Children age 5–11 became eligible for COVID-19 vaccination in November 2021 in the United States, but vaccine uptake in this age group remains low. Understanding reasons why parents are hesitant to vaccinate their children may provide critical insights to help protect children from COVID-19 infection. This study examines factors associated with parents' willingness to vaccinate their children.
We conducted a cross-sectional survey focusing on the Los Angeles County adult residents between March and June 2021. Our analytic sample focused on a subgroup of participants who self-report having a child. Predictors included parents' vaccination status and beliefs about COVID-19. We used multivariable logistic regression analysis and calculated the predicted probabilities of parents' willingness to vaccinate their children.
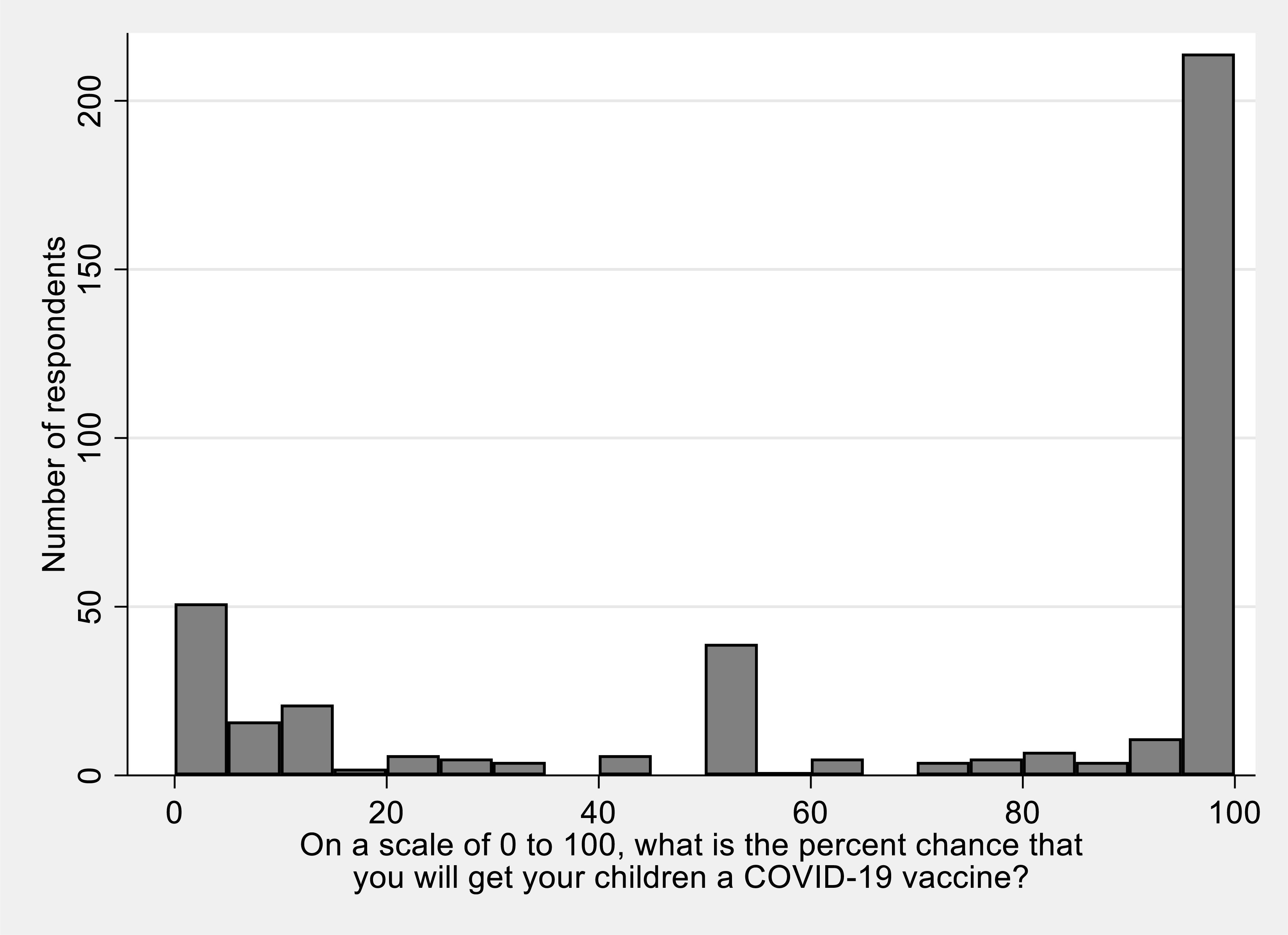
Parents (n = 401) who worried about catching the virus, had trust in vaccine development and the COVID-19 vaccine approval process, and vaccinated against COVID-19 were more likely to be willing to vaccinate their children. Socio-economic, racial and ethnic differences were no longer statistically significant in the adjusted model. Predicted probabilities of parents who were willing to vaccine their children were 55% among the vaccinated and 36% among the unvaccinated.
Parents' intent to vaccinate their children is influenced by their perceived severity of the pandemic, trust in the vaccine development process, and their vaccination status, which can be the potential drivers of hesitancy to vaccinate their children.
Citation: Chun Nok Lam, William Nicholas, Alejandro De La Torre, Yanpui Chan, Jennifer B. Unger, Neeraj Sood, Howard Hu. Factors associated with parents' willingness to vaccinate their children against COVID-19: The LA pandemic surveillance cohort study[J]. AIMS Public Health, 2022, 9(3): 482-489. doi: 10.3934/publichealth.2022033
Children age 5–11 became eligible for COVID-19 vaccination in November 2021 in the United States, but vaccine uptake in this age group remains low. Understanding reasons why parents are hesitant to vaccinate their children may provide critical insights to help protect children from COVID-19 infection. This study examines factors associated with parents' willingness to vaccinate their children.
We conducted a cross-sectional survey focusing on the Los Angeles County adult residents between March and June 2021. Our analytic sample focused on a subgroup of participants who self-report having a child. Predictors included parents' vaccination status and beliefs about COVID-19. We used multivariable logistic regression analysis and calculated the predicted probabilities of parents' willingness to vaccinate their children.
Parents (n = 401) who worried about catching the virus, had trust in vaccine development and the COVID-19 vaccine approval process, and vaccinated against COVID-19 were more likely to be willing to vaccinate their children. Socio-economic, racial and ethnic differences were no longer statistically significant in the adjusted model. Predicted probabilities of parents who were willing to vaccine their children were 55% among the vaccinated and 36% among the unvaccinated.
Parents' intent to vaccinate their children is influenced by their perceived severity of the pandemic, trust in the vaccine development process, and their vaccination status, which can be the potential drivers of hesitancy to vaccinate their children.

| [1] | COVID-19 Vaccinations in LA County. Available from: http://publichealth.lacounty.gov/media/coronavirus/vaccine/vaccine-dashboard.htm |
| [2] | Lopez L, Hamel L, Sparks G, et al. (2021) KFF COVID-19 Vaccine Monitor: Vaccination Trends Among Children And COVID-19 In Schools. Foundation KF : ed2021. |
| [3] |
Sabir DK, Khwarahm NR, Ali SM, et al. (2020) Children protection against COVID-19 at the pandemic outbreak. J Immunol Sci 4: 8-12. https://doi.org/10.29245/2578-3009/2020/2.1188 
|
| [4] | Centers for Disease Control and PreventionScience Brief: Transmission of SARS-CoV-2 in K-12 Schools and Early Care and Education Programs. Available from: https://www.cdc.gov/coronavirus/2019-ncov/science/science-briefs/transmission_k_12_schools.html |
| [5] |
Rhodes ME, Sundstrom B, Ritter E, et al. (2020) Preparing for A COVID-19 vaccine: A mixed methods study of vaccine hesitant parents. J Health Commun 25: 831-837. https://doi.org/10.1080/10810730.2021.1871986
|
| [6] |
Szilagyi PG, Shah MD, Delgado JR, et al. (2021) Parents' intentions and perceptions about COVID-19 vaccination for their children: Results from a national survey. Pediatrics 148: e2021052335. https://doi.org/10.1542/peds.2021-052335
|
| [7] | Davis MM, Zickafoose JS, Halvorson AE, et al. (2020) Parents' likelihood to vaccinate their children and themselves against COVID-19. medRxiv . https://doi.org/10.1101/2020.11.10.20228759 |
| [8] |
Ruggiero KM, Wong J, Sweeney CF, et al. (2021) Parents' intentions to vaccinate their children against COVID-19. J Pediatr Health Care 35: 509-517. https://doi.org/10.1016/j.pedhc.2021.04.005
|
| [9] |
Teasdale CA, Borrell LN, Kimball S, et al. (2021) Plans to vaccinate children for coronavirus disease 2019: a survey of United States parents. J Pediatr 237: 292-297. https://doi.org/10.1016/j.jpeds.2021.07.021
|
| [10] | Lendon JP, Santibanez TA, Singleton JA, et al. Confidence in COVID-19 Vaccination of Children aged 12–17 years old, by Sociodemographic Factors and Adult Respondents' Vaccination Status and Intent—Household Pulse Survey, United States, August 18–September 13, 2021 (2021). Available from: https://www.cdc.gov/vaccines/imz-managers/coverage/covidvaxview/pubs-resources/confidence-covid19-vaccination-children.html |
| [11] |
Sood N, Pernet O, Lam CN, et al. (2022) Seroprevalence of Antibodies Specific to Receptor Binding Domain of SARS-CoV-2 and Vaccination Coverage Among Adults in Los Angeles County, April 2021: The LA Pandemic Surveillance Cohort Study. JAMA Network Open 5: e2144258. https://doi.org/10.1001/jamanetworkopen.2021.44258
|
| [12] |
Gelman A, Pardoe I (2007) Average predictive comparisons for models with nonlinearity, interactions, and variance components. Sociol Methodol 37: 23-51. https://doi.org/10.1111/j.1467-9531.2007.00181.x
|
| [13] |
Dosanjh A (2021) Pediatric vaccine hesitancy and the utilization of antibody measurements: a novel strategy with implications for COVID 19. J Asthma Allergy 14: 427-431. https://doi.org/10.2147/JAA.S303309
|
| [14] | U.S. FOOD & DRUGFDA News Release: Coronavirus (COVID-19) Update: FDA Authorizes Pfizer-BioNTech COVID-19 Vaccine for Emergency Use in Adolescents in Another Important Action in Fight Against Pandemic (2021). Available from: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-pfizer-biontech-covid-19-vaccine-emergency-use |

Figures(2) / Tables(1)

Chun Nok Lam, William Nicholas, Alejandro De La Torre, Yanpui Chan, Jennifer B. Unger, Neeraj Sood, Howard Hu. Factors associated with parents' willingness to vaccinate their children against COVID-19: The LA pandemic surveillance cohort study[J]. AIMS Public Health, 2022, 9(3): 482-489. doi: 10.3934/publichealth.2022033







 DownLoad:
DownLoad: