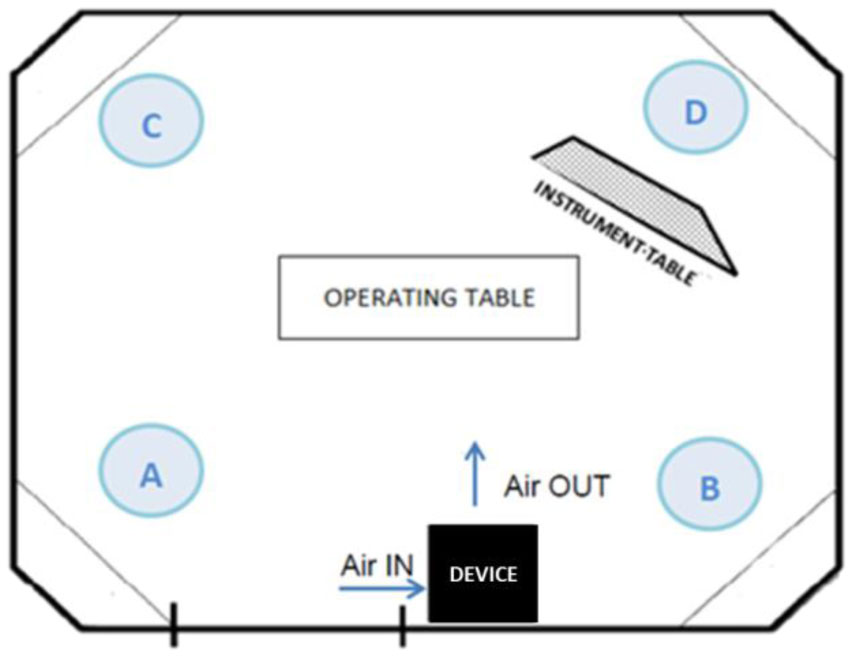
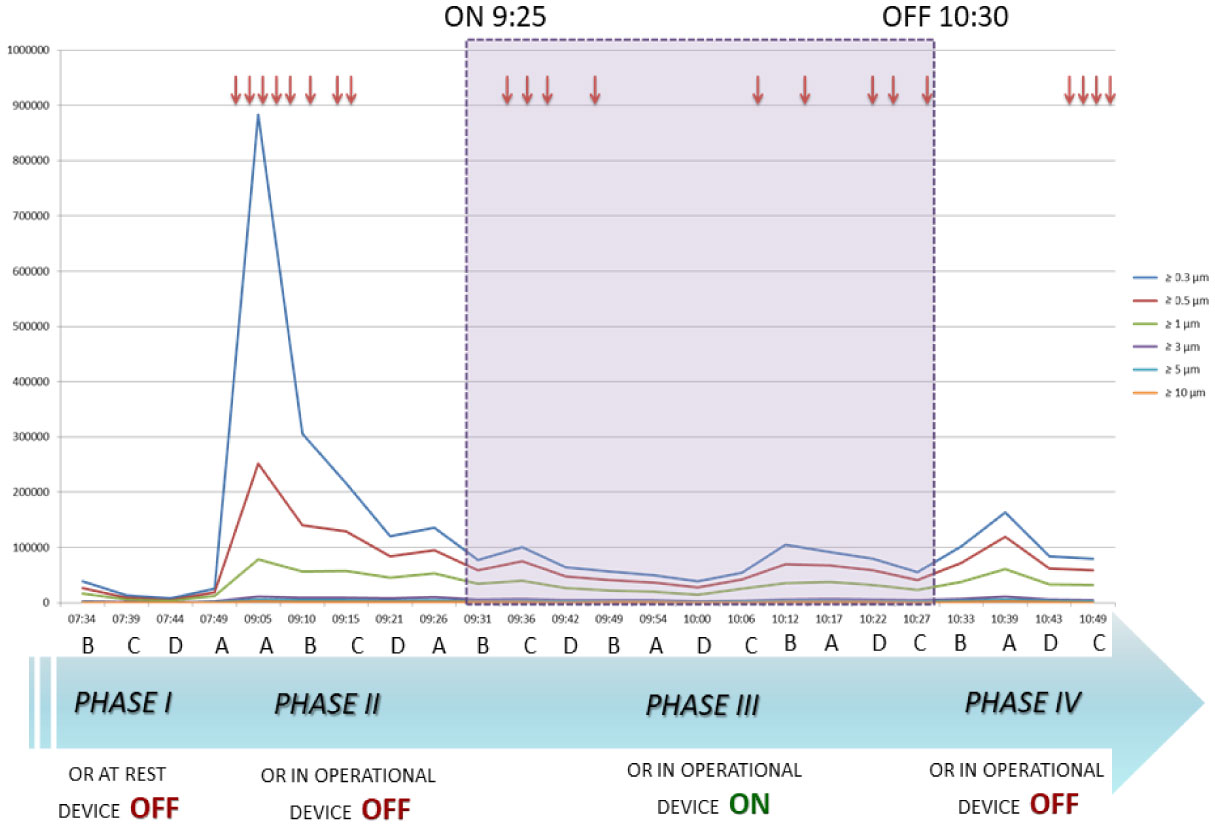
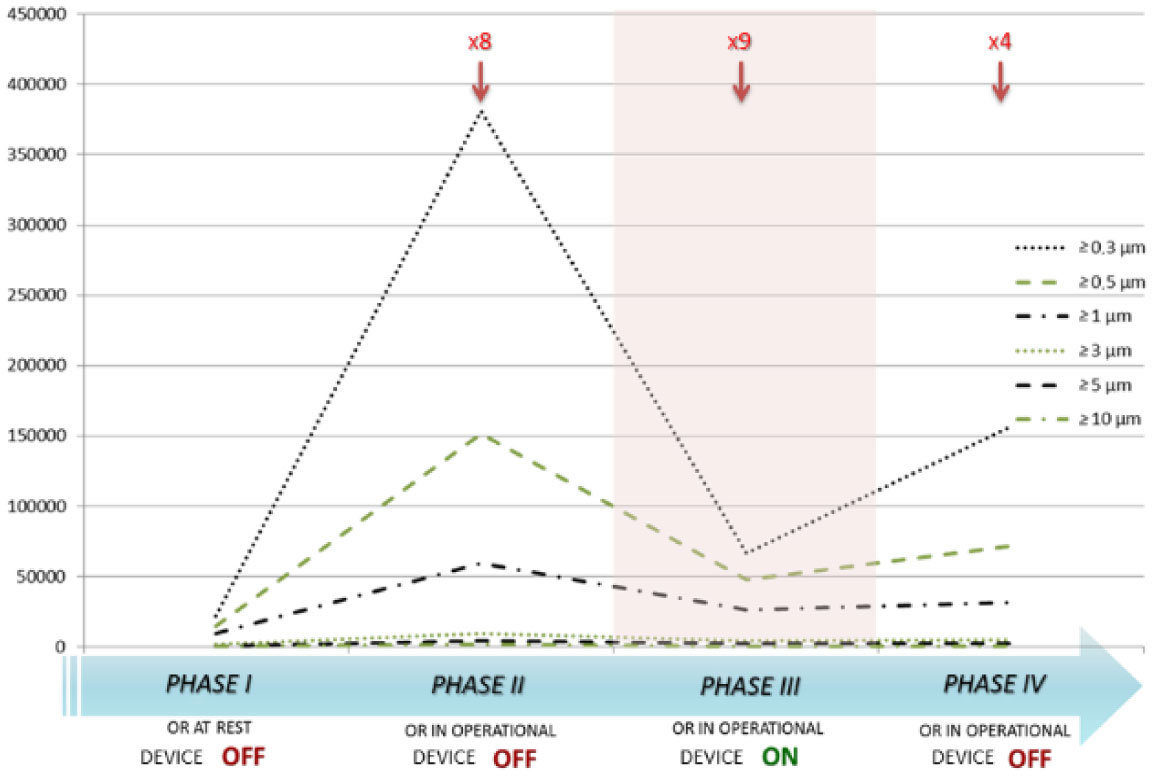
Surgical site infections are the second major cause of hospital acquired infections, accounting for a large part of overall annual medical costs. Airborne particulate is known to be a potential carrier of pathogenic bacteria. We assessed a mobile air particle filter unit for improvement of air quality in an operating room (OR). A new mobile air decontamination and recirculation unit, equipped with a crystalline ultraviolet C (Illuvia® 500 UV) reactor and a HEPA filter, was tested in an OR. Airborne particulate was monitored in four consecutive phases: I) device OFF and OR at rest; II) device OFF and OR in operation; III) device ON and OR in operation; IV) device OFF and OR in operation. We used a particle counter to measure airborne particles of different sizes: ≥0.3, ≥0.5, ≥1, ≥3, ≥5, >10 µm. Activation of the device (phases III) produced a significant reduction (p < 0.05) in airborne particulate of all sizes. Switching the device OFF (phase IV) led to a statistically significant increase (p < 0.05) in the number of particles of most sizes: ≥0.3, ≥0.5, ≥1, ≥3 µm. The device significantly reduced airborne particulate in the OR, improving air quality and possibly lowering the probability of surgical site infections.
Citation: Gabriele Messina, Giuseppe Spataro, Laura Catarsi, Maria Francesca De Marco, Anna Grasso, Gabriele Cevenini. A mobile device reducing airborne particulate can improve air quality[J]. AIMS Public Health, 2020, 7(3): 469-477. doi: 10.3934/publichealth.2020038
Surgical site infections are the second major cause of hospital acquired infections, accounting for a large part of overall annual medical costs. Airborne particulate is known to be a potential carrier of pathogenic bacteria. We assessed a mobile air particle filter unit for improvement of air quality in an operating room (OR). A new mobile air decontamination and recirculation unit, equipped with a crystalline ultraviolet C (Illuvia® 500 UV) reactor and a HEPA filter, was tested in an OR. Airborne particulate was monitored in four consecutive phases: I) device OFF and OR at rest; II) device OFF and OR in operation; III) device ON and OR in operation; IV) device OFF and OR in operation. We used a particle counter to measure airborne particles of different sizes: ≥0.3, ≥0.5, ≥1, ≥3, ≥5, >10 µm. Activation of the device (phases III) produced a significant reduction (p < 0.05) in airborne particulate of all sizes. Switching the device OFF (phase IV) led to a statistically significant increase (p < 0.05) in the number of particles of most sizes: ≥0.3, ≥0.5, ≥1, ≥3 µm. The device significantly reduced airborne particulate in the OR, improving air quality and possibly lowering the probability of surgical site infections.

| [1] | (2013) European Centre for Disease Prevention and ControlSurveillance of surgical site infections in Europe 2010–2011. Stockholm: ECDC. |
| [2] |
Horan TC, Gaynes RP, Martone WJ, et al. (1992) CDC definitions of nosocomial surgical site infections, 1992: a modification of CDC definitions of surgical wound infections. Infect Control Hosp Epidemiol 13: 606-608. doi: 10.2307/30148464

|
| [3] |
Roy MC, Perl TM (1997) Basics of surgical-site infection surveillance. Infect Control Hosp Epidemiol 18: 659-668. doi: 10.2307/30141496
|
| [4] |
Sadrizadeh S, Pantelic J, Sherman M, et al. (2018) Airborne particle dispersion to an operating room environment during sliding and hinged door opening. J Infect Public Health 11: 631-635. doi: 10.1016/j.jiph.2018.02.007
|
| [5] |
Anderson DJ, Kaye KS (2009) Staphylococcal surgical site infections. Infect Dis Clin North Am 23: 53-72. doi: 10.1016/j.idc.2008.10.004
|
| [6] |
Zimlichman E, Henderson D, Tamir O, et al. (2013) Health care-associated infections: a meta-analysis of costs and financial impact on the US health care system. JAMA Intern Med 173: 2039-2046. doi: 10.1001/jamainternmed.2013.9763
|
| [7] |
O'Keeffe AB, Lawrence T, Bojanic S (2012) Oxford craniotomy infections database: a cost analysis of craniotomy infection. Br J Neurosurg 26: 265-269. doi: 10.3109/02688697.2011.626878
|
| [8] |
Badia JM, Casey AL, Petrosillo N, et al. (2017) Impact of surgical site infection on healthcare costs and patient outcomes: a systematic review in six European countries. J Hosp Infect 96: 1-15. doi: 10.1016/j.jhin.2017.03.004
|
| [9] |
Pinkney TD, Calvert M, Bartlett DC, et al. (2013) Impact of wound edge protection devices on surgical site infection after laparotomy: multicentre randomised controlled trial (ROSSINI Trial). BMJ 347: f4305. doi: 10.1136/bmj.f4305
|
| [10] |
Birgand G, Toupet G, Rukly S, et al. (2015) Air contamination for predicting wound contamination in clean surgery: A large multicenter study. Am J Infect Control 43: 516-521. doi: 10.1016/j.ajic.2015.01.026
|
| [11] | Kowalski W (2007) Air-treatment systems for controlling hospital acquired infections. HPAC Eng 79: 24-48. |
| [12] |
Schaal KP (1991) Medical and microbiological problems arising from airborne infection in hospitals. J Hosp Infect 18: 451-459. doi: 10.1016/0195-6701(91)90056-E
|
| [13] |
Edmiston CE, Seabrook GR, Cambria RA, et al. (2005) Molecular epidemiology of microbial contamination in the operating room environment: Is there a risk for infection? Surgery 138: 573-582. doi: 10.1016/j.surg.2005.06.045
|
| [14] |
Seal DV, Clark RP (1990) Electronic particle counting for evaluating the quality of air in operating theatres: a potential basis for standards? J Appl Bacteriol 68: 225-230. doi: 10.1111/j.1365-2672.1990.tb02568.x
|
| [15] |
Vonci N, De Marco MF, Grasso A, et al. (2019) Association between air changes and airborne microbial contamination in operating rooms. J Infect Public Health 12: 827-830. doi: 10.1016/j.jiph.2019.05.010
|
| [16] |
Gormley T, Markel TA, Jones H, et al. (2017) Cost-benefit analysis of different air change rates in an operating room environment. Am J Infect Control 45: 1318-1323. doi: 10.1016/j.ajic.2017.07.024
|
| [17] |
Scaltriti S, Cencetti S, Rovesti S, et al. (2007) Risk factors for particulate and microbial contamination of air in operating theatres. J Hosp Infect 66: 320-326. doi: 10.1016/j.jhin.2007.05.019
|
| [18] |
Anis HK, Curtis GL, Klika AK, et al. (2020) In-Room Ultraviolet Air Filtration Units Reduce Airborne Particles During Total Joint Arthroplasty. J Orthop Res 38: 431-437. doi: 10.1002/jor.24453
|
| [19] |
Curtis GL, Faour M, Jawad M, et al. (2018) Reduction of Particles in the Operating Room Using Ultraviolet Air Disinfection and Recirculation Units. J Arthroplasty 33: S196-S200. doi: 10.1016/j.arth.2017.11.052
|
| [20] |
Anderson DJ, Podgorny K, Berrios-Torres SI, et al. (2014) Strategies to prevent surgical site infections in acute care hospitals: 2014 update. Infect Control Hosp Epidemiol 35: S66-S88. doi: 10.1017/S0899823X00193869
|
| [21] |
Ban KA, Minei JP, Laronga C, et al. (2017) American College of Surgeons and Surgical Infection Society: Surgical Site Infection Guidelines, 2016 Update. J Am Coll Surg 224: 59-74. doi: 10.1016/j.jamcollsurg.2016.10.029
|
| [22] |
Magill SS, Edwards JR, Bamberg W, et al. (2014) Multistate point-prevalence survey of health care-associated infections. N Engl J Med 370: 1198-1208. doi: 10.1056/NEJMoa1306801
|
| [23] | (2018) OECDiLibraryStemming the Superbug Tide: Just A Few Dollars More. Paris: OECD Publishing. Available from: https://www.oecd-ilibrary.org/social-issues-migration-health/stemming-the-superbug-tide_9789264307599-en. |
Figures(3) / Tables(1)

Gabriele Messina, Giuseppe Spataro, Laura Catarsi, Maria Francesca De Marco, Anna Grasso, Gabriele Cevenini. A mobile device reducing airborne particulate can improve air quality[J]. AIMS Public Health, 2020, 7(3): 469-477. doi: 10.3934/publichealth.2020038







 DownLoad:
DownLoad: