Caregiver stress negatively in uences both patients and caregivers. Predictors of caregiver diffculty may provide crucial insights for providers to prioritize those with the highest risk of stress. The purpose of this study was to develop a prediction model of caregiver di culty by applying data mining techniques to a national behavioral risk factor data set.
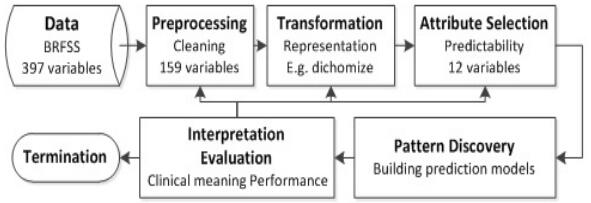
Behavioral data including 397 variables on 2,264 informal caregivers, who provided any care to a friend or family member during the past month, were extracted from a publicly available national dataset in the U.S (N = 451,075) and analyzed. We applied several classi cation algorithms (J48, RandomForest, MultilayerPerceptron, AdaboostM1), to iteratively generate prediction models for caregiving diffculty with 10-fold cross validation.
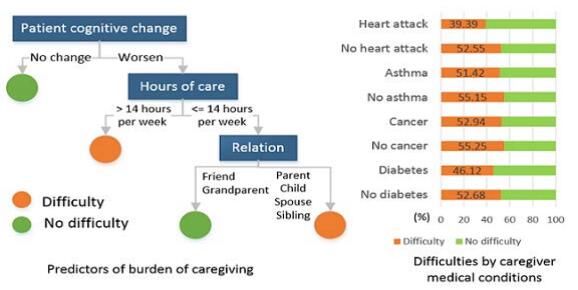
44.7% of informal caregivers answered that they faced the greatest diffculties while they took care of patients. Among those who faced the greatest di culties, the reasons were creating emotional burden (45%). Patient cognitive alteration (e.g. cognitive changes in thinking or remembering during the past year), care hours, and relationship with a caregiver appeared as the main predictors of caregiver stress (classified correctly 63%, diffculty AUC = 65%, no diffculty AUC = 65%).
Data mining methods were useful to discover new behavioral risk knowledge and to visualize predictors of caregiver stress from a multidimensional behavioral dataset.This study suggests that health professionals target dementia family caregivers who are anticipated to experience patients neuro-cognitive changes, and inform the caregivers about importance of limiting care hours, burn out and delegation of caregiving tasks.
Citation: Sunmoo Yoon, Maria Patrao, Debbie Schauer, Jose Gutierrez. Prediction Models for Burden of Caregivers Applying Data Mining Techniques[J]. Big Data and Information Analytics, 2017, 2(3): 209-217. doi: 10.3934/bdia.2017014
Caregiver stress negatively in uences both patients and caregivers. Predictors of caregiver diffculty may provide crucial insights for providers to prioritize those with the highest risk of stress. The purpose of this study was to develop a prediction model of caregiver di culty by applying data mining techniques to a national behavioral risk factor data set.
Behavioral data including 397 variables on 2,264 informal caregivers, who provided any care to a friend or family member during the past month, were extracted from a publicly available national dataset in the U.S (N = 451,075) and analyzed. We applied several classi cation algorithms (J48, RandomForest, MultilayerPerceptron, AdaboostM1), to iteratively generate prediction models for caregiving diffculty with 10-fold cross validation.
44.7% of informal caregivers answered that they faced the greatest diffculties while they took care of patients. Among those who faced the greatest di culties, the reasons were creating emotional burden (45%). Patient cognitive alteration (e.g. cognitive changes in thinking or remembering during the past year), care hours, and relationship with a caregiver appeared as the main predictors of caregiver stress (classified correctly 63%, diffculty AUC = 65%, no diffculty AUC = 65%).
Data mining methods were useful to discover new behavioral risk knowledge and to visualize predictors of caregiver stress from a multidimensional behavioral dataset.This study suggests that health professionals target dementia family caregivers who are anticipated to experience patients neuro-cognitive changes, and inform the caregivers about importance of limiting care hours, burn out and delegation of caregiving tasks.

| [1] |
R. D. Adelman, L. L. Tmanova, D. Delgado, S. Dion and M. S. Lachs, Caregiver burden: A clinical review, Jama, 311 (2014), 1052-1060. doi: 10.1001/jama.2014.304

|
| [2] |
A. Barfar and B. Padmanabhan, Predicting presidential election outcomes from what people watch, Big Data, 5 (2017), 32-41. doi: 10.1089/big.2017.0013
|
| [3] |
C. M. Bishop, Neural Networks for Pattern Recognition, Oxford university press, 1995. MR1385195 |
| [4] | L. Breiman, Random forests, Machine learning, 45 (2001), 5-32. |
| [5] |
C.-Y. Chiao, H.-S. Wu and C.-Y. Hsiao, Caregiver burden for informal caregivers of patients with dementia: A systematic review, International nursing review, 62 (2015), 340-350. doi: 10.1111/inr.12194
|
| [6] |
G. DePalma, H. Xu, K. E. Covinsky, B. A. Craig, E. Stallard, J. Thomas III and L. P. Sands, Hospital readmission among older adults who return home with unmet need for ADL disability, The Gerontologist, 53 (2013), 454-461. doi: 10.1093/geront/gns103
|
| [7] | C. for Disease Control and Prevention, Behavioral risk factor surveillance system survey data, atlanta, georgia. u. s. |
| [8] |
J. E. Gaugler, D. L. Roth, W. E. Haley and M. S. Mittelman, Can counseling and support reduce burden and depressive symptoms in caregivers of people with Alzheimer's disease during the transition to institutionalization? results from the new york university caregiver intervention study, Journal of the American Geriatrics Society, 56 (2008), 421-428. doi: 10.1111/j.1532-5415.2007.01593.x
|
| [9] |
P. E. Greenberg and H. G. Birnbaum, The economic burden of depression in the us: Societal and patient perspectives, Expert opinion on pharmacotherapy, 6 (2005), 369-376. doi: 10.1517/14656566.6.3.369
|
| [10] |
S. Gupta, G. Hawker, A. Laporte, R. Croxford and P. Coyte, The economic burden of disabling hip and knee osteoarthritis (oa) from the perspective of individuals living with this condition, Rheumatology, 44 (2005), 1531-1537. doi: 10.1093/rheumatology/kei049
|
| [11] |
M. Hall, E. Frank, G. Holmes, B. Pfahringer, P. Reutemann and I. H. Witten, The weka data mining software: An update, ACM SIGKDD explorations newsletter, 11 (2009), 10-18. doi: 10.1145/1656274.1656278
|
| [12] |
Y. LeCun, Y. Bengio and G. Hinton, Deep learning, Nature, 521 (2015), 436-444. doi: 10.1038/nature14539
|
| [13] |
S. J. Lupien, B. S. McEwen, M. R. Gunnar and C. Heim, Effects of stress throughout the lifespan on the brain, behaviour and cognition, Nature reviews neuroscience, 10 (2009), 434-445. doi: 10.1038/nrn2639
|
| [14] | P. C. J. Navas, Y. C. G. Parra and J. I. R. Molano, Big data tools: Haddop, mongodb and weka, in International Conference on Data Mining and Big Data, Springer, 2016,449-456. |
| [15] | U. D. of Health and Human Service., 2011 poverty guideline, Federal Register, 76 (2010), 3637-3638. |
| [16] |
B. D. Ripley, Pattern Recognition and Neural Networks, Cambridge university press, 2007. MR2451352 |
| [17] |
J. W. Rowe, T. Fulmer and L. Fried, Preparing for better health and health care for an aging population, Jama, 316 (2016), 1643-1644. doi: 10.1001/jama.2016.12335
|
| [18] |
J. Schmidhuber, Deep learning in neural networks: An overview, Neural networks, 61 (2015), 85-117. doi: 10.1016/j.neunet.2014.09.003
|
| [19] |
B. C. Spillman and S. K. Long, Does high caregiver stress predict nursing home entry?, INQUIRY: The Journal of Health Care Organization, Provision, and Financing, 46 (2009), 140-161. doi: 10.5034/inquiryjrnl_46.02.140
|
| [20] |
C. H. Van Houtven, S. D. Ramsey, M. C. Hornbrook, A. A. Atienza and M. van Ryn, Economic burden for informal caregivers of lung and colorectal cancer patients, The oncologist, 15 (2010), 883-893. doi: 10.1634/theoncologist.2010-0005
|
| [21] | I. H. Witten, E. Frank, M. A. Hall and C. J. Pal, Data Mining: Practical Machine Learning Tools and Techniques, Morgan Kaufmann, 2016. |
| [22] |
X. Wu, V. Kumar, J. Ross Quinlan, J. Ghosh, Q. Yang, H. Motoda, G. J. McLachlan, A. Ng, B. Liu and P. S. Yu et al., Top 10 algorithms in data mining, Knowledge and information systems, 14 (2008), 1-37. doi: 10.1007/s10115-007-0114-2
|
| [23] |
E. Yan and T. Kwok, Abuse of older Chinese with dementia by family caregivers: An inquiry into the role of caregiver burden, International journal of geriatric psychiatry, 26 (2011), 527-535. doi: 10.1002/gps.2561
|
| [24] |
Q. Yang and X. Wu, 10 challenging problems in data mining research, International Journal of Information Technology & Decision Making, 5 (2006), 597-604. doi: 10.1142/S0219622006002258
|
Figures(2) / Tables(2)

Sunmoo Yoon, Maria Patrao, Debbie Schauer, Jose Gutierrez. Prediction Models for Burden of Caregivers Applying Data Mining Techniques[J]. Big Data and Information Analytics, 2017, 2(3): 209-217. doi: 10.3934/bdia.2017014









 DownLoad:
DownLoad: