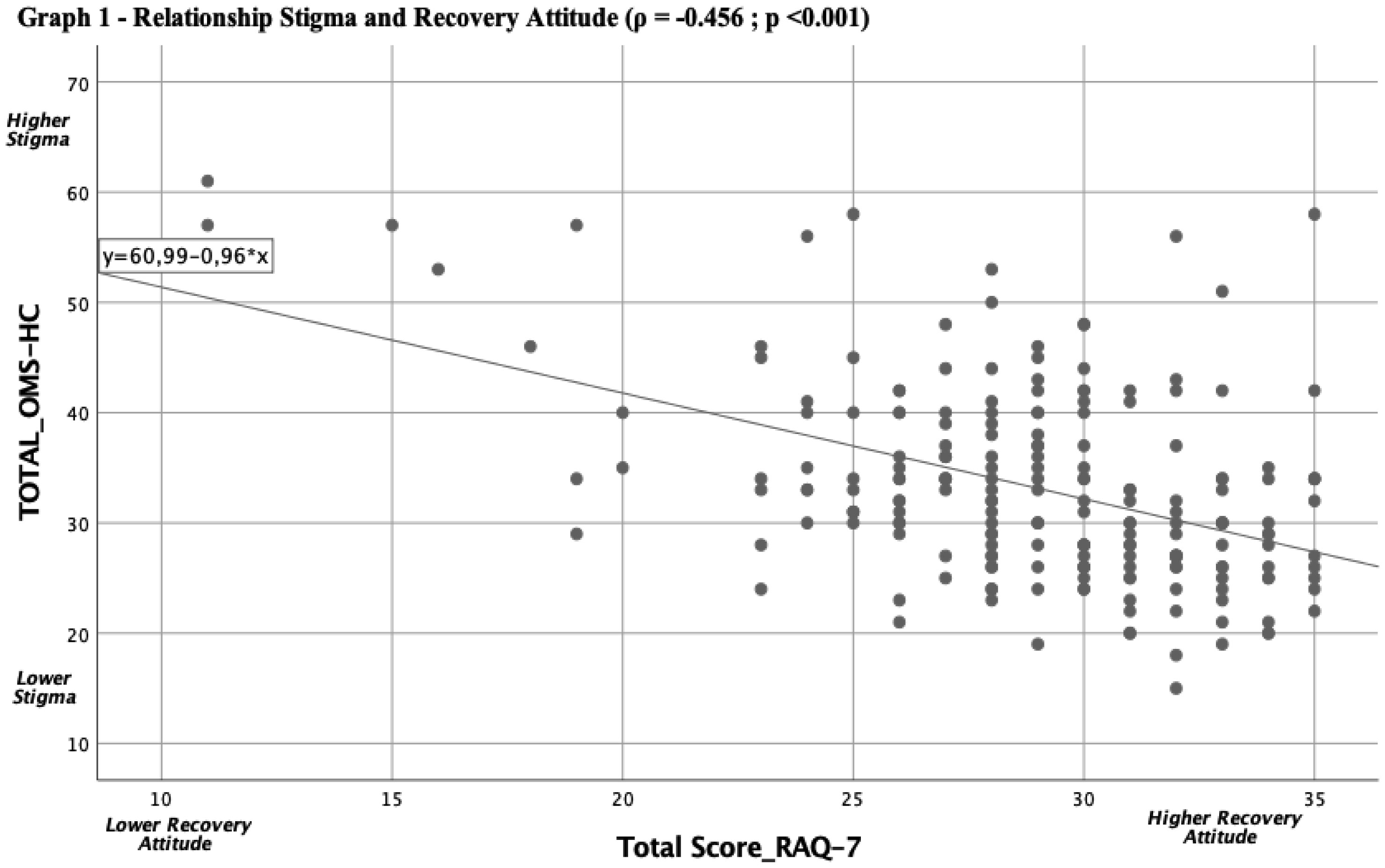
A cross-sectional web survey was conducted on a sample of Italian MHNs, who were administered two validated tools, the RAQ-7 (assessment of recovery aptitude) and the WHO-HC-15 (assessment of stigma) respectively.
A total of 204 MHNs were interviewed. The analysis showed positive overall scores (high recovery aptitude and low stigma levels) among participating MHNs. The attitude to recovery appeared to be directly related to a lower tendency to stigma towards mental illness. It has been observed that MHNs with advanced levels of education appear to be more predisposed to recovery, as well as generally less stigmatizing. There is evidence that the setting in which care is provided, marital status and age can play a significant role in the tendency to stigmatization.
Our manuscript could assist nursing executives, leaders or educators in making decisions about managing and preventing stigma among MHNs.
Citation: Giovanni Napoli, Simone Autuori, Kumi Senkyire Ephraim. Attitudes of Italian mental health nurses towards mental illness and recovery: a cross-sectional study[J]. AIMS Public Health, 2023, 10(2): 333-347. doi: 10.3934/publichealth.2023025
Mental health nurses' (MHNs) stigma and discrimination against people with mental illnesses are obstacles to recovery and the development of effective care and treatment. Although many authors have been interested in exploring stigma among general health professionals, paradoxically, less and non-generalizable evidence is available on this phenomenon among MHNs. Understanding the factors associated with stigma and its relationship to recovery attitudes among MHNs could allow for more accurate interventions and improve patient care outcomes.
This study conducted on a sample of Italian psychiatric nurses had the objective of analyzing the aptitude for recovery and the tendency towards stigma of these professionals towards mental illness.
A cross-sectional web survey was conducted on a sample of Italian MHNs, who were administered two validated tools, the RAQ-7 (assessment of recovery aptitude) and the WHO-HC-15 (assessment of stigma) respectively.
A total of 204 MHNs were interviewed. The analysis showed positive overall scores (high recovery aptitude and low stigma levels) among participating MHNs. The attitude to recovery appeared to be directly related to a lower tendency to stigma towards mental illness. It has been observed that MHNs with advanced levels of education appear to be more predisposed to recovery, as well as generally less stigmatizing. There is evidence that the setting in which care is provided, marital status and age can play a significant role in the tendency to stigmatization.
Our manuscript could assist nursing executives, leaders or educators in making decisions about managing and preventing stigma among MHNs.

| [1] | Vender S, Poloni N, Gambarini S (2005) La stigmatizzazione nella storia e nella cultura. Nòos - Aggiornamenti Psichiatr 11: 149-166. |
| [2] | Goffman E (1963) Stigma: notes on the management of spoiled identity. AM J SOCIOL : 1-4. |
| [3] |
Link BG, Struening EL, Neese Todd S, et al. (2001) Stigma as a barrier to recovery: The consequences of stigma for the self-esteem of people with mental illnesses. Psychiatr Serv Wash DC 52: 1621-1626. https://doi.org/10.1176/appi.ps.52.12.1621 
|
| [4] | Corrigan PW, Watson AC (2002) Understanding the impact of stigma on people with mental illness. World Psychiatry Off J World Psychiatr Assoc WPA 1: 16-20. |
| [5] |
Livingston JD, Boyd JE (2010) Correlates and consequences of internalized stigma for people living with mental illness: a systematic review and meta-analysis. Soc Sci Med 71: 2150-2161. https://doi.org/10.1176/appi.ps.52.12.1621
|
| [6] |
Cavelti M, Kvrgic S, Beck EM, et al. (2012) Self-stigma and its relationship with insight, demoralization, and clinical outcome among people with schizophrenia spectrum disorders. Compr Psychiatry 53: 468-479. https://doi.org/10.1016/j.comppsych.2011.08.001
|
| [7] |
Corrigan PW, Shapiro JR (2010) Measuring the impact of programs that challenge the public stigma of mental illness. Clin Psychol Rev 30: 907-922. https://doi.org/10.1016/j.cpr.2010.06.004
|
| [8] |
Vrbova K, Prasko J, Ociskova M, et al. (2017) Quality of life, self-stigma, and hope in schizophrenia spectrum disorders: A cross-sectional study. Neuropsychiatr Dis Treat 13: 567-576. https://doi.org/10.2147/NDT.S122483
|
| [9] |
Yang LH, Valencia E, Alvarado R, et al. (2013) A theoretical and empirical framework for constructing culture-specific stigma instruments for Chile. Cad Saude Coletiva 21: 71-79. https://doi.org/10.1590/S1414-462X2013000100011
|
| [10] |
Sartorius N (2002) Iatrogenic stigma of mental illness. BMJ 324: 1470-1471. https://doi.org/10.1136/bmj.324.7352.1470
|
| [11] |
Hansson L, Stjernswärd S, Svensson B (2014) Perceived and anticipated discrimination in people with mental illness-an interview study. Nord J Psychiatry 68: 100-106. https://doi.org/10.3109/08039488.2013.775339
|
| [12] | (2016) Ending discrimination against people with mental and substance use disorders: The evidence for stigma change. Washington (DC): National Academies Press(US) 79-91. |
| [13] |
Paykel ES, Tylee A, Wright A, et al. (1997) The defeat depression campaign: psychiatry in the public arena. Am J Psychiatry 154: 59-65. https://doi.org/10.1176/ajp.154.6.59
|
| [14] |
Sreeram A, Cross WM, Townsin L (2022) Anti-stigma initiatives for mental health professionals-a systematic literature review. J Psychiatr Ment Health Nurs 29: 512-528. https://doi.org/10.1111/jpm.12840
|
| [15] |
Angermeyer MC, Breier P, Dietrich S, et al. (2005) Public attitudes toward psychiatric treatment. An international comparison. Soc Psychiatry Psychiatr Epidemiol 40: 855-864. https://doi.org/10.1007/s00127-005-0958-x
|
| [16] |
Angermeyer MC, Dietrich S (2006) Public beliefs about and attitudes towards people with mental illness: a review of population studies. Acta Psychiatr Scand 113: 163-179. https://doi.org/10.1111/j.1600-0447.2005.00699.x
|
| [17] |
Ben Natan M, Drori T, Hochman O (2015) Associative stigma related to psychiatric nursing within the nursing profession. Arch Psychiatr Nurs 29: 388-392. https://doi.org/10.1016/j.apnu.2015.06.010
|
| [18] |
Giandinoto JA, Stephenson J, Edward KL (2018) General hospital health professionals' attitudes and perceived dangerousness towards patients with comorbid mental and physical health conditions: Systematic review and meta-analysis. Int J Ment Health Nurs 27: 942-955. https://doi.org/10.1111/inm.12433
|
| [19] |
Herron J, Ticehurst H, Appleby L, et al. (2001) Attitudes toward suicide prevention in front-line health staff. Suicide Life Threat Behav 31: 342-347. https://doi.org/10.1521/suli.31.3.342.24252
|
| [20] |
Munro S, Baker JA (2007) Surveying the attitudes of acute mental health nurses. J Psychiatr Ment Health Nurs 14: 196-202. https://doi.org/10.1111/j.1365-2850.2007.01063.x
|
| [21] |
Sercu C, Ayala RA, Bracke P (2015) How does stigma influence mental health nursing identities? An ethnographic study of the meaning of stigma for nursing role identities in two Belgian psychiatric hospitals. Int J Nurs Stud 52: 307-316. https://doi.org/10.1016/j.ijnurstu.2014.07.017
|
| [22] |
Nordt C, Rössler W, Lauber C (2006) Attitudes of mental health professionals toward people with schizophrenia and major depression. Schizophr Bull 32: 709-714. https://doi.org/10.1093/schbul/sbj065
|
| [23] |
Ross CA, Goldner EM (2009) Stigma, negative attitudes and discrimination towards mental illness within the nursing profession: a review of the literature. J Psychiatr Ment Health Nurs 16: 558-567. https://doi.org/10.1111/j.1365-2850.2009.01399.x
|
| [24] | Cacioppo M, Tognetti M (2019) L'attivazione dei pazienti con disagio psichico: la mappatura dinamica delle risorse territoriali in una logica di Recovery. Il Mulino-Rivisteweb 1: 127-146. https://doi.org/10.1447/95340 |
| [25] |
Davidson L, Strauss JS (1992) Sense of self in recovery from severe mental illness. Br J Med Psychol 65: 131-145. https://doi.org/10.1111/j.2044-8341.1992.tb01693.x
|
| [26] | Avdibegović E, Hasanović M (2017) The stigma of mental illness and recovery. Psychiatr Danub 29: 900-905. |
| [27] | Davidson L, Rowe M, Tondora J, et al. (2008) A practical guide to recovery-oriented practice: Tools for transforming mental health care. Oxford University Press 1: 1-269. https://doi.org/10.1093/oso/9780195304770.001.0001 |
| [28] | Stull LG, McConnell H, McGrew J, et al. (2017) Explicit and implicit stigma of mental illness as predictors of the recovery attitudes of assertive community treatment practitioners. Isr J Psychiatry Relat Sci 54: 31-37. |
| [29] |
Chambers M, Guise V, Välimäki M, et al. (2010) Nurses' attitudes to mental illness: A comparison of a sample of nurses from five European countries. Int J Nurs Stud 47: 350-362. https://doi.org/10.1016/j.ijnurstu.2009.08.008
|
| [30] |
Halter MJ (2002) Stigma in psychiatric nursing. Perspect Psychiatr Care 38: 23-29. https://doi.org/10.1111/j.1744-6163.2002.tb00652.x
|
| [31] | World Medical Association.Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA (2013) 310: 2191-2194. https://doi.org/10.1001/jama.2013.281053 |
| [32] |
Borkin JR, Steffen JJ, Ensfield LB, et al. (2000) Recovery attitudes questionnaire: Development and evaluation. Psychiatr Rehabil J 24: 95-102. https://doi.org/10.1037/h0095112
|
| [33] |
Modgill G, Patten SB, Knaak S, et al. (2014) Opening minds stigma scale for health care providers (OMS-HC): Examination of psychometric properties and responsiveness. BMC Psychiatry 14: 120. https://doi.org/10.1186/1471-244X-14-120
|
| [34] |
Arvaniti A, Samakouri M, Kalamara E, et al. (2009) Health service staff's attitudes towards patients with mental illness. Soc Psychiatry Psychiatr Epidemiol 44: 658-665. https://doi.org/10.1007/s00127-008-0481-3
|
| [35] |
Babicki M, Kowalski K, Bogudzińska B, et al. (2021) The assessment of attitudes of students at medical schools towards psychiatry and psychiatric patients-a cross-sectional online survey. Int J Environ Res Public Health 18: 4425. https://doi.org/10.3390/ijerph18094425
|
| [36] |
Giralt Palou R, Prat Vigué G, Romeu Labayen M, et al. (2022) Analysis of stigma in relation to behaviour and attitudes towards mental health as influenced by social desirability in nursing students. Int J Environ Res Public Health 19: 3213. https://doi.org/10.3390/ijerph19063213
|
| [37] | Kane CF (2015) The 2014 scope and standards of practice for psychiatric mental health nursing: key updates. Online J Issues Nurs 20: 1. https://doi.org/10.3912/OJIN.Vol20No01Man01 |
| [38] |
Wiesenfeld L, Abbey S, Takahashi SG, et al. (2014) Choosing psychiatry as a career: motivators and deterrents at a critical decision-making juncture. Can J Psychiatry Rev Can Psychiatr 59: 450-454. https://doi.org/10.1177/070674371405900808
|
| [39] |
Winkler P, Csémy L, Janoušková M, et al. (2015) Reported and intended behaviour towards those with mental health problems in the Czech Republic and England. Eur Psychiatry J Assoc Eur Psychiatr 30: 801-806. https://doi.org/10.1016/j.eurpsy.2015.05.003
|
| [40] |
Picco L, Chang S, Abdin E, et al. (2019) Associative stigma among mental health professionals in Singapore: A cross-sectional study. BMJ Open 9: e028179. https://doi.org/10.1136/bmjopen-2018-028179
|
| [41] |
Subu MA, Wati DF, Netrida N, et al. (2021) Types of stigma experienced by patients with mental illness and mental health nurses in Indonesia: A qualitative content analysis. Int J Ment Health Syst 15: 77. https://doi.org/10.1186/s13033-021-00502-x
|
| [42] |
Li J, Li J, Thornicroft G, et al. (2014) Levels of stigma among community mental health staff in Guangzhou, China. BMC Psychiatry 14: 231. https://doi.org/10.1186/s12888-014-0231-x
|
| [43] |
Furnham A, Chan E (2004) Lay theories of schizophrenia. A cross-cultural comparison of British and Hong Kong Chinese attitudes, attributions and beliefs. Soc Psychiatry Psychiatr Epidemiol 39: 543-552. https://doi.org/10.1007/s00127-004-0787-8
|
| [44] |
Shen Y, Dong H, Fan X, et al. (2014) What can the medical education do for eliminating stigma and discrimination associated with mental illness among future doctors? Effect of clerkship training on Chinese students' attitudes. Int J Psychiatry Med 47: 241-254. https://doi.org/10.2190/PM.47.3.e
|
| [45] |
Mather B, Roche M, Duffield C (2014) Disparities in treatment of people with mental disorder in non-psychiatric hospitals: A review of the literature. Arch Psychiatr Nurs 28: 80-86. https://doi.org/10.1016/j.apnu.2013.10.009
|
| [46] |
Björkman T, Angelman T, Jönsson M (2008) Attitudes towards people with mental illness: A cross-sectional study among nursing staff in psychiatric and somatic care. Scand J Caring Sci 22: 170-177. https://doi.org/10.1111/j.1471-6712.2007.00509.x
|
| [47] | Toniolo E, Grossi A (2006) Oltre lo stigma: Strategie di prevenzione in psichiatria. Torino: Centro Scientifico Editore 71-98. |
| [48] | Fernando SM, Deane FP, McLeod HJ (2017) The delaying effect of stigma on mental health help-seeking in Sri Lanka. Asia-Pac Psychiatry Off J Pac Rim Coll Psychiatr 9. https://doi.org/10.1111/appy.12255 |
| [49] | Ewart SB, Bocking J, Happell B, et al. (2016) Mental health consumer experiences and strategies when seeking physical health care: A focus group study. Glob Qual Nurs Res 3: 2333393616631679. https://doi.org/10.1177/2333393616631679 |
| [50] |
Kaufman EA, McDonell MG, Cristofalo MA, et al. (2012) Exploring barriers to primary care for patients with severe mental illness: Frontline patient and provider accounts. Issues Ment Health Nurs 33: 172-180. https://doi.org/10.3109/01612840.2011.638415
|
Figures(1) / Tables(6)

Giovanni Napoli, Simone Autuori, Kumi Senkyire Ephraim. Attitudes of Italian mental health nurses towards mental illness and recovery: a cross-sectional study[J]. AIMS Public Health, 2023, 10(2): 333-347. doi: 10.3934/publichealth.2023025







 DownLoad:
DownLoad: