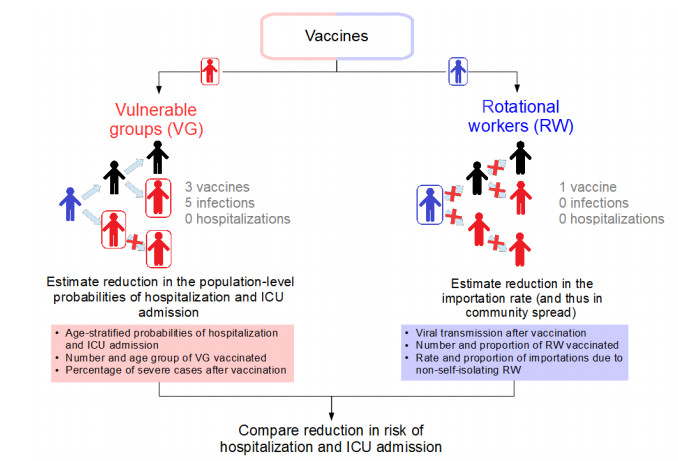
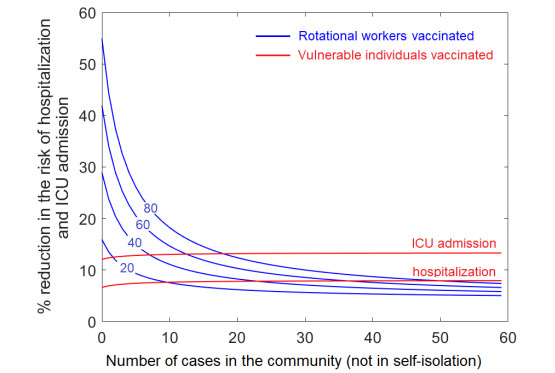
As COVID-19 vaccines become available, different model-based approaches have been developed to evaluate strategic priorities for vaccine allocation to reduce severe illness. One strategy is to directly prioritize groups that are likely to experience medical complications due to COVID-19, such as older adults. A second strategy is to limit community spread by reducing importations, for example by vaccinating members of the mobile labour force, such as rotational workers. This second strategy may be appropriate for regions with low disease prevalence, where importations are a substantial fraction of all cases and reducing the importation rate reduces the risk of community outbreaks, which can provide significant indirect protection for vulnerable individuals. Current studies have focused on comparing vaccination strategies in the absence of importations, and have not considered allocating vaccines to reduce the importation rate. Here, we provide an analytical criteria to compare the reduction in the risk of hospitalization and intensive care unit (ICU) admission over four months when either older adults or rotational workers are prioritized for vaccination. Vaccinating rotational workers (assumed to be 6,000 individuals and about 1% of the Newfoundland and Labrador (NL) population) could reduce the average risk of hospitalization and ICU admission by 42%, if no community spread is observed at the time of vaccination, because epidemic spread is reduced and vulnerable individuals are indirectly protected. In contrast, vaccinating all individuals aged 75 and older (about 43,300 individuals, or 8% of the NL population) would lead to a 24% reduction in the average risk of hospitalization, and to a 45% reduction in the average risk of ICU admission, because a large number of individuals at high risk from COVID-19 are now vaccinated. Therefore, reducing the risk of hospitalization and ICU admission of the susceptible population by reducing case importations would require a significantly lower number of vaccines. Benefits of vaccinating rotational workers decrease with increasing infection prevalence in the community. Prioritizing members of the mobile labour force should be considered as an efficient strategy to indirectly protect vulnerable groups from COVID-19 exposure in regions with low disease prevalence.
Citation: Maria M. Martignoni, Proton Rahman, Amy Hurford. Rotational worker vaccination provides indirect protection to vulnerable groups in regions with low COVID-19 prevalence[J]. AIMS Mathematics, 2022, 7(3): 3988-4003. doi: 10.3934/math.2022220
As COVID-19 vaccines become available, different model-based approaches have been developed to evaluate strategic priorities for vaccine allocation to reduce severe illness. One strategy is to directly prioritize groups that are likely to experience medical complications due to COVID-19, such as older adults. A second strategy is to limit community spread by reducing importations, for example by vaccinating members of the mobile labour force, such as rotational workers. This second strategy may be appropriate for regions with low disease prevalence, where importations are a substantial fraction of all cases and reducing the importation rate reduces the risk of community outbreaks, which can provide significant indirect protection for vulnerable individuals. Current studies have focused on comparing vaccination strategies in the absence of importations, and have not considered allocating vaccines to reduce the importation rate. Here, we provide an analytical criteria to compare the reduction in the risk of hospitalization and intensive care unit (ICU) admission over four months when either older adults or rotational workers are prioritized for vaccination. Vaccinating rotational workers (assumed to be 6,000 individuals and about 1% of the Newfoundland and Labrador (NL) population) could reduce the average risk of hospitalization and ICU admission by 42%, if no community spread is observed at the time of vaccination, because epidemic spread is reduced and vulnerable individuals are indirectly protected. In contrast, vaccinating all individuals aged 75 and older (about 43,300 individuals, or 8% of the NL population) would lead to a 24% reduction in the average risk of hospitalization, and to a 45% reduction in the average risk of ICU admission, because a large number of individuals at high risk from COVID-19 are now vaccinated. Therefore, reducing the risk of hospitalization and ICU admission of the susceptible population by reducing case importations would require a significantly lower number of vaccines. Benefits of vaccinating rotational workers decrease with increasing infection prevalence in the community. Prioritizing members of the mobile labour force should be considered as an efficient strategy to indirectly protect vulnerable groups from COVID-19 exposure in regions with low disease prevalence.

| [1] |
J. Arino, N. Bajeux, S. Portet, J. Watmough, Assessing the risk of COVID-19 importation and the effect of quarantine, medRxiv, 2020. https://doi.org/10.1101/2020.08.12.20173658 doi: 10.1101/2020.08.12.20173658

|
| [2] |
J. H. Buckner, G. Chowell, M. R. Springborn, Optimal dynamic prioritization of scarce COVID-19 vaccines, medRxiv, 2020. https://doi.org/10.1101/2020.09.22.20199174 doi: 10.1101/2020.09.22.20199174
|
| [3] |
A. Babus, S. Das, S. Lee, The optimal allocation of COVID-19 vaccines, medRxiv, 2020. https://doi.org/10.1101/2020.07.22.20160143 doi: 10.1101/2020.07.22.20160143
|
| [4] |
K. M. Bubar, K. Reinholt, S. M. Kissler, M. Lipsitch, S. Cobey, Y. H. Grad, et al., Model-informed COVID-19 vaccine prioritization strategies by age and serostatus, Science, 371 (2021), 916-921. https://doi.org/10.1126/science.abe6959 doi: 10.1126/science.abe6959
|
| [5] |
I. Berry, J.-P. R. Soucy, A. Tuite, D. Fisman, Open access epidemiologic data and an interactive dashboard to monitor the COVID-19 outbreak in Canada, CMAJ, 192 (2020), E420-E420. https://doi.org/10.1503/cmaj.75262 doi: 10.1503/cmaj.75262
|
| [6] | J. Corum, D. Grady, S.-L. Wee, C Zimmer, Coronavirus vaccine tracker, The New York Times, 5 (2020). |
| [7] |
J. Chen, S. Hoops, A. Marathe, H. Mortveit, B. Lewis, S. Venkatramanan, et al., Prioritizing allocation of COVID-19 vaccines based on social contacts increases vaccination effectiveness, medRxiv, 2021. https://doi.org/10.1101/2021.02.04.21251012 doi: 10.1101/2021.02.04.21251012
|
| [8] | Z. Du, L. Wang, B. Yang, Sh. T. Ali, T. K. Tsang, et al., International risk of the new variant COVID-19 importations originating in the United, Science, 371 (2021), 9-10. |
| [9] | N. M. Ferguson, D. Laydon, G. Nedjati-Gilani, N. Imai, K. Ainslie, M. Baguelin, et al., Impact of non-pharmaceutical interventions (NPIs) to reduce COVID-19 mortality and healthcare demand. Imperial College COVID-19 Response Team, Imperial College COVID-19 Response Team, page 20, 2020. |
| [10] | A. Giubilini, The ethics of vaccination, Springer Nature, 2019. https://doi.org/10.1007/978-3-030-02068-2 |
| [11] | GovNL, Definition of rotational worker, 2021. Available from: https://www.gov.nl.ca/covid-19/self-isolation/rotational-workers. |
| [12] | C. M. Hewitt, M. Haan, B. Neis, Interprovincial employees from Newfoundland and Labrador, 2005-2014, 2018. |
| [13] |
A. Hurford, P. Rahman, J. Concepción Loredo-Osti, Modelling the impact of travel restrictions on COVID-19 cases in Newfoundland and Labrador, Roy. Soc. Open Sci., 8 (2021), 202266. https://doi.org/10.1098/rsos.202266 doi: 10.1098/rsos.202266
|
| [14] | A. Hurford, J. Watmough, Don't wait, re-escalate: delayed action results in longer duration of COVID-19 restrictions, medRxiv, pages 2020-11, 2021. https://doi.org/10.1101/2020.11.04.20226316 |
| [15] |
P. Jentsch, M. Anand, C. T. Bauch, Prioritising COVID-19 vaccination in changing social and epidemiological landscapes, medRxiv, 2020. https://doi.org/10.1101/2020.09.25.20201889 doi: 10.1101/2020.09.25.20201889
|
| [16] |
A. Kronbichler, D. Kresse, S. Yoon, K. H. Lee, M. Effenberger, J. I. Shin, Asymptomatic patients as a source of COVID-19 infections: A systematic review and meta-analysis, Int. J. Infect. Dis., 98 (2020), 180-186. https://doi.org/10.1016/j.ijid.2020.06.052 doi: 10.1016/j.ijid.2020.06.052
|
| [17] |
W. O. Kermack, A. G. McKendrick, A contribution to the mathematical theory of epidemics, Proceedings of the Royal Society of London, Series A, 115 (1927), 700-721. https://doi.org/10.1098/rspa.1927.0118 doi: 10.1098/rspa.1927.0118
|
| [18] |
M. D. Knoll, C Wonodi, Oxford-AstraZeneca COVID-19 vaccine efficacy, The Lancet, 397 (2021), 72-74. https://doi.org/10.1016/S0140-6736(20)32623-4 doi: 10.1016/S0140-6736(20)32623-4
|
| [19] |
L. F. Lopez, M. Amaku, F. A. B. Coutinho, M. Quam, M. N. Burattini, C. J. Struchiner, et al., Modeling importations and exportations of infectious diseases via travelers, B. Math. Biol., 78 (2016), 185-209. https://doi.org/10.1007/s11538-015-0135-z doi: 10.1007/s11538-015-0135-z
|
| [20] |
M. K. Lemke, Commercial truck drivers should be a priority population for COVID-19 vaccinations, Am. J. Ind. Med., 64 (2021), 217-219. https://doi.org/10.1002/ajim.23220 doi: 10.1002/ajim.23220
|
| [21] |
N. Mulberry, P. Tupper, E. Kirwin, C. McCabe, C. Colijn, Vaccine rollout strategies: The case for vaccinating essential workers early, medRxiv, 2021. https://doi.org/10.1101/2021.02.23.21252309 doi: 10.1101/2021.02.23.21252309
|
| [22] | NHS, Who's at higher risk from coronavirus, 2021. Available from: https://www.nhs.uk/conditions/coronavirus-covid-19/people-at-higher-risk/who-is-at-high-risk-from-coronavirus. |
| [23] | B. Neis, K. Neil, K. Lippel, Mobility in a Pandemic: COVID-19 and the Mobile Labour Force, Working Paper, 2020. |
| [24] | NL Population and Demographics, NL Population and Demographics, 2021. Available from: https://www.statista.com/statistics/463905/canada-real-gross-domestic-product-by-province. |
| [25] |
G. Persad, E. J. Emanuel, S. Sangenito, A. Glickman, S. Phillips, E. A. Largent, Public Perspectives on COVID-19 Vaccine Prioritization, JAMA Netw. Open, 4 (2021), e217943-e217943. https://doi.org/10.1001/jamanetworkopen.2021.7943 doi: 10.1001/jamanetworkopen.2021.7943
|
| [26] | S. Premji, A virus that doesn't discriminate? 2021. Available from: https://www.onthemovepartnership.ca/a-virus-that-doesnt-discriminate. |
| [27] |
T. W. Russell, J. T. Wu, S. Clifford, W. J. Edmunds, A. J. Kucharski, M. Jit, et al., Effect of internationally imported cases on internal spread of COVID-19: a mathematical modelling study, The Lancet Public Health, 6 (2021), e12-e20. https://doi.org/10.1016/S2468-2667(20)30263-2 doi: 10.1016/S2468-2667(20)30263-2
|
| [28] | Statistica, Population estimates for Newfoundland and Labrador, Canada from 2000 to 2020, 2021. Available from: https://www.statista.com/statistics/569858/population-estimates-newfoundland-and-labrador-canada. |
| [29] | M. Voysey, S. A. C. Clemens, S. A. Madhi, L. Y. Weckx, P. M. Folegatti, P. K. Aley, et al., Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: an interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK, The Lancet, 397 (2021), 99-111. http://dx.doi.org/10.1016/S0140-6736(20)32661-1 |
| [30] | J. Wise, COVID-19: New data on Oxford AstraZeneca vaccine backs 12 week dosing interval, 2021. https://doi.org/10.1136/bmj.n326 |
Figures(5) / Tables(1)

Maria M. Martignoni, Proton Rahman, Amy Hurford. Rotational worker vaccination provides indirect protection to vulnerable groups in regions with low COVID-19 prevalence[J]. AIMS Mathematics, 2022, 7(3): 3988-4003. doi: 10.3934/math.2022220







 DownLoad:
DownLoad: