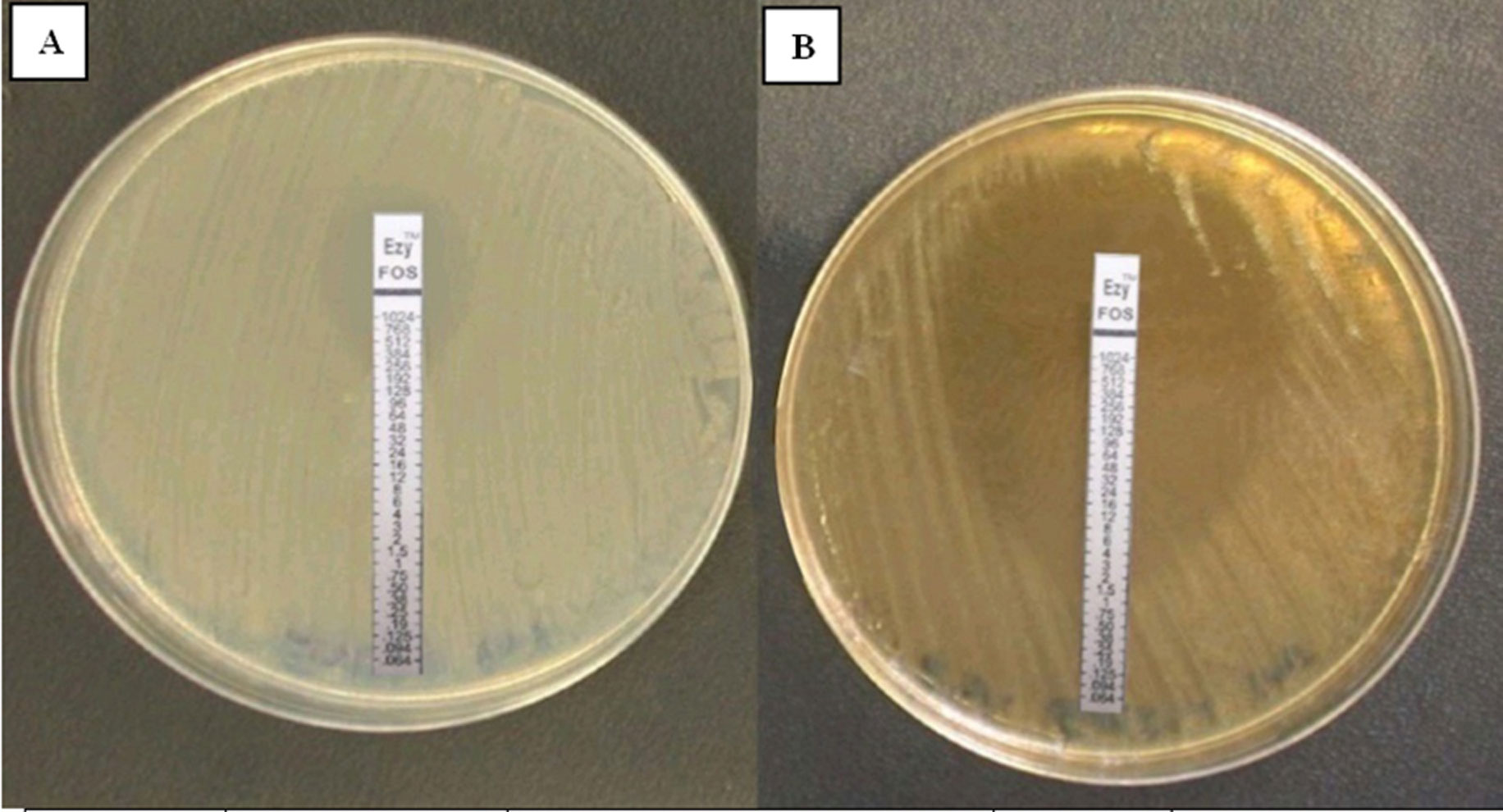
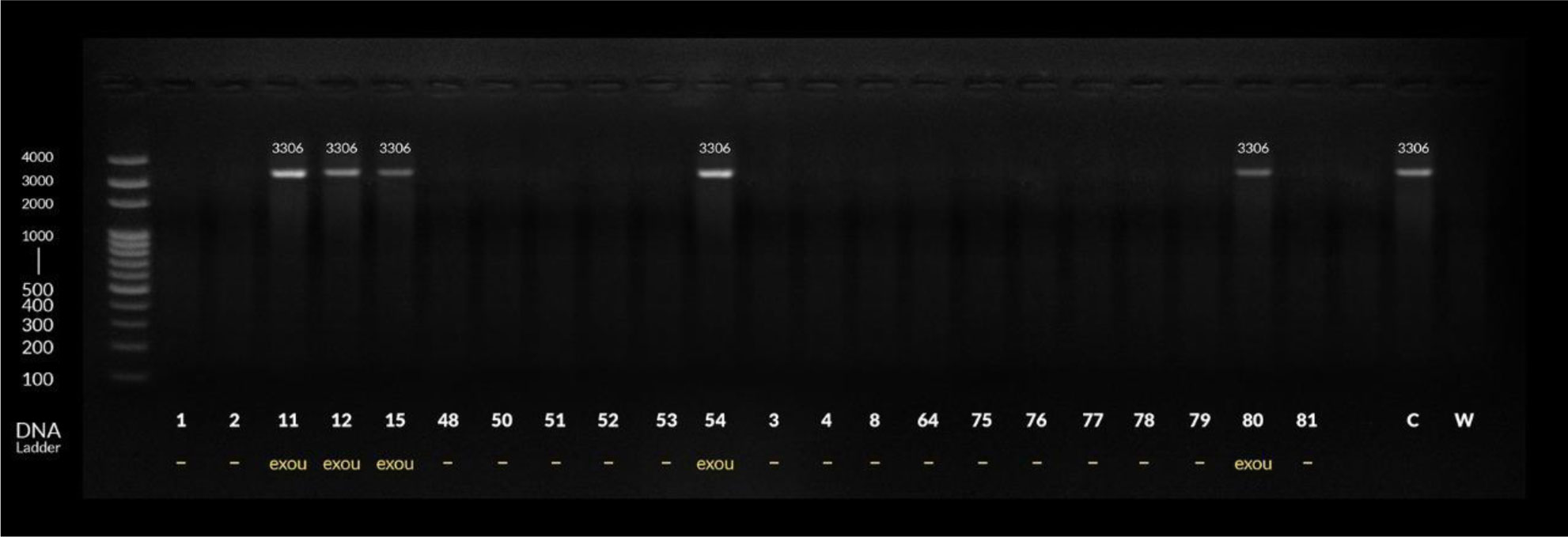
Infections with Pseudomonas aeruginosa (P. aeruginosa) have become a real fear in hospital-acquired infections, especially in critically ill and immunocompromised patients. Thus, advance of novel anti-infectives is currently pursued. The aim of the present study was to evaluate the antibacterial effect of each of citrus honey and fosfomycin in comparison to the combined effect of both of them on multidrug resistant (MDR) P. aeruginosa. 50 MDR P. aeruginosa isolates were tested for the antibacterial effect of citrus honey. Screening for potential synergistic activity of fosfomycin and honey combinations by E test. Molecular detection of the virulent exoenzyme U (exoU) genotype by conventional PCR was done. The present study found that 50 % (v/v) concentration of citrus honey was sufficient to inhibit the growth of most isolates (33/50, 66%). Minimal inhibitory concentration (MIC) for fosfomycin tested by E test was found to be >128 µg/mL in 50(100%) of MDR P. aeruginosa isolates but after repeating E test with Mueller-Hinton agar (MHA) containing sublethal concentration of citrus honey (29/50,58%) isolates were sensitive. Also, there was a significant correlation between the presence of exoU gene and positive synergy of citrus honey-fosfomycin combination. This study showed that citrus honey has antibacterial effect and synergy with fosfomycin antibiotic against MDR P. aeruginosa isolates. Also, exoU positive genotype is associated with MDR phenotype. In conclusion, our results revealed that the citrus honey-fosfomycin combination showed highly statistically significant effect on MDR P. aeruginosa fosfomycin susceptibility pattern. exoU positive P. aeruginosa isolates were detected mostly in burn unit and ICUs. Also, there was a statistically significant correlation between the presence of exoU gene and positive result of honey-fosfomycin combination E test.
Citation: Amira Saied M Abdelhady, Nebal Medhat Darwish, Safaa M. Abdel-Rahman, Nagwa M Abo El Magd. The combined antimicrobial activity of citrus honey and fosfomycin on multidrug resistant Pseudomonas aeruginosa isolates[J]. AIMS Microbiology, 2020, 6(2): 162-175. doi: 10.3934/microbiol.2020011
Infections with Pseudomonas aeruginosa (P. aeruginosa) have become a real fear in hospital-acquired infections, especially in critically ill and immunocompromised patients. Thus, advance of novel anti-infectives is currently pursued. The aim of the present study was to evaluate the antibacterial effect of each of citrus honey and fosfomycin in comparison to the combined effect of both of them on multidrug resistant (MDR) P. aeruginosa. 50 MDR P. aeruginosa isolates were tested for the antibacterial effect of citrus honey. Screening for potential synergistic activity of fosfomycin and honey combinations by E test. Molecular detection of the virulent exoenzyme U (exoU) genotype by conventional PCR was done. The present study found that 50 % (v/v) concentration of citrus honey was sufficient to inhibit the growth of most isolates (33/50, 66%). Minimal inhibitory concentration (MIC) for fosfomycin tested by E test was found to be >128 µg/mL in 50(100%) of MDR P. aeruginosa isolates but after repeating E test with Mueller-Hinton agar (MHA) containing sublethal concentration of citrus honey (29/50,58%) isolates were sensitive. Also, there was a significant correlation between the presence of exoU gene and positive synergy of citrus honey-fosfomycin combination. This study showed that citrus honey has antibacterial effect and synergy with fosfomycin antibiotic against MDR P. aeruginosa isolates. Also, exoU positive genotype is associated with MDR phenotype. In conclusion, our results revealed that the citrus honey-fosfomycin combination showed highly statistically significant effect on MDR P. aeruginosa fosfomycin susceptibility pattern. exoU positive P. aeruginosa isolates were detected mostly in burn unit and ICUs. Also, there was a statistically significant correlation between the presence of exoU gene and positive result of honey-fosfomycin combination E test.

| [1] |
Walsh CC, McIntosh MP, Peleg AY, et al. (2015) In vitro pharmacodynamics of fosfomycin against clinical isolates of Pseudomonas aeruginosa. J Antimicrob Chemother 70: 3042-3050. doi: 10.1093/jac/dkv221

|
| [2] |
Subedi D, Vijay A K, Kohli G S, et al. (2018) Association between possession of exoU and antibiotic resistance in Pseudomonas aeruginosa. PLoS One 13: e0204936. doi: 10.1371/journal.pone.0204936
|
| [3] |
Hassuna NA (2016) Molecular Detection of the virulent exoU genotype of Pseudomonas aeruginosa isolated from infected surgical incisions. Surg Infect 17: 610-614. doi: 10.1089/sur.2016.065
|
| [4] |
Horna G, Amaro C, Palacios A, et al. (2019) High frequency of the exoU+/exoS+ genotype associated with multidrug-resistant ‘high-risk clones’ of Pseudomonas aeruginosa clinical isolates from Peruvian hospitals. Sci Rep 9: 10874. doi: 10.1038/s41598-019-47303-4
|
| [5] |
Cheesman MJ, Ilanko A, Blonk B, et al. (2017) Developing new antimicrobial therapies: Are synergistic combinations of plant extracts/compounds with conventional antibiotics the solution? Pharmacogn Rev 11: 57-72. doi: 10.4103/phrev.phrev_21_17
|
| [6] |
Wasihun AG, Kasa BG (2016) Evaluation of antibacterial activity of honey against multidrug resistant bacteria in Ayder referral and teaching hospital, Northern Ethiopia. Springerplus 5: 842. doi: 10.1186/s40064-016-2493-x
|
| [7] |
Matthew EF, Evridiki KV, George S, et al. (2016) Fosfomycin. Clin Microbiol Rev 29: 321-347. doi: 10.1128/CMR.00068-15
|
| [8] |
Jenkins R, Cooper R (2012) Improving antibiotic activity against wound pathogens with manuka honey in vitro. PLoS One 7: e45600. doi: 10.1371/journal.pone.0045600
|
| [9] | (2018) Clinical and Laboratory Standards Institute (CLSI)Performance Standards for Antimicrobial Susceptibility Testing. CLSI supplement M100 . Wayne, PA: . Available from: http://file.qums.ac.ir/repository/mmrc/CLSI-2018-M100-S28.pdf |
| [10] |
Sweeney MT, Lubbers BV, Schwarz S, et al. (2018) Applying definitions for multidrug resistance, extensive drug resistance and pandrug resistance to clinically significant livestock and companion animal bacterial pathogens. J Antimicrob Chemother 73: 1460-1463. doi: 10.1093/jac/dky043
|
| [11] |
Zhu H, Bandara R, Conibear TC, et al. (2004) Pseudomonas aeruginosa with lasI quorum-sensing deficiency during corneal infection. Invest Ophthalmol Vis Sci 45: 1897-1903. doi: 10.1167/iovs.03-0980
|
| [12] |
Finnan S, Morrissey JP, O'Gara F, et al. (2004) Genome diversity of Pseudomonas aeruginosa isolates from cystic fibrosis patients and the hospital environment. J Clin Microbiol 42: 5783-5792. doi: 10.1128/JCM.42.12.5783-5792.2004
|
| [13] | Kacaniova M, Vukovic N, Bobkova A, et al. (2011) Antimicrobial and antiradical activity of Slovakian honeydew honey samples. J Microbiol Biotech Food Sci 1: 354-360. |
| [14] | The European Committee on Antimicrobial Susceptibility Testing (EUCAST) (2018) Breakpoint tables for interpretation of MICs and zone diameters. Version 8.0.Available from: http://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Breakpoint_tables/v_8.0_Breakpoint_Tables.pdf. |
| [15] |
Santajit S, Indrawattana N (2016) Mechanisms of antimicrobial resistance in ESKAPE pathogens. Biomed Res Int 2016: 2475067. doi: 10.1155/2016/2475067
|
| [16] |
Hashem H, Hanora A, Abdalla S, et al. (2016) Carbapenem susceptibility and multidrug resistance in Pseudomonas aeruginosa isolates in Egypt. Jundishapur J Microbiol 9: e30257. doi: 10.5812/jjm.30257
|
| [17] | Al-Haik WM, Al-Mahbash AA, Al-Mahdi AY, et al. (2016) Genotypic characteristics of clinical and non-clinical isolates of Pseudomonas aeruginosa: distribution of different antibiogram profiles and molecular typing. Jordan J Biol Sci 9: 185-194. |
| [18] | Bashir D, Thokar M A, Fomda B A, et al. (2011) Detection of metallo-beta-lactamase (MBL) producing Pseudomonas aeruginosa at a tertiary care hospital in Kashmir. Afr J Microbiol Res 5: 164-172. |
| [19] |
Raman G, Avendano EE, Chan J, et al. (2018) Risk factors for hospitalized patients with resistant or multidrug-resistant Pseudomonas aeruginosa infections: a systematic review and meta-analysis. Antimicrob Resist Infect Control 7: 79. doi: 10.1186/s13756-018-0370-9
|
| [20] |
Polotto M, Casella T, de Lucca Oliveira M G, et al. (2012) Detection of P. aeruginosa harboring bla CTX-M-2, bla GES-1 and bla GES-5, bla IMP-1 and bla SPM-1 causing infections in Brazilian tertiary-care hospital. BMC Infect Dis 12: 176. doi: 10.1186/1471-2334-12-176
|
| [21] | Kamel GM, Ezzeldeen NA, El-Mishad M Y, et al. (2011) Susceptibility pattern of Pseudomonas aeruginosa against antimicrobial agents and some plant extracts with focus on its prevalence in different sources. Global Vet 6: 61-72. |
| [22] |
Mansour S, Eldaly O, Jiman-Fatani A, et al. (2013) Epidemiological characterization of P. aeruginosa isolates of intensive care units in Egypt and Saudi Arabia. East Mediter Health J 19: 71-80. doi: 10.26719/2013.19.1.71
|
| [23] |
Ayatollahi J, YazdiYousefi Y, Shahcheraghi SH (2018) Study of Drug Resistance of Pseudomonas aeruginosa in Yazd, Iran, During 2015–2016. Int J Infect 5: e68749. doi: 10.5812/iji.68749
|
| [24] |
Dash M, Padhi S, Narasimham MV, et al. (2014) Antimicrobial resistance pattern of Pseudomonas aeruginosa isolated from various clinical samples in a tertiary care hospital, South Odisha, India. Saudi J Health Sci 3: 15-19. doi: 10.4103/2278-0521.130200
|
| [25] |
Farhan S, Ibrahim R, Mahran KM, et al. (2019) Antimicrobial resistance pattern and molecular genetic distribution of metallo-β-lactamases producing Pseudomonas aeruginosa isolated from hospitals in Minia, Egypt. Infect Drug Resist 12: 2125-2133. doi: 10.2147/IDR.S198373
|
| [26] |
Raouf MR, Sayed M, Rizk HA, et al. (2018) High incidence of MBL-mediated imipenem resistance among Pseudomonas aeruginosa from surgical site infections in Egypt. J Infect Dev Ctries 12: 520-525. doi: 10.3855/jidc.9936
|
| [27] | Sader HS, Castanheira M, Shortridge D, et al. (2017) Antimicrobial activity of ceftazidime-avibactam tested against multidrug-resistant Enterobacteriaceae and Pseudomonas aeruginosa isolates from U.S. Medical centers, 2013 to 2016. Antimicrob Agents Chemother 61: e01045-17. |
| [28] |
Samad A, Ahmed T, Rahim A, et al. (2017) Antimicrobial susceptibility patterns of clinical isolates of Pseudomonas aeruginosa isolated from patients of respiratory tract infections in a Tertiary Care Hospital, Peshawar. Pak J Med Sci 33: 670-674. doi: 10.12669/pjms.333.12416
|
| [29] |
Kwakman PH, Velde AA, de Boer L, et al. (2011) Two major medical honeys have different mechanisms of bactericidal activity. Plos One 6: e17709. doi: 10.1371/journal.pone.0017709
|
| [30] |
Hussain M B, Hannan A, Akhtar N, et al. (2015) Evaluation of the antibacterial activity of selected Pakistani honeys against multi-drug resistant Salmonella typhi. BMC Complement Altern Med 15: 32. doi: 10.1186/s12906-015-0549-z
|
| [31] |
Hegazi AG (2011) Antimicrobial activity of different Egyptian honeys as comparison of Saudi Arabia honey. Res J Microbiol 6: 488-495. doi: 10.3923/jm.2011.488.495
|
| [32] |
Roby MHH, Abdelaliem YF, Esmail AM, et al. (2020) Evaluation of Egyptian honeys and their floral origins: phenolic compounds, antioxidant activities, and antimicrobial characteristics. Environ Sci Pollut Res Int 27: 20748-20756. doi: 10.1007/s11356-020-08586-7
|
| [33] |
Jantakee K, Tragoolpua Y (2015) Activities of different types of Thai honey on pathogenic bacteria causing skin diseases, tyrosinase enzyme and generating free radicals. Biol Res 48: 4. doi: 10.1186/0717-6287-48-4
|
| [34] | Ahmed M, Sahile S, Subramanian C (2014) Evaluation of antibacterial potential of honey against some common human pathogens in north gondar zone of Ethiopia. Int J Pure Appl Zool 2: 286-295. |
| [35] |
Mandal MD, Mandal S (2011) Honey: its medicinal property and antibacterial activity. Asian Pac J Trop Biomed 1: 154-160. doi: 10.1016/S2221-1691(11)60016-6
|
| [36] |
Wasfi R, Elkhatib WF, Khairalla AS (2016) Effects of selected Egyptian honeys on the cellular ultrastructure and the gene expression profile of Escherichia coli. PloS One 11: e0150984. doi: 10.1371/journal.pone.0150984
|
| [37] |
AL-Waili N, Al Ghamdi A, Ansari MJ, et al. (2013) Differences in composition of honey samples and their impact on the antimicrobial activities against drug multiresistant bacteria and pathogenic fungi. Arch Med Res 44: 307-316. doi: 10.1016/j.arcmed.2013.04.009
|
| [38] |
Behera B, Mohanty S, Sahu S, et al. (2018) In vitro Activity of fosfomycin against Multidrug-resistant urinary and nonurinary Gram-negative isolates. Indian J Crit Care Med 22: 533-536. doi: 10.4103/ijccm.IJCCM_225_18
|
| [39] |
Perdigão-Neto LV, Oliveira MS, Rizek CF, et al. (2014) Susceptibility of multiresistant Gram-negative bacteria to fosfomycin and performance of different susceptibility testing methods. Antimicrob Agents Chemother 58: 1763-1767. doi: 10.1128/AAC.02048-13
|
| [40] |
Maraki S, Samonis G, Rafailidis PI, et al. (2009) Susceptibility of urinary tract bacteria to fosfomycin. Antimicrob Agents Chemother 53: 4508-4510. doi: 10.1128/AAC.00721-09
|
| [41] |
Jayaraman P, Sakharkar MK, Lim CS, et al. (2010) Activity and interactions of antibiotic and phytochemical combinations against Pseudomonas aeruginosa in vitro. Int J BiolSci 6: 556-568. doi: 10.7150/ijbs.6.556
|
| [42] |
Ejim L, Farha MA, Falconer SB, et al. (2011) Combinations of antibiotics and nonantibiotic drugs enhance antimicrobial efficacy. Nat Chem Biol 7: 348-350. doi: 10.1038/nchembio.559
|
| [43] |
Khan F, Hill J, Kaehler S, et al. (2014) Antimicrobial properties and isotope investigations of South African honey. J Appl Microbiol 117: 366-379. doi: 10.1111/jam.12533
|
| [44] | Ruiz Ramos J, Salavert Lletí M (2019) fosfomycin in infections caused by multidrug-resistant Gram-negative pathogens. Rev Esp Quimioter 32: 45-54. |
| [45] |
Vardakas KZ, Legakis NJ, Triarides N, et al. (2016) Susceptibility of contemporary isolates to fosfomycin: a systematic review of the literature. Int J Antimicrob Agents 47: 269-285. doi: 10.1016/j.ijantimicag.2016.02.001
|
| [46] |
Sastry S, Clarke LG, Alrowais H, et al. (2015) Clinical Appraisal of fosfomycin in the era of antimicrobial resistance. Antimicrob Agents Chemother 59: 7355-7361. doi: 10.1128/AAC.01071-15
|
| [47] |
Peña C, Cabot G, Gómez-Zorrilla S, et al. (2015) Influence of virulence genotype and resistance profile in the mortality of Pseudomonas aeruginosa bloodstream infections. Clin Infect Dis 60: 539-548. doi: 10.1093/cid/ciu866
|
| [48] |
Bradbury RS, Roddam LF, Merritt A, et al. (2010) Virulence gene distribution in clinical, nosocomial and environmental isolates of Pseudomonas aeruginosa. J Med Microbiol 59: 881-890. doi: 10.1099/jmm.0.018283-0
|
| [49] |
Mitov I, Strateva T, Markova B (2010) Prevalence of virulence genes among Bulgarian nosocomial and cystic fibrosis isolates of Pseudomonas aeruginosa. Braz J Microbiol 41: 588-595. doi: 10.1590/S1517-83822010000300008
|
| [50] |
Kainuma A, Momiyama K, Kimura T, et al. (2018) An outbreak of fluoroquinolone-resistant Pseudomonas aeruginosa ST357 harboring the exoU gene. J Infect Chemother 24: 615-622. doi: 10.1016/j.jiac.2018.03.008
|
Figures(2) / Tables(7)

Amira Saied M Abdelhady, Nebal Medhat Darwish, Safaa M. Abdel-Rahman, Nagwa M Abo El Magd. The combined antimicrobial activity of citrus honey and fosfomycin on multidrug resistant Pseudomonas aeruginosa isolates[J]. AIMS Microbiology, 2020, 6(2): 162-175. doi: 10.3934/microbiol.2020011







 DownLoad:
DownLoad: